urinary incontinence symptoms
advertisement

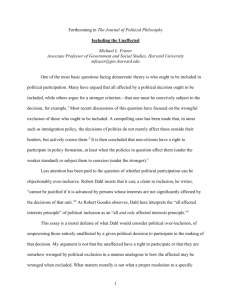
Hollis Herman DPT, PT, IF, OCS, WCS, BCB-PMD Doctor of Physical Therapy | Women's and Men's Health Board Certified Orthopedic, Women’s Health, Biofeedback Specialist, ISSWSH Fellow 675 Massachusetts Ave. 5th Fl. | Cambridge, MA 02139 p. 617-576-3204 | f. 1-617-497-1565 | contact@hollyherman.com PELVIC EVALUATION – PAGE 1 PLEASE FILL OUT and BRING WITH YOU to your first appointment (submitting electronically is also acceptable). PATIENT NAME: DATE: ADDRESS: DATE OF BIRTH: OCCUPATION: AGE: DR/REFERRAL: CHIEF COMPLAINT: DIAGNOSIS: DATE OF LAST PELVIC/PROSTATE EXAM: DATE OF URINALYSIS: RESULTS: Neg Pos BLADDER WAS THERE AN EVENT ASSOCIATED WITH ONSET OF URINARY COMPLAINTS?: URINE STREAM: EMPTYING: Easy to Start Complete Strong Incomplete Weak FREQUENCY OF URINATION: During awake hours? URINARY SENSATION PRESENT: Starts & Stops Pushing or straining needed Yes Variable WHAT IS THE AVERAGE VOLUME OF URINATION?: 1-4oz Yes During Sleep Hours? # times per night 8-16oz minutes, hours FLUID INTAKE: # of 8 oz glasses per day HOW MANY CUPS OF TEA/COFFEE PER DAY? CAN YOU STOP YOUR URINE ONCE STARTED?: PAIN WITH URINATION?: Deflects to one side CAN YOU HOLD BACK YOUR URINE?: 4-8oz HOW MANY OUNCES PER DAY IS WATER?: Yes. Please describe: Other # times per day No None Complete Deflects No Unable OTHER: None ANY DRIBBLING AFTER URINATION?: Yes. Explain:: Yes No BOWEL WAS THERE AN EVENT ASSOCIATED WITH ONSET OF BOWEL COMPLAINTS?: BOWEL SENSATION PRESENT?: Yes No FREQUENCY OF BOWEL MOVEMENTS: EVACUATION HABITS: LAXATIVE USE: None None Variable # times per day, Straining Splinting None Yes. Please describe: CAN YOU HOLD BACK YOUR FECES IF NO BATHROOM IS AROUND?: minutes, hours # times per week Other Explain: Yes. How often per week? ANY BLOOD ON TISSUE AFTER BOWEL MOVEMENT?: Yes URINARY INCONTINENCE SYMPTOMS URINARY LEAKAGE: CAUSE: None # episodes per Day Week Month Yes. Explain: URINE LEAKAGE AMOUNT: DO YOU WEAR A PAD?: None No Few Drops Yes Wets Pad Wets Underwear What kind?: Wets Outerwear # PAD CHANGES REQUIRED IN 24 HOURS: FECAL INCONTINENCE SYMPTOMS FECAL LEAKAGE: # episodes per FECAL LEAKAGE AMOUNT: FORM OF PROTECTION: KC4HL PELVIC EVALUATION 10/30/2010 None None Day Smear Week Month Diarrhea Yes. What type of pad?: CAUSE: Few “Pebbles” None Yes. Explain: Full Stool # PAD CHANGES REQUIRED IN 24 HOURS: PAGE 1 of 2 No Hollis Herman DPT, PT, IF, OCS, WCS, BCB-PMD Doctor of Physical Therapy | Women's and Men's Health Board Certified Orthopedic, Women’s Health, Biofeedback Specialist, ISSWSH Fellow 675 Massachusetts Ave. 5th Fl. | Cambridge, MA 02139 p. 617-576-3204 | f. 1-617-497-1565 | contact@hollyherman.com PELVIC EVALUATION – PAGE 2 DATE OF BIRTH: PATIENT NAME: DATE: PAIN DESCRIPTION: None Yes. Type of pain?: HOW IS PAIN AFFECTED BY: MOVEMENT: Unaffected REST: Unaffected TIME OF DAY: Stabbing Unaffected Increase BOWEL MOVEMENT: Unaffected VAGINAL PENETRATION: INITIAL PENETRATION: DEEP PENETRATION: Increase Unaffected N/A Decrease Decrease Increase Duration Decrease Duration N/A 2 Pain interrupts or prevents completion N/A N/A Unaffected Unaffected N/A EXERCISE: Decrease Duration: Increase Unaffected 1 Discomfort that does not affect completion LIFTING: Decrease Decrease Decrease Increase Unaffected 0 No problems BENDING: Increase Increase Decrease MARINOFF SCALE – DESCRIPTIVE SCALE OF INTERCOURSE MENSTRUATION: NIGHTTIME: Increase Duration: Unaffected N/A FOLLOWING PENETRATION: AFTERNOON: Decrease Decrease Increase N/A Sharp Decrease Unaffected N/A Prickling Decrease Increase AFTER A BOWEL MOVEMENT: Decrease Increase Increase Increase Unaffected Burning Decrease Type: MORNING: Unaffected BOWEL URGE: Sore Decrease Type of movement?: Increase Type: EVENING: URINATION: Tender Increase Type of movement?: Unaffected FULL BLADDER: Aching Unaffected N/A Increase Increase Unaffected CONTACT WITH CLOTHING: 3 Pain preventing any attempts at intercourse Increase Duration Decrease Decrease Increase Unaffected Decrease Duration Decrease Increase HOW BAD IS YOUR PAIN (10 BEING WORST)?: At best?: Decrease /10 At present?: /10 At worst?: /10 WHAT MAKES YOUR SYMPTONS WORSE? LIFESTYLE / QUALITY OF LIFE / FUNCTIONAL LIMITATIONS SOCIAL ACTIVITIES: Unaffected Yes. Explain: DIET/FLUID INTAKE: Unaffected Yes. Explain: PHYSICAL ACTIVITY: WORK: N/A OTHER (SPECIFY): Unaffected Unaffected N/A Yes. Explain: Yes. Explain: Yes. Explain: PATIENT GOALS: KC4HL PELVIC EVALUATION 10/30/2010 PAGE 2 of 2