BLEEDING PRECAUTIONS
advertisement

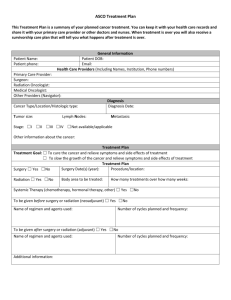
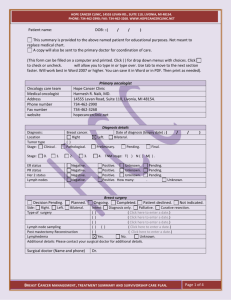
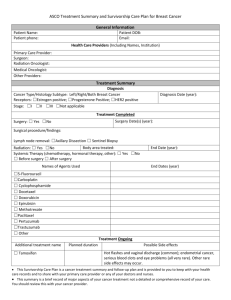
HOPE CANCER CLINIC, 14555 LEVAN RD., SUITE 110, LIVONIA, MI 48154. PHONE: 734-462-2990; FAX: 734-462-3268. WWW.HOPECANCERCLINIC.NET Patient name: DOB: : ( / Date plan was created: ( Click here to enter a date.) purposes. Not meant to replace medical chart. Provider Medical oncologist / ) . This summary is provided for educational Oncology providers Name Harmesh R. Naik, MD., Hope Cancer Clinic 14555 Levan Road, Suite 110, Livonia, MI 48154. Contact information Ph: 734-462-2990 Fax: 734-462-3268 Surgeon Radiation oncologist Primary MD Other Diagnosis: Breast cancer. Location: (choose) Diagnosis details Date of diagnosis (biopsy date) : ( Tumor type (choose) ER status (choose) PR status (choose) Lymph nodes (choose). Number: . / / ) Stage: (choose) . TNM: T( choose ) N (choose) M(choose). Her 2 status (choose) Oncotype DX ( Choose ). Score (Choose). 5 yr risk %. Other: Breast surgery: ( choose ) Side: (choose) Type of surgery (choose) Click here to enter a date.) Lymph node sampling (choose) (choose) ( Click here to enter a date.) Lymphedema (choose) Additional details: Please contact your surgical doctor for additional details. Regimen (choose) Details of regimen (Name and dose ) Chemotherapy: ( choose ) Start date: ( Click here to enter a date.) WBC growth factor (choose) Anthracycline total dose (choose) Start date ( Click here to enter a date.) Side effects : Hair loss. Nausea/Vomiting. Menopause symptoms. Cardiac. Other Additional details / complications / comments: Transfusions (choose) ( mg/m2) End date ( Click here to enter a date.) Neuropathy. Low blood count Fatigue. Trastuzumab (Herceptin) therapy: ( choose ) Start date ( Click here to enter a date.) End date ( Click here to enter a date.) Details : BREAST CANCER MANAGEMENT , TREATMENT SUMMARY AND SURVIVORSHIP CARE PLAN. This template was created by: Harmesh Naik, MD. (2012 short version). Page 1 of 2 HOPE CANCER CLINIC, 14555 LEVAN RD., SUITE 110, LIVONIA, MI 48154. PHONE: 734-462-2990; FAX: 734-462-3268. WWW.HOPECANCERCLINIC.NET Hormonal therapy: ( choose ) Drug: ( choose ) Start date (Click here to enter a date.) Additional details / side effects: End date ( Click here to enter a date.) Radiation therapy: ( choose ) Radiation dose rads Start date ( Click here to enter a date.) End date ( Click here to enter a date.) Additional details / side effects: Please contact your radiation doctor for additional details. Side: (choose) What to watch for: Promptly report any new symptoms: Example symptoms: New lumps, Bone pain, Chest pain, breathing difficult, cough, Abdominal pain, Persistent headaches Weight loss, loss of appetite, Any other symptoms that are not improving, Unexplained symptoms Survivorship care: Suggested follow up care for asymptomatic patients: Based on ASCO guidelines Annually thereafter Medical history/physical exam Every 4 months x 3 years Breast self exam Every 4-6 months years 4-5 Monthly if feasible Genetic counseling Annually or earlier if suggested by radiologist Consider if criteria met Colo-rectal cancer screening Recommended. Pap smear and pelvic exam Recommended. Skin cancer screening Recommended No smoking /smoking cessation Bone density measurement / Oral Calcium and vitamin D Low fat diet Recommended- Do not smoke Recommended. Michigan Tobacco Quit Line: 1-800-784-8669 Contact primary MD. Recommended Nutritional consult Staying active Recommended Fall precautions Report any new symptoms Recommended Mammography (first in six months after RT) Ask your doctor Contact primary MD or Gyn MD. Use sun block in summer. REMEMBER: Please note that the ASCO guidelines apply to patient who are feeling fine and have no symptoms. If you are having any symptoms, then you need to contact your physician for proper testing. Notes: Have fun! Enjoy life! Recommended Ctr + click on http://hopecancerclinic.net/inspirational/fly_a_kite BREAST CANCER MANAGEMENT , TREATMENT SUMMARY AND SURVIVORSHIP CARE PLAN. This template was created by: Harmesh Naik, MD. (2012 short version). Page 2 of 2