File - Adair McIntyre
advertisement

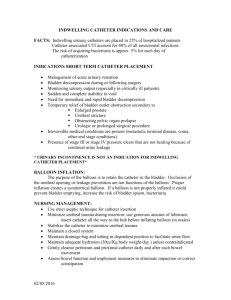
Running head: SAFETY AND QUALITY INDWELLING CATHETERIZATION Safety and Quality as it Relates to Indwelling Catheterization Adair L. McIntyre Ferris State University 1 SAFETY AND QUALITY AS IT RELATES TO INDWELLING CATHETERIZATION Safety and Quality as it Relates to Indwelling Catheterization Catheter-associated urinary tract infections (CAUTIs) occur when foreign bacterium is introduced to part of the urinary tract system. According to Fink et. al (2012), 34% of all health care associated infections in the United States are attributed to CAUTIs. Within the elderly population, UTIs can cause more damage and are the leading cause of systemic infections in this demographic (Taylor, Lillis, LeMone and Lynn, 2011). This paper will focus on the skill of insertion of an indwelling catheterization as well as the importance of sterile technique as it pertains to safety and quality measures when placing an indwelling catheter. The paper will also focus on the safety concerns which extend to after catheter insertion. Taylor et al. (2011) states one of the most important risk factors for CAUTIs is the length of time the catheter is in place. The longer the patient has an indwelling catheter, the more likely a CAUTI will occur. The evidence based safety measures that nurses follow allow the patient to receive quality care and more positive outcomes. According to Taylor et al. (2011), urinary catheterization is achieved by placing a tube directly into the bladder, which is naturally acidic and sterile, via the urethra. The bladder maintains an acidic environment to prevent infection from setting in; many bacteria cannot grow successfully in an acidic environment. The purpose of this procedure is to drain urine stored in the bladder (Taylor et al., 2011). Because having an indwelling catheter greatly increases the patient’s risk of infection, especially in the elderly population, the patient must meet certain criteria before a physician will place an order. A patient might require a catheterization placement to relieve urinary retention, monitoring a critically ill patient, obtaining a sterile urine specimen, or emptying the bladder throughout the surgical process (Taylor et al., 2011). However, these criterions are usually specific to the facility. 2 SAFETY AND QUALITY AS IT RELATES TO INDWELLING CATHETERIZATION When placing an indwelling catheter, there are several aspects of the procedure that require specific handling. Firstly, the entire process is sterile. The catheter kit should be sealed and remain unopened until the nurse is ready to perform the procedure. Once the package is opened, the sterile field should be maintained so cross contamination will not occur. The labia or the meatus and glans penis should be cleansed with antiseptic cleansing solution three times to effectively remove bacterium (Taylor et al., 2011). Any breach of sterility throughout this procedure could introduce bacterium to the bladder. Adhering to these evidence based safety concerns provides the highest quality of care to the patient. The patient is at the forefront of every action and decision the nurse makes. For example, when a catheter is placed out of necessity rather than convenience, the patient’s quality of care is positively impacted. The patient is also receiving high quality of care when a catheter is discontinued immediately after it is deemed medically unnecessary. A study (performed at Our Lady of the Lake Regional Medical Center (OLOL)) in 2010 examined the necessity of indwelling catheters (when present) once a new patient was admitted to the skilled nursing unit. When the nurse found the catheter was medically unnecessary and notified the physician for a discontinuation order, 50% of the time the physician stated they had forgotten the patient still had a catheter (Delatte, Alberato, Steele-Moses, and Murphree, 2010). In this case, the nurses were improving the quality of care by advocating for the health of their patients and avoiding unnecessary CAUTIs whenever possible. The systems theory examines how a whole entity is made up of smaller parts and how those parts work synergistically so the system can function as a whole. In the case of CAUTIs, when the bladder or kidneys are infected, the healing process slows down. The patient is presently in the hospital, so evidently their health is already compromised; now their body has to 3 SAFETY AND QUALITY AS IT RELATES TO INDWELLING CATHETERIZATION fight another infection. The system is not functioning correctly and individual parts cannot work together as efficiently so the body can attain freedom from infection. As previously discussed, when this infection occurs in elderly patients, the results can be devastating. Imogene King theorized that the patient is a system within their social system and therefore experiences the nurse, the health situation and reacts to everything (Taylor et al., 2011). When a patient’s discharge date is delayed because of a CAUTI, it can negatively impact their social and personal system. The patient may feel out of touch or be at risk for depression because they cannot experience their social system. In summation, CAUTIs are a very real and relevant problem within the health care system. These types of infections can be very serious and are the leading cause of illness among patients of all ages (Taylor et al., 2011). Also, a preventable infection can lead to a break down in the patient’s personal and social systems. Concern for the patient’s safety and quality of care are one way CAUTIs can be prevented. Advocating for the patient by questioning indwelling catheterization criterion, discontinuing the catheter as soon as its deemed medically unnecessary and performing the insertion procedure with sterile technique in mind are examples of how the safety concerns are being met and the patient is receiving high quality of care which in turn, produces more positive outcomes. 4 SAFETY AND QUALITY AS IT RELATES TO INDWELLING CATHETERIZATION References Delatte, H., Alberato, R., Steele-Moses, S., & Murphree, P. (2010). Decreasing urinary tract infections one indwelling catheter at a time: a hospital based skilled nursing unit performance improvement program. Pelican News, 66(4), 8. Fink, R., Gilmartin, H., Richard, A., Capezuti, E., Boltz, M., & Wald, H. (2012). Indwelling urinary catheter management and catheter-associated urinary tract infection prevention practices in Nurses Improving Care for Healthsystem Elders hospitals. American Journal Of Infection Control, 40(8), 715-720. doi:10.1016/j.ajic.2011.09.017 Taylor, C. R., Lillis, C., LeMone, P., & Lynn, P. (2011). Fundamentals of Nursing the Art and Science of Nursing Care (7th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. . 5 SAFETY AND QUALITY AS IT RELATES TO INDWELLING CATHETERIZATION 6