Serotonin Syndrome
What is it?
Potentially life threatening adverse drug reaction resulting from excess serotonergic agonism of CNS receptors. Serotonin
syndrome is described as a clinical triad of AMS, autonomic hyperactivity and neuromuscular abnormalities.
How often does it happen?
In 2002, 26,7333 reported cases with significant toxic effects in 7349 and 93 deaths. It has been identified in patients of all
ages, including elderly, children and infants.
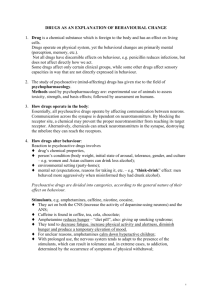
Why?
Serotonergic neurons primarily in the midline raphe nuclei
located in the brain stem from the midbrain to the medulla.
Assists with regulation of wakefulness, affective behavior,
food intake, thermoregulation, migraines, emesis, sexual
behavior, nociception and motor tone. Peripherally the
serotonin system assists with the regulation of vascular tone
and gastrointestinal motility.
When?
Onset of symptoms rapid with clinical findings often
occurring within minutes to 6 hours after medication or self
poisoning. A large number of drugs and drug combinations
can cause serotonin syndrome and a single therapeutic dose
has been enough. MAOIs have a strong association with
severe cases of the syndrome esp in combination with
meperidine, dextromethorphan, SSRI, or ecstasy.
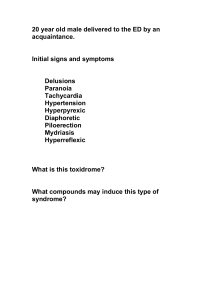
What are the symptoms?
Clinical signs is a range of clinical symptoms. Mild cases may
have tachycardia and autonomic findings such as shivering,
diaphoresis, or mydriasis. Also may have intermittent myoclonus or tremor. Moderate cases may have tachycardia, HTN,
hyperthermia (muscle hyperactivity). Symptoms may include mydriasis, hyperactive bowel sounds, diaphoresis, normal
skin color, hyperreflexia, clonus, and agitation. Severe cases may have severe hypertension and tachycardia with may
deteriorate to shock. Pt will likely have muscular rigidity and hypertonicity.
How to treat?
Removal of precipitating drugs. Many cases serotonin syndrome resolve within 24 hours after the initiation of therapy and
discontinuation of serotonergic drugs.
Mild cases can be managed with supportive care and treatment of benzodiazepines to control agitation.
Moderate cases should have all cardiorespiratory and thermal abnormalities aggressively corrected. Pt may benefit from 5HT2A antagonist, cyproheptadine.
Severe cases should additionally have immediately sedation, neuromuscular paralysis and intubation.
How not to treat?
Propranolol, bromocriptine, and dantrolene not recommended. Propranolol , a 5 HT1A antagonist, has long duration of
action and may cause hypotension. Bromocriptine (dopamine agonist and used in neuroleptic malignant syndrome) has
been implicated in development of serotonin syndrome. Dantrolene has no effect on survival.
 0
0