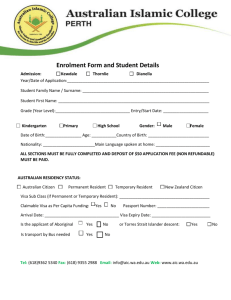
enrolment form - Sunset Road Family Doctors
advertisement

Dr Patti Piper 13207 Dr Sarah English 40659 Dr Meg Thomson 44022 EDI - sunsetfd Unit 3/317 Sunset Road, Sunnynook 0632 Phone: 09 478 2878 Fax: 09 478 3007 PATIENT ENROLMENT FORM 1. Each person aged 16 years and over needs to sign their own form Family Name Given Name Preferred Name Date of Birth Sex Ethnicity NHI (reception to (see to Q4) complete) 1. 2. 3. 4. My preferred practitioner ……………………………………………………….. (Optional) By signing this enrolment you are enrolling at Sunset Road Family Doctors not a specific Doctor, though you can let us know you’re preferred Provider 2. Contact Details Street Address …………………………………………………………………….…. Suburb/Town …………….………………………… City ……………………………………………………. Post code …………………………… Phone (home) …………………………………… Email ………………………………………………………………… Phone (mobile) ………………………………. Phone (work) …………………………… (are you happy to receive texts on this number? please circle one) yes no Is this your main contact number? please circle one yes no Place of Birth ……………………………………… Occupation ……………………………………………………… Employer details ………………………………………………………………………………….. …………………………………………………………………………………………………………. 3. 4. Next of Kin/Emergency contact details Name ………………………………………………………. Street Address………………………………………………………………………………………………… Phone (home) ………………………………. Phone (mobile) ………………………………. Relationship ………………………..……………… Ethnicity Which Ethnic group do you identify with? Please write code number in the ethnicity column above for each person being enrolled. 21 36 41 40 5. Maori Hapu/iwi………………. Fijian 34 Niuean South East Asian Asian not defined 11 33 43 12 Community Services Card Yes Card Number ………………………………………………. NZ European Tongan Indian Other European Yes Card Number ……………………………………………… 7. Are you a New Zealand Citizen? 35 37 44 54 Tokelauan Other Pacific Islands Other Asian Not stated No Start Date ……………………….… Expiry Date ………………………………… If No: Are you a permanent resident of NZ? Work permit Status of at least 2 years Yes Yes Yes Smoking Status. Past Smoker Smoker Cook Island Maori Samoan Chinese Middle Eastern No Start Date …………………………. Expiry Date ………………………………. High User Card 6. 32 31 42 51 No No No If No: Passport and visa to be sighted Never Smoked ENROLMENT IN THE PRACTICE/PRIMARY HEALTH ORGANISATION (PHO) I intend to use Sunset Road Family Doctors as my regular and ongoing provider of general practise / GP / First Level primary health care services. a. b. c. d. e. f. g. h. i. j. k. I am a New Zealand citizen I hold a resident visa or a permanent resident visa (or a residence permit issued before December2010) I am an Australian or Australian permanent resident AND able to show I have been in New Zealand or intend to stay in New Zealand for a t least 2 consecutive years I have a work visa/permit and can show that I am able to be in new Zealand for at least 2 years (previous permits included) I am an interim visa holder who was eligible immediately before my interim visa started I am a refugee or protected person OR in the process of applying for, or appealing refugee or protection status, OR a victim or suspected victim of people trafficking I am under 18 years and in the care and control of a parent/legal guardian/adopting parent who meets one criterion on clauses a-f above I am 18 or 19 years old and can demonstrate that, on the 15 April 2011, I was the dependant of an eligible work permit holder I am a NZ Aid Programme student studying in NZ and receiving Official Development Assistance funding (or their partner or child under 18 years old) I am participating in the Ministry of Education Foreign Language Teaching Assistantship scheme I am a Commonwealth Scholarship holder studying in NZ and receiving funding from a New Zealand University under the Commonwealth Scholarship and Fellowship Fund I confirm that, if requested, I can provide proof of my eligibility Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes MY AGREEMENT TO THE ENROLMENT PROCESS I choose to enrol with this practice as my regular and ongoing provider of general practise / GP / First Level primary health care services. I understand that by enrolling with this practise I will be enrolled with the Primary Health Organisation (PHO) this practise belongs to, and my name, address and other identification details will be included on both the Practise and the PHO enrolment Register. I understand that if I visit another provider where I am not enrolled I may be charged a higher fee. I have been given information about the benefits and implications of enrolment with the PHO, and their contact details. I have read and I agree with the Health information Privacy Statement. I agree to inform the practice of any changes in my eligibility. Name ……………………………………………….. Signature ………………………………………… Date……………………………………… INFORMATION FOR GP 2 GP FILE TRANSFERS Dr Patti Piper 13207 Dr Sarah English Dr Meg Thomson 44022 40659 EDI - sunsetfd REQUEST THE TRANSFER OF MY/OUR MEDICAL RECORDS I understand that I will be removed from the register of my previous General Practice and I authorise the transfer of my records (and/or my child/children under 16 years) Yes No Family Name 1. 2. 3. 4. Given Name Date of Birth NHI Previous Surgery/GP Name ………………………………………………………………………………. Address …………………………………………………………….. Contact Details …………………………………………………… Name ………………………………………………… Signature …………………………………………… Date …………………………………. Unit 3/317 Sunset Road, Sunnynook 0632 P: 09 478 2878 F: 09 478 3007 E: reception@sunsetrfd.co.nz