Abstract link - Kings airway
advertisement

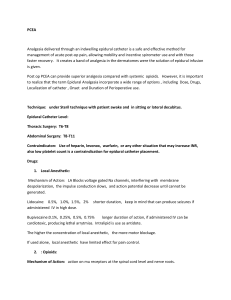
A case of severe thrombocytopenia during pregnancy: diagnostic dilemma and multidisciplinary approach Salota, Vishal; Sharafudeen, Saju; Skelton, Vanessa King's College Hospital, London Thrombocytopenia (platelet count of <100×109/L) is the second most common haematological abnormality during pregnancy1,2 with an incidence of 7-8% of all pregnancies3. Majority of causes are easily understood. However, various aetiologies can make it difficult to diagnose in certain cases. Diagnosis carries importance as this determines outcome based on whether or not a platelet transfusion can be safely carried out. Management requires a multidisciplinary approach. Description A 30 year old healthy primiparous full term woman delivered a healthy baby by assisted ventouse delivery. She had an epidural for pain relief. Estimated blood loss was about 1.2 L. Haemodyamic parameters remained stable and patient was kept in the high dependency unit for further observation. Her antenatal bloods were all normal, Hb 136 g/L and platelet count (PLT) of 148×109/L. Immediately after delivery, inspite of adequate fluid resuscitation, she developed acute kidney injury and haemolysis. Hb at the nadir on day 6 post-partum was 57 g/L with lowest PLT of 16×109/L. Creatinine increased to a peak of 213 µmol/L. Liver enzymes remained normal apart from a modest increase in AST to 87 U/L, elevated lactate dehydrogenase (LDH) levels (peak of 3339 iu/L) with haptoglobin of < 0.1 g/L. Liver and renal ultrasound remained normal. She had blood 3+ and urine protein 2+ in urine dipsticks. Blood film showed numerous red cell fragments. She did not show any neurological symptoms. Following discussion with haematology team, a diagnosis of microangiopathic haemolytic anaemia (MAHA), probably atypical HELLP syndrome (haemolysis, elevated liver enzymes, low platelets) was made. ADAMST-13 test (a disintegrin and metalloproteinase with a thrombospondin type1 motif, member 13) was performed to exclude thrombotic thrombocytopenic purpura (TTP). She received multiple red cell transfusions and a single pool of PLT with little effect. Therapeutic plasma exchanges were subsequently initiated on day 5 post-partum. She underwent four plasma exchanges with excellent response and was discharged on day 12 with recommendation to take ferrous fumarate and folic acid. One week after discharge, her Hb increased to 102 g/L, PLT 338×109/L with normal haptoglobin and LDH levels. She made a complete recovery. Figure 1 Trend of haemoglobin and platelet count during pre and post-partum period Discussion The majority of women with HELLP syndrome have hypertension and proteinuria which may be absent in 10–20% of cases - referred to as atypical HELLP. These patients may present with gastrointestinal, respiratory, or hematologic symptoms risking initial misdiagnosis. Management includes:1. Obstetric management: Treatment is delivery, however, if patient is < 34 weeks gestation corticosteroids can be administered to accelerate fetal lung maturity. Magnesium sulphate (to prevent seizures) and antihypertensives may be required. 2. Hematologic management: Corticosteroids may improve the PLT count.There is no contraindication to PLT transfusion or other blood products. If patient continuous to worsen 48-72 hours postpartum, therapeutic plasma exchange should be considered. References 1. Shehata N, Burrows R, Kelton JG. Gestational thrombocytopenia. Clinical Obstetrics and Gynecology. 1999 Jun; 42(2):327-34. 2. Sullivan CA, Martin JN Jr. Management of the obstetric patient with thrombocytopenia. Clinical Obstetrics and Gynecology. 1995 Sep; 38(3):52134. 3. Kadir RA, Mc Lintock C. Thrombocytopenia and disorders of platelet function in pregnancy. Seminars in Thrombosis and Hemostasis. 2011 Sep;37(6):640-52. 4. Sibai BM. The HELLP Syndrome: much ado about nothing? American Journal of Obstetrics and Gynecology 1990;162:311- 6. 5. Gernsheimer T, James AH, Stasi R, How I treat thrombocytopenia in pregnancy. Blood. 2013;121(1):38-47 Anaesthetic Management of a 13-month-old child with medium chain Acyl CoA dehydrogenase deficiency (MCADD) in a district general hospital. V Salota1,3, R Salota2 and C Chapman1 1 Queen Elizabeth The Queen Mother Hospital, Margate, Kent; 2 St Helier Hospital, Surrey; 3 King’s College Hospital, Denmark Hill, London. Introduction MCADD is an inherited fatty acid oxidation disorder with incidence of 1:10,000 births among Caucasians. Fasting periods are poorly tolerated with risk of serious hypoglycaemia. We report an interesting case of a 13-month-old child with this condition undergoing major orthopaedic surgery. Case description A 13-month-old child with MCADD (weight 11.3 kg) was posted for femoral osteotomy. Considering the high risk of hypoglycaemia, she was admitted night before surgery and was started on intravenous drip of 10% dextrose with 2.25 gm sodium. Oral midazolam was given as premedication. She underwent gas induction with sevoflurane and airway was secured with LMA. Intra-operatively, caudal epidural with 0.25% levo-bupivacaine and clonidine was performed. Anaesthesia was uneventful. Regular blood gas and glucose levels remained within normal limits. The dextrose sodium infusion was continued for further 9 hours until normal feeding was commenced. Blood glucose was monitored for 6 hours. She was discharged home following day, on regular paracetamol and ibuprofen. . Discussion Fatty acid beta-oxidation provides energy after the body has used up its stores of glucose and glycogen. Defective oxidation of fatty acid in MCADD patients results in inability to switch to fatty acid metabolism during periods of starvation or increased requirement hence continued metabolism of glucose ultimately lead to profound hypoglycaemia.1 Lack of acetyl CoA also affects hepatic ketogenesis. Clinically, MCADD patients may present with lethargy, seizures, coma and hypoketotic hypoglycemia, particularly triggered by a minor illness; acute liver disease and hepatomegaly which can lead to a misdiagnosis of Reye syndrome. In some individuals, the only manifestation of MCADD is sudden, unexplained death often preceded by a minor illness that would not usually be fatal. Goal of anaesthesia therefore, is to minimise ongoing energy requirements by reducing stress while providing adequate calories in the form of carbohydrate. This was achieved by using premedication, gas induction rather than repeated cannulation, avoiding intubation and caudal block with clonidine. Adequate provision for their particular metabolic needs would allow to safely undertake major procedures even outside the tertiary centres. References 1. Ewout JH,Geany D,Robb M,Mitchell L, Bohn H, Bohn D , Paediatrics 2004;113;1279 Brainstem Anaesthesia Presenting as a Fifth and Seventh Cranial Nerve Palsy Following a Peribulbar Nerve Block for Cataract and Glaucoma Surgery Strowbridge S, Milroy S. Department of Anaesthesia, Kings College Hospital, UK March 2015 Ophthalmic blocks are safe and effective options for eye surgery. The safety profile of ‘blunt needle’ subtenon blocks is preferable. However, for complex ophthalmic surgery such as trabeculectomy and gas injection, the peribulbar block (PB) provides dense and reliable akinesis and analgesia. These techniques should only be performed after discussion with the surgical team and patient assessment. Brainstem anaesthesia is a serious but recognised complication of these techniques. We present a case of fifth and seventh cranial nerve blockade after performing a PB for ophthalmic surgery. An ASA 2, 61year old female presented for cataract phacoemulsification, lens implantation and goniosynechialysis. Preoperative assessment was unremarkable. Optometry revealed normal axial length but elevated intraocular pressure, treated with intravenous acetazolamide. A PB was performed with local anaesthetic (2% lignocaine & 0.5% bupivacaine) and 150i.u hyaluronidase. 7mls was injected via a transdermal approach inferolaterally. The patient developed immediate, transient agitation lasting for approximately 10 seconds. She remained haemodynamically stable. No ptosis or akinesia was noted, and a further 3ml medial canthus top up was administered. Post-procedure, the patient developed features consistent with an ipsilateral motor facial nerve and sensory trigeminal nerve distribution palsy. Haemodynamic and respiratory parameters remained stable. Surgery was expedited and completed uneventfully. 3 hours postoperatively, the neurological deficits had resolved fully. Further review on day 1 postoperatively was unremarkable. Although rare, brainstem anaesthesia is a recognised complication of PB. These techniques should be performed by an experienced practitioner, with intravenous access, monitoring and the facility to provide ventilatory and haemodynamic support. References for poster 1. Carneiro H, Oliveira B, Ávila M, Neto O, Brainstem Anesthesia after Extraconal Retrobulbar block. Can it be avoided? Case report. Rev Bras Anestesiol 2007;57(4):391-400. 2. Loken R, Mervyn Kirker GE, Hamilton RC: Respiratory arrest following peribulbar anesthesia for cataract surgery: Case report and review of the literature. Can J Ophthalmol 1998;33:225-226. 3. Roman SJ, Chong Sit DA, Boureau CM, Auclin FX, Ullern MM: Sub-Tenon's anaesthesia: an efficient and safe technique. Br J Ophthalmol 1997;81:673–676. 4. Singer SB, Preston R, Hodge WG: Respiratory arrest following peribulbar anesthesia for cataract surgery: Case report and review of literature. Can J Ophthalmol 1997;32:450-454. Are we achieving recommended targets with labour analgesia: what happens after 2 hours of epidural use and how to improve? Salota, Vishal; Sharafudeen, Saju; Fleming, Ian; Skelton, Vanessa King's College Hospital, London PCEA is a widely accepted technique for labour pain relief. We currently use a bolus only regime with plain bupivacaine (0.1%) and fentanyl (2mcg/L). 8 mL boluses are delivered every 20 minutes using GemStar™ infusion systems (GIS). RCoA recommendations include re-siting or alternative form of analgesia if epidural fails to provide pain relief within 45 minutes. Patient satisfaction ≥ 98% is considered acceptable1. Our previously presented audit showed significant motor blockade and less breakthrough pain with a background only regime in 20102. We audited the quality of analgesia after 2 hours of initiation of our bolus only protocol and compared the results with the prevoius outcomes. Methods King’s College Hospital is a teaching hospital with 7000 deliveries. After internal governance approval, we included consecutive 52 patients who had epidural for labour pain relief over a period of 3 weeks. Patients with epidurals for less than 2 hours were excluded. We looked at incidence and frequency of breakthrough pain, unilateral motor block, use of other mode of pain relief and requests for manual top-ups. Patient satisfaction was assessed using a NRS of 0-10. Results All patients experienced good pain relief following initial manual bolus of 15ml low dose mixture. 26.9% patients experienced breakthrough pain, 23% requiring 1 or more manual top-ups after 2 hours. 91.6% manual top-ups were delivered within 30 minutes of the request. 13.4% patients had dense motor block (modified Bromage scale). Only 92% patients experienced satisfactory or above pain relief. Figure 1 Comparison of breakthrough pain & motor blockade with background infusion & bolus only regime. Discussion Bolus only regimes are known for higher incidence of breakthrough pain compared to those with background infusions. However, background infusions cause significant motor blockade. Factors which may contribute to the increased incidence of breakthrough pain include lateral positioning, low pressure boluses delivered by pumps, or delay in the request for the bolus. Recently, MHRA has issued a medical device alert related to GIS 3. These faults may lead to under performances of the pump such as over-infusion, under infusion or calibration errors3. Our audit showed a significant proportion of patients experienced breakthrough pain after initial loading dose. This had an impact on satisfaction scores. However, we still achieve a significantly less motor blockade with the bolus only regime. Our unit is currently considering an alternative epidural pump which can deliver bolus with higher pressure (350-1100 mmHg), which is adjustable. We will re-audit the performance of new device. References 1. Royal College of Anaesthetists - Raising the Standard: a compendium of audit recipes - 3rd Edition 2012. 2. Sharafudeen, S.; Barry, A.; Nicholson, C.; Skelton, V.; Fleming, I. PCEA labour analgesia: Are we better with or without background infusion? European Journal of Anaesthesiology:12 June 2010 - Volume 27 - Issue 47 - p 163-164 Obstetric Anaesthesia. 3. Medicines & Healthcare products Regulatory Agency: (Hospira) Due to pump faults. (MDA/2013/016). Safe combined spinal epidural for a patient with Takayasu’s arteritis for elective Caesarean section Esprit S.A1 & Kirby S2. 1. Obstetric anaesthesia fellow, 2. Consultant Anaesthetist Queen Charlotte’s Hospital, London Takayasu's arteritis (TA) is a rare chronic progressive panendarteritis involving the aorta and its main branches (1) often complicated by severe uncontrolled hypertension, with end-organ dysfunction, and stenosis of major blood vessels affecting regional circulation (1). It is vital to control the blood pressure of such patients because TA is often associated with arterial aneurysms, which may rupture when exposed to high blood pressure and cerebral dysfunction (2), so low blood pressure may lead to cerebral ischaemia. The sympathetic block that occurs with regional anaesthesia may result in hypotension, however it is easier to monitor cerebral function in awake patients (2) and regional anaesthesia is the preferred technique in pregnant women. Description A 27year old woman, who had been diagnosed with TA three years earlier, presented for elective Caesarean section at 38weeks' gestation in a spontaneous pregnancy. During the pregnancy she had been experiencing worsening chest pain and claudication in all four limbs, with left upper limb pulses unpalpable on examination. Recent CT scans had revealed left subclavian artery stenosis, coeliac axis stenosis, aortitis and thickening of the aortic arch up to the left subclavian artery and pulmonary artery inflammation. A trans-thoracic echocardiogram revealed good biventricular systolic function and no valvular heart disease. The disease process was controlled with azathioprine and prednisiolone. A combined spinalepidural was performed at L3/4 space with a spinal dose of 10mg of heavy bupivicaine and 25mcg of fentanyl. 50mg of hydrocortisone was given intravenously. A phenylephrine infusion was started and continued until the blood pressure stabilised. The rate of the phenylephrine infusion was commenced at 2mg per hour, standard practice in our department. After five minutes it was necessary to increase the infusion rate to 3mg per hour, then 4mg per hour in order to maintain her blood pressure at 110/70. An arterial line was not inserted due to the risk of compromising arterial blood supply to the upper limb further. Non-invasive measurement of blood pressures was adequate throughout the Caesarean section. The epidural was used to provide analgesia for six hours postoperatively. There were no complications from the regional anaesthesia. Discussion Combined spinal-epidural is a safe technique for regional anaesthesia in women with TA undergoing Caesarean section. Maintenance of normotension is crucial to avoid complications from the vascular abnormalities, in our patient more phenylephrine than normal was needed. Acknowledgment The patient is aware of this case report and has signed a consent form. References 1. Kathirvel, S., Chavan, S., Arya, V. K. et al. Anesthetic management of patients with Takayasu’s arteritis: a case series and review. Anesthesia & Analgesia, (2001) 93(1), 60-65. 2.Beilin, Y, and Berstein H. "Successful epidural anaesthesia for a patient with Takayasu’s arteritis presenting for caesarean section." Canadian journal of anaesthesia 40, no. 1 (1993): 64-66. Patient monitoring during epidural labour analgesia by midwives: are we doing it right? Salota, Vishal; Costantini, Diletta; Sharafudeen, Saju; Dasan, Jay; Skelton, Va nessa King's College Hospital, London While epidural is considered to be the most effective method of labour analgesia, it is also the most invasive. Therefore, careful monitoring of vital signs and block level during siting and administration of epidural analgesia is essential to minimise the potential risks. We use a PCEA bolus only regime with plain bupivacaine (0.1%) and fentanyl (2 mcg/mL). Current recommendation by NICE during epidural labour analgesia is to measure blood pressure every 5 minutes for 15 minutes during establishment of regional analgesia or further boluses and assess the level of sensory block hourly1. RCoA recommends monitoring heart rate and blood pressure; respiratory rate; temperature; sedation & pain score; degree of motor & sensory block throughout the period of epidural analgesia2. Methods King’s College Hospital is a large London teaching hospital with 7000 deliveries annually with a significant proportion being high risk. After internal governance approval, medical records of 30 patients receiving epidural for labour analgesia were retrospectively reviewed over a period of 2 weeks. Patients who used epidurals for less than 2 hours were excluded. We checked the documented frequency of monitoring of maternal vital parameters including heart rate, blood pressure, respiratory rate, temperature; sedation & pain score; degree of motor & sensory block and fetal heart rate throughout the period of PCEA. We also surveyed 20 midwives to assess their level of awareness of local epidural guideline. Results Compliance to heart rate and blood pressure monitoring after loading dose was 100%. However, further hourly heart rate monitoring was documented in only 33.3%, hourly blood pressure was monitored in 16.6% patients. Only 6.6% patients had documented respiratory rate, with no regular time interval. Regular temperature monitoring was done in 86.6% patients. Sensory block was documented in 20% patients after loading dose. Subsequently, during the progress of labour it was documented only in 6.6% patients, with no regular time interval. None of the patients had documented sedation score, pain score and degree of motor block. The fetal heart rate was assessed regularly through CTG and documented every 15 minutes in all the patients. Figure1 Midwives survey on awareness of epidural guideline (N=20) Disussion Above monitoring results show poor awareness of local trust epidural guidelines among the midwives. This was further confirmed by the survey. Poor adherence to epidural guidelines could prevent early detection of potentially serious complications. We aim to re-educate the midwives through monthly teaching sessions and re-audit the progress in two months time. References 1. Intrapartum care: care of healthy women and their babies during childbirth. NICE guideline (CG 190), December 2014 2. Best practice in the management of epidural analgesia in the hospital setting. RCoA, London, 2010