Supplemental Fig. 1: Health questionnaire
advertisement

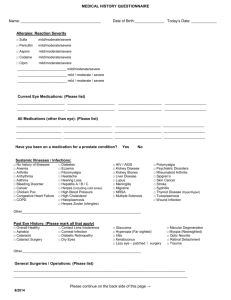
Supplemental Fig. 1: Health questionnaire - completed by patients at study enrollment Health Questionnaire At Start of Administration This questionnaire contains questions on the degree of severity of your chest and stomach conditions and your life-style activities. Your cooperation will be highly appreciated. You will later receive another questionnaire on your conditions after taking the drug. 1. Tick (☑) the most appropriate box for each of Questions #1 to 9 below. (1) Did you experience any sensation of heartburn, chest pain, or chest heaviness in the previous week? (heartburn) □Never □Sometimes/mild □Often/moderate □Frequent/severe (2) Did you feel a regurgitation of stomach contents into the mouth, leaving an acid or bitter taste in the previous week? (regurgitation) □Never □Sometimes/mild □Often/moderate □Frequent/severe (3) Did you feel your stomach was upset, heavy, or containing food for a long time in the previous week? (postprandial fullness) □Never □Sometimes/mild □Often/moderate □Frequent/severe (4) Did you feel too full to eat any more after small amounts of food in the previous week? (early satiation) □Never □Sometimes/mild □Often/moderate □Frequent/severe (5) Did you feel pain in the stomach or epigastrium in the previous week? (epigastric pain) □Never □Sometimes/mild □Often/moderate □Frequent/severe (6) Did you feel burning sensation in the stomach or epigastrium in the previous week? (epigastric burning) □Never □Sometimes/mild □Often/moderate □Frequent/severe (7) Did you feel your stomach was distended in the previous week? (upper abdominal bloating) □Never □Sometimes/mild □Often/moderate □Frequent/severe (8) Did you have nausea or churning feeling in the stomach in the previous week? (nausea/vomiting) □Never □Sometimes/mild □Often/moderate □Frequent/severe (9) Did you belch in the previous week? (belching) □Never □Sometimes/mild □Often/moderate □Frequent/severe 2. Tick (☑) all relevant boxes concerning your daily life style. □ You keep on eating until you feel full. □ You eat greasy food (e.g., fries, high-fat meat, potato chips) at least once in 2 to 3 days. □ You eat sweets (e.g., manju cakes, sweet bean-jam cakes, cream cakes) at least once in 2 to 3 days. □ You eat hot and spicy food (e.g., curry rice, chili pepper food) at least once in 2 to 3 days. □ You drink alcoholic drink almost daily. □ You drink coffee almost daily. □ You smoke 10 or more cigarettes a day. □ You usually wear girdles or corsets. □ You often have a bent-forward posture during work and other activities. □ You frequently lie down after eating. □ You are feeling continued stress. Supplemental Fig. 2: Health questionnaire - completed by patients 2 weeks after the start of lansoprazole administration Health Questionnaire At Week 2 This questionnaire contains questions on the degree of severity of your chest and stomach conditions. Your cooperation will be highly appreciated. Two weeks later, you will receive another questionnaire on your conditions after taking the drug. Tick (☑) the most appropriate box for each of Questions #1 to 10 below. (1) Did you experience any sensation of heartburn, chest pain, or chest heaviness in the previous week? (heartburn) □Never □Sometimes/mild □Often/moderate □Frequent/severe (2) Did you feel a regurgitation of stomach contents into the mouth, leaving an acid or bitter taste in the previous week? (regurgitation) □Never □Sometimes/mild □Often/moderate □Frequent/severe (3) Did you feel your stomach was upset, heavy, or containing food for a long time after meal in the previous week? (postprandial fullness) □Never □Sometimes/mild □Often/moderate □Frequent/severe (4) Did you feel too full to eat any more after taking small amounts of food in the previous week? (early satiation) □Never □Sometimes/mild □Often/moderate □Frequent/severe (5) Did you feel pain in the stomach or epigastrium in the previous week? (epigastric pain) □Never □Sometimes/mild □Often/moderate □Frequent/severe (6) Did you feel burning sensation in the stomach or epigastrium in the previous week? (epigastric burning) □Never □Sometimes/mild □Often/moderate □Frequent/severe (7) Did you feel your stomach was distended in the previous week? (upper abdominal bloating) □Never □Sometimes/mild □Often/moderate □Frequent/severe (8) Did you have nausea or churning feeling in the stomach in the previous week? (nausea/vomiting) □Never □Sometimes/mild □Often/moderate □Frequent/severe (9) Did you belch in the previous week? (belching) □Never □Sometimes/mild □Often/moderate □Frequent/severe (10) How often did you take the medicine to relieve your chest and stomach symptoms? (compliance) □Took every day □Missed 1-2 days/week □Missed 3-4 days/week □Missed almost every day Supplemental Fig. 3: Health questionnaire - completed by patients 4 weeks after the start of lansoprazole administration Health Questionnaire At Week 4 This questionnaire contains questions on the degree of severity of your chest and stomach conditions. Your cooperation will be highly appreciated. Tick (☑) the most appropriate box for each of Questions #1 to 12 below. (1) Did you experience any sensation of heartburn, chest pain, or chest heaviness in the previous week? (heartburn) □Never □Sometimes/mild □Often/moderate □Frequent/severe (2) Did you feel a regurgitation of stomach contents into the mouth, leaving an acid or bitter taste in the previous week? (regurgitation) □Never □Sometimes/mild □Often/moderate □Frequent/severe (3) Did you feel your stomach was upset, heavy, or containing food for a long time after meal in the previous week? (postprandial fullness) □Never □Sometimes/mild □Often/moderate □Frequent/severe (4) Did you feel too full to eat any more after taking small amounts of food in the previous week? (early satiation) □Never □Sometimes/mild □Often/moderate □Frequent/severe (5) Did you feel pain in the stomach or epigastrium in the previous week? (epigastric pain) □Never □Sometimes/mild □Often/moderate □Frequent/severe (6) Did you feel burning sensation in the stomach or epigastrium in the previous week? (epigastric burning) □Never □Sometimes/mild □Often/moderate □Frequent/severe (7) Did you feel your stomach was distended in the previous week? (upper abdominal bloating) □Never □Sometimes/mild □Often/moderate □Frequent/severe (8) Did you have nausea or churning feeling in the stomach in the previous week? (nausea/vomiting) □Never □Sometimes/mild □Often/moderate □Frequent/severe (9) Did you belch in the previous week? (belching) □Never □Sometimes/mild □Often/moderate □Frequent/severe (10) How often did you take the medicine to relieve your chest and stomach symptoms? (compliance) □Took every day □Missed 1-2 days/week □Missed 3-4 days/week □Missed almost every day (11) Are you satisfied with the medicine to relieve your chest and stomach symptoms? (Treatment satisfaction) □Very satisfied □Satisfied □Neutral □Dissatisfied □Very dissatisfied (12) Are you willing to continue use of the medicine to relieve your chest and stomach symptoms? (Willingness to continue) □Willing to continue to use □Willing to use if symptoms relapse □Unwilling to use Supplemental Table 1. Classification of treatment response After two and four weeks of LPZ treatment At the start of LPZ treatment Never Sometimes/Mild Often/Moderate Frequent/Severe Never None before or become worse become worse become worse after treatment Sometimes/Mild Disappearance no change become worse become worse of symptoms Often/Moderate Disappearance Improvement no change become worse of symptoms Frequent/Severe Disappearance Improvement no change no change of symptoms Unclear Unclear Unclear Unclear Unclear LPZ: Lansoprazole Unclear Unclear Unclear Unclear Unclear Unclear