Abeer Ahmed Mohamed Shoman_paper(TB)
advertisement
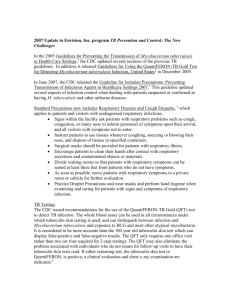
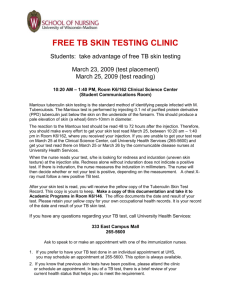
")
COMPARATIVE STUDY BETWEEN TUBERCULIN SKIN TEST AND SERUM ALBUMIN LEVEL IN PATIENTS WITH ACTIVE PULMONARY TUBERCULOSIS Ahmad Abdelsadek Mohammad MD*.Osama E.Mohammad MD*Abeer A. ShomanMD** Chest Department - Faculty of medicine Benha University*.Physiology department Faculty of Medicine Benha University**. Abstract Aim of the Work: To study the possible relationship between severity of tuberculin skin test reaction and serum albumin level in patients with active pulmonary tuberculosis. Subjects and Methods: 40 patients with active pulmonary tuberculosis just before initiation of treatment, that were selected from chest outpatient clinic, Benha university hospital, they were classified into:Group A included twenty patients with serum albumin level below 3.5g/dl. This group included 17 males (85%) and 3 females (15%) with their ages ranging from 23 to 70 years. And Group B included twenty patients with serum albumin level ≥ 3.5g/dl. this group included 16 males (80%) and 4 females (20%) with their ages ranging from 15 to 68 years. . The patients were subjected for full clinical evaluation, History of any other co-morbidity that may affect tuberculin skin test reactions were excluded like previous anti tuberculosis treatment.HIV infection, alcoholism and drug abuse, chronic renal failure, neoplasmic diseases and chronic use of corticosteroids. General &local examination, laboratory tests including complete blood count (CBC),erythrocyte sedimentation rate (ESR).liver and kidney function tests, plain chest x-ray (P.A. and lateral views), Tuberculin skin test using Mantoux technique, Sputum for acid fast bacilli by Z. N. stain for three consecutive days and Serum albumin level at the same time of Tuberculin test. Results: According to this study serum albumin level in group A was ranging from 1.5-3.4 gm/dl with mean 2.6±0.48 and in group B was ranging from 3.5-4.5 with mean 3.85±0.33. These results showed statistical significant difference between the two groups, In the present study, tuberculin skin test diameter in (group A) was ranging from 5-15mm with mean 7.5±3.94 and in (group B) was ranging from 12-30mm with mean 20.9±5.51. Which showed statistically significant difference between the two groups, in our study there was a statically significant positive -1- correlation between intensity of tuberculin skin reaction at 72 hours and serum albumin levels in both group. Conclusion: Patients with active pulmonary tuberculosis and lower serum albumin levels react with weaker skin responses to tuberculin test. Key words: active pulmonary tuberculosis, tuberculin skin test, serum albumin levels. INTRODUCTION Tuberculosis or TB (short for tubercle bacilli) is a common and often deadly infectious disease caused by various strains of mycobacteria, usually Mycobacterium tuberculosis in humans. Tuberculosis usually attacks the lungs but can also affect other parts of the body [ 1]. Tuberculin skin test (TST) is a useful diagnostic test for evaluating persons who have symptoms of tuberculosis or who are suspected of being infected with M. tuberculosis [ 2] . Tuberculin skin test (TST) is the standard test for the diagnosis of asymptomatic tuberculous infection.Tuberculin a broth culture filtrate of tubercle bacilli was first prepared by (Robert Koch) in 1891. Subsequently a standardized version of Tuberculin, the purified protein derivative (PPD) was introduced in 1934 [ 3]. Serum albumin is the most abundant protein in human plasma. Albumin is synthesized in the liver as preproalbumin. The rate of synthesis is dependent on protein intake, subjected to feed back regulation by plasma level, oncotic pressure, inflammation and hormones. During times of increased albumin loss, the liver can increase the rate of synthesis [ 4]. Hypoalbuminemia is a common problem among persons with acute and chronic medical conditions, malnutrition is observed frequently in patients with pulmonary tuberculosis due to anorexia [ 5]. -2- AIM OF THE WORK To study the possible relationship between severity of tuberculin skin test reaction and serum albumin level in patients with active pulmonary tuberculosis. PATIENTS AND METHODS The study included 40 patients with active pulmonary tuberculosis just before initiation of treatment, that were selected from chest outpatient clinic , Benha university hospital, in the period from march 2010 to December 2011, they were classified into: Group A: included twenty patients with serum albumin level below 3.5g/dl. This group included 17 males (85%) and 3 females (15%) their ages ranging from 23 to 70 years. Group B: included twenty patients with serum albumin level ≥ 3.5g/dl. This group included 16 males (80%) and 4 females (20%) with their ages ranging from 15 to 68 years. Inclusion criteria Patients suffering from active pulmonary tuberculosis (smear positive) defined as one or more initial sputum smear examinations positive for Acid Fast Bacilli by microscopy [ 6]. Exclusion criteria ● Previous anti tuberculosis treatment. ● HIV infection. ● Alcoholism and drug abuse. ● Chronic renal failure. ● Neoplasmic diseases ●Chronic use of corticosteroids All patients were subjected to: (1) Full History tacking and physical examination. With special attention to fever, cough, loss of weight and appetite, night sweats, weakness -3- and malaise.Physical signs, such as pallor and weight loss, rales, bronchial breathing. (2) Laboratory tests. Complete blood count (CBC). Erythrocyte sedimentation rate (ESR). Liver and Kidney function tests. (3) Plain Chest X-ray P-A view Chest x ray was done to detect radiological classification according to the extent and exclude an associated lung disease. (4) Tuberculin skin testing by (Mantoux technique). By using 0.1ml (5 tuberculin units) of PPD RT tween 80 administrated intradermally in the volar surface of the forearm. then reading after 48-72 hours, a positive reaction is indicated by induration of > 10 mm in size. (5) Sputum for acid fast bacilli by Z. N. stain. Collection of sputum: Three first morning sputum specimens obtained after a deep productive cough for three consecutive days, ask the patients to cough into a sterile screw cap cups, 5-10 ml of sample of each time is appropriate [ 7].The specimens were kept at 4cº prior to processing with N-Acetyl-L-Cysteine- NaOH (NALC-NaOH), for liquefaction, decontamination and concentration [ 8]. (6) Serum albumin level at the same time of Tuberculin test. Statistical analysis The program used was SPSS version 16. Quantitative data were analyzed using mean and standard deviation, while frequency and percentage were used with qualitative data. Student t test was used to compare means of different groups, while chi square and z test to compare frequencies. Pearson correlation was used to find relationships. Statistical significance was set at p < 0.05 [ 9]. -4- RESULTS Table (1): Age distribution among the studied groups. Variable Groups Range Mean ±SD Group A 23-70 44.25 15.55 Group B 15-68 35.3 14.77 Student t test P value 1.87 0.07 NS Age Table (2): Sex distribution among the studied groups. Group A Group B Total Sex No % No % No % Male 17 85.0 16 80.0 33 82.5 Female 3 15.0 4 20.0 7 17.5 Total 20 100.0 2 100.0 40 100.0 S = significant FET P value 0.173 1.0 ( N.S.) N.S = non significant Table (3): Radiological classification according to the extent among groups. Group A Group B Total X ray finding Minimal Moderate advanced Far advanced No % No % No % 10 45.0 8 40.0 17 42.5 7 35.0 8 40.0 15 37.5 3 15.0 4 20.0 7 17.5 -5- FET P value 0.243 0.89 )N.S) Total 20 100.0 20 100.0 40 100.0 Table (4):Serum albumin levels among studied groups. Variable Groups Range Mean± SD Group A 1.5-3.4 2.6± 0.48 Group B 3.5- 4.5 3.85± 0.33 Albumin Student t test P value 9.51 0.001 (S) This table shows that there is statistically significant difference between group A and group B as regarding serum albumin (p=0.001). Table (5): The diameter of induration in the tuberculin skin test of the studied groups after 72 hours. Variable Groups Range Mean± SD Tuberculin test Group A 5-15 7.5± 3.94 Group B 12-30 20.9± Student t test P value 8.84 0.001 (S) 5.51 This table shows that there is a significant tendency for the 72 hours reaction to be larger among group B (p=0.001). Figure (1): Correlation between intensity of tuberculin skin reaction after72 hours and serum albumin levels in group A. -6- 16 y = 7.8924x - 13.02 R² = 0.9417 Tuberculin test diameter 14 12 10 8 6 4 2 0 -2 0 0.5 1 1.5 2 Albumin 2.5 3 3.5 4 This figure shows positive statistical significant correlation between intensity of tuberculin skin reaction after 72 hours and serum albumin levels in group A Figure (2): Correlation between intensity of tuberculin skin reaction after 72 hours and serum albumin levels in group B. -7- 35 y = 15.804x - 39.866 R² = 0.8859 Tuberculin test diameter 30 25 20 15 10 5 0 0 1 2 3 4 5 Albumin level This figure shows positive statistical significant correlation between intensity of tuberculin skin reaction after 72 hours and serum albumin levels in group B. DISCUSSION Tuberculin skin test is a useful diagnostic test for evaluating persons who have symptoms of tuberculosis or who are suspected of being infected. Positive tuberculin skin test only indicates infection and by itself is not diagnostic of TB disease as it fails to distinguish between active disease and prior sensitization by contact with M.tuberculosis [10].Malnutrition and tuberculosis are both problems of considerable magnitude, these two problems tend to interact with each other and link between them has long been recognized. Malnutrition can lead to secondary immunodeficiency that increase the host’s susceptibility to the development of clinical disease. In patients with tuberculosis, it leads to reduction in appetite, nutrition malabsorption and altered metabolism [11]. In the present study 40 patients with active pulmonary tuberculosis was divided into group A with serum albumin level below 3.5g/dl and their ages ranging from 23 to 70 years and mean was 44.25±15.55 and group B with serum albumin level ≥ 3.5g/dl and their ages ranging from 15 to 68 years and mean was 35.3±14.77, these results showed no statistical significant difference between the two groups as regarding age distribution (Table 1). -8- The current study group A included 17 males (85%) and 3 females (15%) and group B included 16 males (80%) and 4 females (20%) which revealed no statistical significant difference (Table 2).The radiological classification of the extent of the disease in current study was; (group A) minimal disease: 10 patients (45%), moderate advanced disease: 7 patients (35%) and far advanced disease: 3 patients (15%) and in patients (group B), minimal:8 patients(40%),moderate advanced:8 patients(40%), far advanced: 4 patients(20%) The results revealed no statistical significant difference between two groups (Table 3). According to this study serum albumin level in group A was ranging from 1.5-3.4 gm/dl with mean 2.6±0.48 and in group B was ranging from 3.5-4.5 with mean 3.85±0.33. These results showed statistical significant difference between the two groups (Table 4). This result was in accordance with those of Stylianos et al., [12] ,their study included 48 patients with active pulmonary tuberculosis was divided into group A with low serum albumin and their mean serum albumin level was 2.95±0.91 and group B with normal serum albumin level and their mean serum albumin level was 3.92±0.6. TB can cause diverse laboratory abnormalities such as anemia, increased erythrocyte sedimentation rate and low serum albumin. Malnutrition per se had a more pronounced effect on serum albumin concentration in TB patients. Thus, all chronic infections such as TB can cause decrease production of serum albumin [13].In the present study, tuberculin skin test diameter in (group A) was ranging from 5-15mm with mean 7.5±3.94 and in (group B) was ranging from 12-30mm with mean 20.9±5.51. which showed statistically significant difference between the two groups (Table 5).This result was in agreement with those of Stylianoset al., [12] ,their study included group A with low serum albumin and their mean tuberculin skin test diameter was 11.3±2.1 and group B with normal serum albumin and their mean tuberculin skin test diameter was 18.4±3.9, the study showed statistically significant difference between the two groups . In our study there was a statically significant positive correlation between intensity of tuberculin skin reaction at 72 hours and serum albumin levels in both groups (Figure 1, 2).This result was in accordance with Kardjito and Donosepoetro, [14] who studied the mantoux test in tuberculosis, the result showed a statistically significant positive correlation between intensity of tuberculin skin reaction and serum albumin levels. -9- Also this result was in accordance with Michaelides et al., [15] who studied relationship between tuberculin hypersensitivity and serum albumin level in patients with pulmonary tuberculosis, their study included 42 patients (35 males and 7 females) aged 33.04±15.7. The diameter of induration was 17.8mm±6.01 and serum albumin levels were 7.27g/dl±0.86.Analysis showed a statistically significant positive correlation between intensity of tuberculin skin reaction and serum albumin levels. These findings indicated that tuberculous patients with lower albumin levels seem to react with weaker skin responses to tuberculin compared to those with rather normal albumin levels which could be explained by, malnutrition that cause suppression of delayed hypersensitivity reaction; false negative tuberculin reactions are very frequent in advanced malnutrition, malnutrition has been linked with decreased immune function[16]. CONCLUSIONS - Tuberculous patients with lower serum albumin levels react with weaker skin responses to tuberculin. As there was a significant positive correlation between intensity of tuberculin skin reaction at 72 hours and serum albumin levels REFERENCES 1. Kumar, Abbas Abul K, Fausto, et al. (2007): Robbins Basic Pathology (8th ed). Saunders Elsevier. PP. 516-522. 2. Castelo-Filho A, Kritski AL, Barreto AW, et al. (2004a): Consenso Brasileieiro de Tuberculose. J. Bras Pneumol, 30 (suppl 1): 557-586. 3. Chan ED, Heifets L, Iseman MD, et al. (2000 ): Immunologic diagnosis of Tuberculosis. Review Tuber Lung DIS, 80:131-40. 4. Jacobs JM. (2005): Utilizing human blood plasma for proteomic biomarker discovery. Journal of Proteome Research, 4(4): 1073-1085. 5. Finfer S, Bellomo R, McEvoy S, et al.(2006):Effect of baseline serum albumin concentration on outcome of resuscitation with albumin or saline in patients in intensive care units: analysis of data from the saline versus albumin fluid evaluation study. BMJ.333 (7577):1044. 6. World Health Organization Library Cataloguing in Publication Data. (2008): -10- Implementing the WHO stop TB Strategy: a hand book for national tuberculosis control programmes. WHO/ HTM/2008. 401. 7. Yassin MA and Cuevas LE. (2003): How many sputum smears are necessary for case finding in pulmonary tuberculosis? Trop. Med. Int. Health, 8: 927. 8. Topley WW and Wilson GS. (1990): Principles of bacteriology, virology and immunity, 8th. Arnold London Vol. (1): 76, Vol. (2): 74, Vol. (3): 105. 9. Yadolah (2003): The Oxford Dictionary of Statistical Terms. Oxford University Press. ISBN 0-19-920613-9. 10. Castelo-Filho A, Kritski AL, Barreto, et al. (2004b). The diagnosis of tuberculosis. Clin Chest Med 2005;26:247-71. 11. Gupta KB, Gupta R, Atreja A, et al. ( 2009): Department of Tuberculosis and Respiratory Medicine, Pt. Bhagwat Dayal Sharma post Graduate Institute of Medical Science, 26(1); 9-16. 12. Stylianos M, Vassilios C, Ioannis H, et al. (2010): Tuberculosis: metabolic insights, Tuberculin hypersensitivity and its relation to nutritional status in patients with active tuberculosis. 1st Dept. of Thoracic Medicine,School of Medical Assistants and Nursing. 13. Paton NI, Chua YK, Chee CBE, et al. (2004): Randomized controlled trial of nutritional supplementation in patients with newly diagnosed tuberculosis and wasting. Am J Clin Nutr, 80: 460-5. 14. Kardjito T and Donosepoetro M. (1981): The Mantoux test in tuberculosis: correlations between the diameters of the dermal responses and the serum protein levels. Tubercle, 62; 3135. 15. Michaelides Stylianos, Julia Vrioni, Aimslia Tsarouha, et al. (2005): Relationship between tuberculin hypersensitivity and serum albumin level in patients with active tuberculosis.American College of Chest Journal, 128(4):142s.doi. 16. Cegielski, JP and DNMC Murray. (2004): The relationship between malnutrition and tuberculosis: evidence from studies in humans and experimental animals. Int J Tuberculosis Lung Dis 8:286-298. -11-