Serotonin syndrome Author Edward W Boyer, MD, PhD Section

http://www.muyinteresante.es/tag/serotonina
Serotonin syndrome
Author
Edward W Boyer, MD, PhD
Section Editor
Stephen J Traub, MD
Deputy Editor
Jonathan Grayzel, MD, FAAEM
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: May 2012. | This topic last updated: abr 12, 2012.
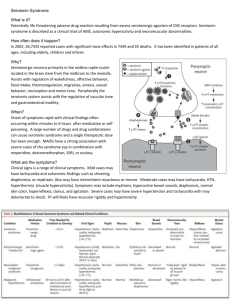
INTRODUCTION — Serotonin syndrome is a potentially life-threatening condition associated with increased serotonergic activity in the central nervous system (CNS). It is seen with therapeutic medication use, inadvertent interactions between drugs, and intentional self-poisoning [ 1 ]. Although classically described as the triad of mental status changes, autonomic hyperactivity, and neuromuscular abnormalities, serotonin syndrome is actually a spectrum of clinical findings ranging from benign to lethal [ 1-4 ]. A summary table to facilitate the emergent management of serotonin syndrome is provided (table 1).
This review will discuss serotonin syndrome. A discussion of selective serotonin reuptake inhibitor (SSRI) intoxication and a general approach to management of the poisoned patient are found elsewhere. (See "Selective serotonin reuptake inhibitor poisoning" and "General approach to drug poisoning in adults".)
EPIDEMIOLOGY — Serotonin syndrome has been observed in all age groups, including newborns and the elderly. The increasing incidence of this condition is thought to parallel the increasing use of serotonergic agents in medical practice [ 1,3,5 ].
In 2004, the Toxic Exposure Surveillance System identified 48,204 exposures to selective serotonin reuptake inhibitors (SSRIs) that resulted in moderate or major outcomes in 8187 patients and death in 103 patients; the vast majority of these fatalities were associated with
coingestants [ 6 ]. The true incidence of serotonin syndrome, however, may be underrepresented in these figures for a number of reasons. Manifestations may be wrongly attributed to another cause, mild cases may be dismissed, or clinicians may not suspect the condition: one study reported that over 85 percent of physicians are unaware of serotonin syndrome as a clinical diagnosis [ 7 ].
PHARMACOLOGY AND CELLULAR TOXICOLOGY — In the central nervous system
(CNS), serotonin modulates attention, behavior, and thermoregulation. In the peripheral nervous system, serotonin is produced primarily by intestinal enterochromaffin cells and is involved in regulating gastrointestinal motility, vasoconstriction, uterine contraction, and bronchoconstriction [ 3 ]. Serotonin is also found in platelets where it promotes platelet aggregation.
Stimulation of the postsynaptic 5-HT1A and 5-HT2A receptors has been implicated in serotonin syndrome [ 8 ], but no single receptor is solely responsible [ 1 ]. Serotonin syndrome may result from any combination of drugs that has the net effect of increasing serotonergic neurotransmission (table 2). The syndrome is classically associated with the simultaneous administration of two serotonergic agents, but it can occur after initiation of a single serotonergic drug or increasing the dose of a serotonergic drug in individuals who are particularly sensitive to serotonin. The syndrome is also described following intentional overdose [ 9 ].
CLINICAL FEATURES AND DIAGNOSIS — The diagnosis of serotonin syndrome is made solely on clinical grounds. Therefore, a detailed history and thorough physical and neurologic examinations are essential.
Serotonin syndrome encompasses a spectrum of disease where the intensity of clinical findings is thought to reflect the degree of serotonergic activity. Mental status changes can include anxiety, agitated delirium, restlessness, and disorientation [ 10 ]. Patients may startle easily. Autonomic manifestations can include diaphoresis, tachycardia, hyperthermia, hypertension, vomiting, and diarrhea [ 3 ]. Neuromuscular hyperactivity can manifest as tremor, muscle rigidity, myoclonus, hyperreflexia, and bilateral Babinski sign.
Hyperreflexia and clonus are particularly common; these findings, as well as rigidity, are more often pronounced in the lower extremities [ 3 ].
Questions remain regarding the exact point at which serotonergic signs associated with therapeutic drug administration become the toxic reaction known as serotonin syndrome.
The transition point likely depends upon an assessment of the risks and benefits of therapy.
As an example, an individual treated for major depression with a serotonergic agent may develop mild tremor and hyperreflexia. Although technically meeting the diagnostic criteria for serotonin syndrome, the patient may benefit more (ie, be less depressed) with continued administration of the agent, even though it produces obvious but tolerable signs of serotonergic excess. However, clinicians should be extremely careful not to add other serotonergic drugs to the regimen of such a patient, and must remain vigilant for any worsening in condition.
History — The patient's history should include a detailed description of prescription drugs, over-the-counter medications, illicit substances, and dietary supplements used, as well as any change in dosing and schedule (table 2). Clinicians should ask about both the dose, the formulation (eg, sustained release), and any recent changes in all medications.
A description of symptoms, their onset, and their rate of change is also important [ 1 ]. The majority of cases of serotonin syndrome present within 24 hours, and most within six hours, of a change or initiation of a drug [ 3 ].
Patients with intentional ingestions often develop greater toxicity than those with accidental exposures, so it is important to ask the patient directly about his or her intentions.
Information obtained from the overdose patient is often unreliable, and confirmation should be sought. Additional history, including comorbid conditions and signs and symptoms, should be elicited from the patient, family members, friends, emergency medical services
(EMS) personnel, and police. A general approach to management of the poisoned patient is found elsewhere. (See "General approach to drug poisoning in adults".)
Physical exam — Typical vital sign abnormalities include tachycardia and hypertension, but severe cases may develop hyperthermia and dramatic swings in pulse and blood pressure. Pertinent physical examination findings include: hyperthermia; agitation; slow, continuous, horizontal, eye movements (referred to as ocular clonus); tremor; akathisia; deep tendon hyperreflexia; inducible or spontaneous clonus; muscle rigidity; bilateral
Babinski signs; dilated pupils; dry mucus membranes; increased bowel sounds; flushed skin; and diaphoresis [ 1 ]. Neuromuscular findings are typically more pronounced in the lower extremities.
Diagnostic criteria — Several sets of diagnostic criteria have been developed to define serotonin syndrome. The most accurate are the Hunter Toxicity Criteria Decision Rules
[ 11 ]. The Hunter Criteria are 84 percent sensitive and 97 percent specific when compared with the gold standard of diagnosis by a medical toxicologist. In a comparison with the original Sternbach Criteria, the Hunter Criteria performed with greater accuracy and were less likely to miss early, mild, or subacute forms of serotonin syndrome.
To fulfill the Hunter Criteria, a patient must have taken a serotonergic agent and meet
ONE of the following conditions:
Spontaneous clonus
Inducible clonus PLUS agitation or diaphoresis
Ocular clonus PLUS agitation or diaphoresis
Tremor PLUS hyperreflexia
Hypertonia PLUS temperature above 38ºC PLUS ocular clonus or inducible clonus
DIFFERENTIAL DIAGNOSIS — The differential diagnosis of serotonin syndrome includes neuroleptic malignant syndrome (NMS), anticholinergic toxicity, malignant hyperthermia, intoxication from sympathomimetic agents, meningitis, and encephalitis.
Serotonin syndrome is often misdiagnosed as NMS, but the two can easily be distinguished on the basis of history, examination findings, and clinical course (table 3) [ 8 ]. NMS develops over days to weeks [ 8 ], whereas serotonin syndrome develops over 24 hours [ 3 ].
Serotonin syndrome is characterized by neuromuscular hyperreactivity (tremor, hyperreflexia, myoclonus), while NMS involves sluggish neuromuscular responses
(rigidity, bradyreflexia). Hyperreflexia and myoclonus are rare in NMS [ 8 ]. Also, resolution of NMS typically requires an average of nine days, compared with less than 24 hours (usually) for resolution of serotonin syndrome [ 8 ]. (See "Neuroleptic malignant syndrome".)
Hyperthermia, altered mental status, muscle rigidity, leukocytosis, elevated creatine phosphokinase, elevated hepatic transaminases, and metabolic acidosis are seen in severe cases of both conditions, which highlights the necessity of a thorough history and physical examination.
Anticholinergic toxicity classically presents with hyperthermia, agitation, altered mental status, mydriasis, dry mucous membranes, urinary retention, and decreased bowel sounds after the use of an anticholinergic agent. Muscular tone and reflexes are normal in anticholinergic poisoning (table 4).
Malignant hyperthermia occurs in susceptible individuals exposed to halogenated volatile anesthetics and depolarizing muscle relaxants (eg, succinylcholine). It classically presents with increased concentrations of end-tidal carbon dioxide, rigor mortis-like muscle rigidity, tachycardia, hyperthermia, and acidosis [ 12 ]. (See "Severe hyperthermia (heat stroke) in adults".)
LABORATORY EVALUATION — Serotonin syndrome is a clinical diagnosis; serum serotonin concentrations do not correlate with clinical findings, and no laboratory test confirms the diagnosis [ 3 ].
Nevertheless, some nonspecific laboratory findings may develop, including an elevated white blood cell count, elevated creatine phosphokinase, and decreased serum bicarbonate concentration. Severe cases may develop disseminated intravascular coagulation, rhabdomyolysis, metabolic acidosis, renal failure, myoglobinuria, and acute respiratory distress syndrome [ 3 ]. (See "Clinical features, diagnosis, and treatment of disseminated intravascular coagulation in adults" and "Clinical manifestations and diagnosis of rhabdomyolysis" and "Acute respiratory distress syndrome: Epidemiology; pathophysiology; pathology; and etiology".)
In order to narrow the differential diagnosis and to monitor for potential complications, particularly in severely ill patients, the following studies may be necessary: complete blood count, basic metabolic panel, creatine phosphokinase, hepatic transaminases, coagulation studies, blood culture, urinalysis, urine culture, chest radiograph, lumbar puncture, and head computed tomography (CT).
MANAGEMENT — A summary table to facilitate the emergent management of serotonin syndrome is provided (table 1). Five principles are central to the management of serotonin syndrome:
Discontinuation of all serotonergic agents (table 2)
Supportive care aimed at normalization of vital signs
Sedation with benzodiazepines
Administration of serotonin antagonists
Assessment of the need to resume use of causative serotonergic agents after resolution of symptoms
Application of these principles varies with the severity of illness. In mild cases, discontinuation of inciting medications, supportive care, and sedation with benzodiazepines is generally sufficient. Moderately ill patients require more aggressive treatment of autonomic instability and possibly treatment with a serotonin antagonist. (See
'Cyproheptadine' below.) Hyperthermic patients are critically ill and often require paralysis and endotracheal intubation.
Common management pitfalls include failure to recognize serotonin syndrome, misdiagnosis, and failure to understand serotonin syndrome's potentially rapid rate of progression. (See 'Clinical features and diagnosis' above.) Even if the diagnosis remains unclear, the clinician should withhold serotonergic agents and provide aggressive supportive care, anticipating the need for interventions before the patient's condition deteriorates.
Serotonin syndrome often resolves within 24 hours of discontinuing the serotonergic agent and initiating care, but drugs with long half-lives or active metabolites may cause symptoms to persist [ 1 ]. Irreversible monoamine oxidase inhibitors (MAOIs) carry the greatest risk, and symptoms can persist for several days. Selective serotonin reuptake inhibitors (SSRIs), may contribute to the development of serotonin syndrome up to several weeks after the drug has been discontinued. The half-life of fluoxetine is one week and that of its metabolite norfluoxetine is up to 2.5 weeks [ 13 ]. Although the patient may not exhibit symptoms of serotonin syndrome while taking fluoxetine, care should be taken when administering another serotonergic agent after discontinuing this or any other SSRI.
As with any toxic exposure, consultation with a medical toxicologist, clinical pharmacologist, or poison control center can provide valuable assistance with clinical decision-making.
Supportive care — Supportive care is the mainstay of therapy and includes the administration of oxygen and intravenous fluids, continuous cardiac monitoring, and correction of vital signs. Clinicians should provide sufficient oxygen to maintain an oxygen saturation greater than 93 percent, and give IV crystalloid to treat volume depletion and hyperthermia.
Chemical restraint is greatly preferred to physical restraint for agitated patients; physical restraints may cause isometric muscle contractions leading to profound lactic acidosis and
hyperthermia [ 1 ]. Sedation with benzodiazepines is important for controlling agitation as well as correcting mild increases in blood pressure and heart rate. Diazepam has prolonged survival in a rat model of serotonin syndrome, but no specific agent has been studied in humans [ 14 ]. Regardless of the benzodiazepine selected, the clinician should give standard doses to begin therapy and titrate further treatment to effect, the goals being adequate patient sedation and normal vital signs.
Autonomic instability — Management of autonomic instability may be difficult since severely intoxicated patients often exhibit large and rapid changes in blood pressure and heart rate. Consequently, patients with severe hypertension and tachycardia should be treated with short-acting agents, such as esmolol or nitroprusside [ 1 ]. Dosing of these shortacting cardiovascular agents should be titrated to maintain autonomic stability; longeracting agents, such as propranolol, should be avoided.
Hypotension from MAOIs should be treated with low doses of direct-acting sympathomimetic amines such as phenylephrine, epinephrine, or norepinephrine [ 1 ].
Indirect agents (eg, dopamine) should be avoided because they are metabolized to epinephrine and norepinephrine; when monoamine oxidase is inhibited, epinephrine and norepinephrine production at the cellular level is not controlled, possibly leading to an exaggerated hemodynamic response [ 1 ].
Hyperthermia — Control of hyperthermia is critical and involves eliminating excessive muscle activity. Aggressive and effective control of hyperthermia can potentially minimize several severe complications of serotonin syndrome (eg, seizures, coma, disseminated intravascular coagulation, hypotension, ventricular tachycardia, and metabolic acidosis) [ 8 ].
Standard treatments for hyperthermia are discussed elsewhere. (See "Severe hyperthermia
(heat stroke) in adults", section on 'Cooling measures'.)
Patients whose temperature is above 41.1ºC require immediate sedation, paralysis, and endotracheal intubation [ 1 ]. Standard rapid sequence intubation (RSI) using an induction and paralytic agent should be performed. Etomidate (0.3 mg/kg IV) and succinylcholine (1.5 to 2 mg/kg IV) can generally be used; succinylcholine should be avoided in patients with possible hyperkalemia (eg, acute renal failure, rhabdomyolysis).
After intubation, paralysis can be maintained with a longer-acting nondepolarizing agent, such as vecuronium. Clinicians must provide adequate sedation, typically with a benzodiazepine, while the patient is paralyzed.
In hyperthermia associated with serotonin syndrome, there is no role for antipyretic agents, such as acetaminophen; the increase in body temperature is not due to an alteration in the hypothalamic temperature set point, but rather an increase in muscular activity [ 1 ].
Cyproheptadine — If benzodiazepines and supportive care fail to improve agitation and correct vital signs, we suggest antidotal therapy be given. Cyproheptadine is the recommended antidote [ 15 ]. Cyproheptadine is a histamine-1 receptor antagonist with nonspecific 5-HT1A and 5-HT2A antagonistic properties [ 15 ]. It also has weak anticholinergic activity.
Cyproheptadine is available in 4 mg tablets or 2 mg/5 mL syrup [ 8 ]. When administered as an antidote for serotonin syndrome, an initial dose of 12 mg is recommended, followed by
2 mg every two hours until clinical response is seen. Cyproheptadine is only available in an oral form, but it may be crushed and given through a nasogastric tube.
Cyproheptadine may lead to sedation, but this effect is consistent with the goals of management [ 1 ]. Furthermore, as a nonspecific serotonin antagonist, cyproheptadine may produce transient hypotension due to the reversal of serotonin-mediated increases in vascular tone. Such hypotension usually responds to intravenous fluids. Cyproheptadine is rated category B for safety in pregnancy by the US Food and Drug administration (FDA)
(table 5) [ 8 ].
Definitive evidence of cyproheptadine's effectiveness is lacking. A small study used PET scan to assess 5-HT2 blockade in two volunteers after taking cyproheptadine (12 mg and 18 mg per day for six days). At 12 mg/day, there was 85 percent blockade and at 18 mg/day there was over 95 percent blockade of 5-HT2 receptors in the prefrontal cortex [ 16 ]. In addition, many reports describe the successful use of cyproheptadine to treat serotonin syndrome [ 15,17-22 ]. The majority of these patients received cyproheptadine at an initial dose of 8 mg, while fewer patients responded to as little as 4 mg and some had no response to as much as 16 mg.
Other antidotes — Antipsychotic agents with 5-HT2A antagonist activity, such as olanzapine and chlorpromazine, have been considered for antidotal treatment, but their efficacy is unproven and we do NOT recommend their use [ 1 ]. Chlorpromazine can cause orthostatic hypotension, although this is generally not an issue with serotonin syndrome, in which hypertension is common. Chlorpromazine can also increase hyperthermia.
Treatment with propranolol, bromocriptine, or dantrolene is NOT recommended.
Propranolol has a long duration of action, may cause prolonged hypotension, and can mask tachycardia that can be used to monitor the effectiveness of treatment. Bromocriptine, a serotonin agonist, may exacerbate serotonin syndrome [ 1 ]. Dantrolene has no effect on survival in animal models.
Disposition and prognosis — Patients with severe serotonin syndrome (eg, hyperthermia, autonomic instability, agitated delirium) require care in an intensive care unit. Those with moderate symptoms should be admitted for observation and placed on a cardiac monitor until symptoms resolve. Symptoms usually resolve within 24 hours of discontinuing the serotonergic agent and initiating care, but drugs with long durations of action or active metabolites may cause prolonged symptoms [ 1 ]. Mild cases may be observed for four to six hours. If during that period the patient's mental status and vital signs remain normal, there is no increase in clonus or deep tendon reflexes, and close follow-up is assured, the patient may be discharged home.
It merits reiteration that serotonin syndrome manifests a broad spectrum of clinical severity.
Particularly in mild cases, clinicians must weigh benefits and risks when determining treatment and whether to continue the causative agent. (See 'Clinical features and diagnosis' above.)
Prognosis is generally favorable, as long as the entity is recognized and complications are treated appropriately.
ADDITIONAL RESOURCES — To obtain emergent consultation with a medical toxicologist, call the United States Poison Control Network at 1-800-222-1222, or access the World Health Organization's list of international poison centers
( www.who.int/gho/phe/chemical_safety/poisons_centres/en/index.html
).
PEDIATRIC CONSIDERATIONS — Serotonin syndrome in the pediatric population parallels that in the adult population, with similar pathophysiology and manifestations. Any drug or drug combination that increases serotonergic neurotransmission can produce the syndrome (table 2). The same diagnostic criteria, characterized by increased neuromuscular activity, are used in the pediatric population. Hyperreflexia, clonus, and hyperthermia remain important findings. (See 'Diagnostic criteria' above.)
Although multiple case reports have been published, several obstacles make the diagnosis of serotonin syndrome more difficult in pediatric patients [ 23-26 ]. Children may not be able to communicate vague symptoms; clinicians may not consider the syndrome a pediatric problem; and adolescents may be reluctant to disclose recreational drug use, which may include serotonergic agents, such as methylenedioxymethamphetamine (MDMA; "ecstasy") or dextromethorphan [ 10 ].
The fundamental principles of serotonin syndrome management remain unchanged in pediatrics. Any serotonergic agent is discontinued. Supportive care is provided, the goals being adequate patient sedation and normal vital signs. Standard interventions include oxygen, intravenous fluids, and continuous cardiac monitoring. Autonomic instability and hyperthermia require aggressive treatment. Sedation with weight-based doses of benzodiazepines is recommended for the treatment of agitation. (See 'Management' above.)
In patients with severe symptoms, serotonergic antagonists can be given; cyproheptadine may be used in pediatric patients with a dose of 0.25 mg/kg/day divided every six hours. Doses should be titrated to maintain adequate sedation. General dosing is as follows:
Children younger than two years can be given approximately 0.06 mg/kg per dose every
six hours, if needed (not to exceed 0.25 mg/kg/day).
Children two to six years can be given 2 mg every six hours, if needed (not to exceed 12 mg/day).
Children 7 to 14 years can be given 4 mg every six hours, if needed (not to exceed 16 mg/day).
Pediatric patients with severe serotonin syndrome require management in an intensive care unit. Pediatric patients with mild to moderate symptoms should be placed on a cardiac monitor and admitted for observation. If serotonin syndrome is recognized and complications are treated appropriately, the prognosis is generally favorable.
In addition to cases in the general pediatric population, there are rare reports of neonates with symptoms resembling serotonin syndrome. One small study showed that infants exposed to SSRIs late in pregnancy were at increased risk for adverse central nervous system (CNS) effects [ 27 ]. The most prominent findings were restlessness, tremor, and rigidity; myoclonus and hyperreflexia occurred less often. Symptoms appeared to subside quickly without any specific treatment [ 27 ].
PREVENTION — Serotonin syndrome can be avoided by applying pharmacologic principles, educating clinicians, and modifying prescription practices [ 1 ]. Multi-drug regimens should be avoided, if possible. Once serotonin syndrome occurs, a medical toxicologist, clinical pharmacologist, or poison control center should be consulted for assistance.
SUMMARY AND RECOMMENDATIONS
Diagnosis
Serotonin syndrome is a potentially life-threatening condition associated with increased serotonergic activity in the central nervous system (CNS). It is seen with therapeutic medication use, inadvertent interactions between drugs, and intentional self-poisoning. A summary table to facilitate the emergent management of serotonin syndrome is provided
(table 1).
The diagnosis of serotonin syndrome is made solely on clinical grounds; a detailed history and thorough physical and neurologic examination are essential. (See 'Clinical features and diagnosis' above.)
The majority of cases of serotonin syndrome present within 24 hours, and most within six hours, of a change or initiation of a drug (table 2). The patient's history should include a detailed description of prescription drugs, over-the-counter medications, illicit substances, and dietary supplements used, as well as any change in dosing and schedule. Clinicians should ask about both the dose, the formulation (eg, sustained release), and any recent changes in all medications. (See 'History' above.)
Typical vital sign abnormalities include tachycardia and hypertension, but severe cases may develop hyperthermia and rapid, dramatic swings in pulse and blood pressure.
Pertinent physical examination findings include: hyperthermia, agitation, ocular clonus, tremor, akathisia, deep tendon hyperreflexia, inducible or spontaneous clonus, muscle rigidity, dilated pupils, dry mucus membranes, increased bowel sounds, flushed skin, and diaphoresis. Neuromuscular findings are typically more pronounced in the lower extremities. (See 'Physical exam' above.)
The Hunter Toxicity Criteria Decision Rules represent the most accurate diagnostic criteria for serotonin syndrome. To fulfill the Hunter Criteria, a patient must have taken a serotonergic agent and meet ONE of the following conditions (see 'Physical exam' above):
Spontaneous clonus
Inducible clonus PLUS agitation or diaphoresis
Ocular clonus PLUS agitation or diaphoresis
Tremor PLUS hyperreflexia
Hypertonia PLUS temperature above 38ºC PLUS ocular clonus or inducible clonus
Serotonin syndrome is a clinical diagnosis; serotonin concentrations do not correlate with clinical findings, and no laboratory test confirms the diagnosis. To narrow the differential diagnosis and to monitor potential complications, particularly in severely ill patients, additional diagnostic studies may be necessary. (See 'Laboratory evaluation' above.)
Treatment
An overview of the management of serotonin syndrome is provided (table 1). Application of the following principles is central to management of acute serotonin syndrome:
Discontinuation of all serotonergic agents
Supportive care aimed at normalization of vital signs
Sedation with benzodiazepines
Administration of serotonin antagonists
Application of these principles varies with the severity of illness. In mild cases, discontinuation of inciting medications, supportive care, and sedation with benzodiazepines is generally sufficient. Moderately ill patients require more aggressive treatment of autonomic instability and possibly treatment with a serotonin antagonist.
Hyperthermic patients are critically ill and often require paralysis and endotracheal intubation. (See 'Management' above.)
Supportive care is the mainstay of therapy. For all patients who fulfill the Hunter Criteria, we suggest the following standard treatments (Grade 2C):
Oxygen to maintain SpO2 ≥94 percent
Intravenous fluids for volume depletion, and hyperthermia
Continuous cardiac monitoring
Correction of vital signs
We suggest sedation with benzodiazepines for controlling agitation as well as correcting mild increases in blood pressure and heart rate (Grade 2C). (See 'Management' above.)
Management of autonomic instability may be difficult; severely intoxicated patients often exhibit rapid, dramatic changes in vital signs. For patients with severe hypertension and tachycardia, we suggest treatment with short-acting agents, such as esmolol and nitroprusside (Grade 2C). For hypotension from monoamine oxidase inhibitors (MAOIs), we suggest treatment with low doses of direct-acting sympathomimetic amines such as phenylephrine, epinephrine, or norepinephrine (Grade 2C). We recommend that indirect agents (eg, dopamine) NOT be used (Grade 1C). (See 'Management' above.)
Control of hyperthermia is critical and involves eliminating excessive muscle activity. For patients whose temperature is above 41.1ºC, we recommend treatment with immediate sedation, paralysis, and orotracheal intubation (Grade 1C). In hyperthermia associated with serotonin syndrome, antipyretic agents (eg, acetaminophen) are ineffective and should NOT be used. (See 'Management' above.) Standard treatments for hyperthermia should be implemented and are discussed elsewhere. (See "Severe hyperthermia (heat stroke) in adults", section on 'Cooling measures'.)
If benzodiazepines and supportive care fail to improve agitation and correct vital signs, we suggest treatment with cyproheptadine, a histamine-1 receptor antagonist (Grade 2C).
When administered as an antidote for serotonin syndrome, an initial dose of 12 mg is given, followed by 2 mg every two hours until clinical response is seen. Cyproheptadine is only available in an oral form, but it may be crushed and given through a nasogastric tube.
Cyproheptadine may lead to sedation and transient hypotension that is responsive to intravenous fluids. (See 'Cyproheptadine' above.) Detailed pediatric dosing is provided above. (See 'Pediatric considerations' above.)
Use of UpToDate is subject to the Subscription and License Agreement .
REFERENCES
1 Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005; 352:1112.
2
Birmes P, Coppin D, Schmitt L, Lauque D. Serotonin syndrome: a brief review. CMAJ 2003;
168:1439.
3
Mason PJ, Morris VA, Balcezak TJ. Serotonin syndrome. Presentation of 2 cases and review of the literature. Medicine (Baltimore) 2000; 79:201.
4 Bodner RA, Lynch T, Lewis L, Kahn D. Serotonin syndrome. Neurology 1995; 45:219.
5 Sternbach H. The serotonin syndrome. Am J Psychiatry 1991; 148:705.
6
Watson WA, Litovitz TL, Rodgers GC Jr, et al. 2004 Annual report of the American Association of
Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 2005; 23:589.
7
Mackay FJ, Dunn NR, Mann RD. Antidepressants and the serotonin syndrome in general practice. Br J Gen Pract 1999; 49:871.
8 Mills KC. Serotonin syndrome. A clinical update. Crit Care Clin 1997; 13:763.
9
De Roos, FJ. Drug interactions: combinations that can kill your patients. American College of
Emergency Physicians Scientific Assembly lecture, Sep 26, 2005, Washington Convention
Center.
10
Ganetsky, M, Brush, E. Serotonin syndrome—what have we learned? Clin Ped Emerg Med
2005; 6:103.
11
Dunkley EJ, Isbister GK, Sibbritt D, et al. The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM 2003; 96:635.
12
Ali SZ, Taguchi A, Rosenberg H. Malignant hyperthermia. Best Pract Res Clin Anaesthesiol 2003;
17:519.
13 Martin TG. Serotonin syndrome. Ann Emerg Med 1996; 28:520.
Nisijima K, Shioda K, Yoshino T, et al. Diazepam and chlormethiazole attenuate the
14 development of hyperthermia in an animal model of the serotonin syndrome. Neurochem Int
2003; 43:155.
15
Graudins A, Stearman A, Chan B. Treatment of the serotonin syndrome with cyproheptadine. J
Emerg Med 1998; 16:615.
16
Kapur S, Zipursky RB, Jones C, et al. Cyproheptadine: a potent in vivo serotonin antagonist. Am J
Psychiatry 1997; 154:884.
17
Baigel GD. Cyproheptadine and the treatment of an unconscious patient with the serotonin syndrome. Eur J Anaesthesiol 2003; 20:586.
18 Gillman PK. The serotonin syndrome and its treatment. J Psychopharmacol 1999; 13:100.
19
Horowitz BZ, Mullins ME. Cyproheptadine for serotonin syndrome in an accidental pediatric sertraline ingestion. Pediatr Emerg Care 1999; 15:325.
20
Kolecki P. Venlafaxine induced serotonin syndrome occurring after abstinence from phenelzine for more than two weeks. J Toxicol Clin Toxicol 1997; 35:211.
21
Lappin RI, Auchincloss EL. Treatment of the serotonin syndrome with cyproheptadine. N Engl J
Med 1994; 331:1021.
22
McDaniel WW. Serotonin syndrome: early management with cyproheptadine. Ann
Pharmacother 2001; 35:870.
23
Thomas CR, Rosenberg M, Blythe V, Meyer WJ 3rd. Serotonin syndrome and linezolid. J Am
Acad Child Adolesc Psychiatry 2004; 43:790.
24
Pao M, Tipnis T. Serotonin syndrome after sertraline overdose in a 5-year-old girl. Arch Pediatr
Adolesc Med 1997; 151:1064.
25
Godinho EM, Thompson AE, Bramble DJ. Neuroleptic withdrawal versus serotonergic syndrome in an 8-year-old child. J Child Adolesc Psychopharmacol 2002; 12:265.
26
Gill M, LoVecchio F, Selden B. Serotonin syndrome in a child after a single dose of fluvoxamine.
Ann Emerg Med 1999; 33:457.
Laine K, Heikkinen T, Ekblad U, Kero P. Effects of exposure to selective serotonin reuptake
27 inhibitors during pregnancy on serotonergic symptoms in newborns and cord blood monoamine and prolactin concentrations. Arch Gen Psychiatry 2003; 60:720.
Topic 301 Version 7.0 • All rights reserved.
©2012 UpToDate ®
• customerservice@uptodate.com