Correction of the dystrophin gene Jacques P. Tremblay Université

Correction of the dystrophin gene
Jacques P. Tremblay
Université Laval, Québec, Canada
Duchenne muscular dystrophy is due to mutations in the dystrophin gene. In
70% of the patients, the mutation is a deletion of one or several exons. In the remaining patients there are small point mutations, i.e., a deletion, an insertion or a modification of a few nucleotides. Most of the gene therapy approaches aimed to introduce the normal dystrophin gene to compensate for the mutated dystrophin gene. However, since the dystrophin gene is too big to be inserted in viral vectors, several investigators have generated truncated version of the dystrophin gene called mini-dystrophin or micro-dystrophin. The micro-dystrophin gene can be inserted in an adeno associated virus for a blood delivery of that gene.
An alternative approach to the introduction of a normal or truncated dystrophin gene is to correct the mutated dystrophin gene. Indeed since a few years, it is possible to design endonuclease enzymes to cut the DNA at a precise sequence of more than 18 nucleotides. There are 3 types of endonucleases, which have been used so far: the meganucleases, the Zinc Finger Nucleases (ZFNs) and the Tal
Effector Nucleases (TALENs). These enzymes can cut the dystrophin gene at a precise site. After the patients mutated dystrophin gene is cut by one of these enzymes, it is possible to correct the gene mutation by introducing the missing exons or by replacing the mutated nucleotides by providing a sequence of DNA that contains the correct sequence including sequences of homologies preceding and following the site of the cut. This type of reparation is called Homologous
Recombination. This type of reparation could be done in culture in the patient own myoblasts, i.e., the cells that form the muscle fibers. This would permit to transplant to the patients their own genetically corrected myoblasts and this would thus permit to avoid the use of a sustained immunosuppressive treatment required when the myoblasts of a healthy donor are transplanted.
It is also possible to use these precise endonucleases to cut the dystrophin gene in the exon, which precede or follow the patient deletion. The DNA cut can be repaired spontaneously by a process called Non Homologous End Joining (NHEJ).
This repair process is imperfect resulting in the insertion or the deletion of a variable number of nucleotides. One out 3 of these spontaneous repair which insert or delete a number of nucleotides adequate the restore the normal reading frame of the dystrophin gene. This would thus permit to restore the expression of a dystrophin protein, which would have the beginning and the end of the protein but would be missing an internal part due to the patient deletion.
This idea of restoring the expression of an internally deleted dystrophin gene is similar to the exon skipping strategy. However, since the endonucleases are correcting the gene (i.e., the DNA) rather than the messenger (i.e., the RNA), the correction would be permanent and thus the treatment would not have to be repeated as is the case for the exon skipping therapeutic approach.
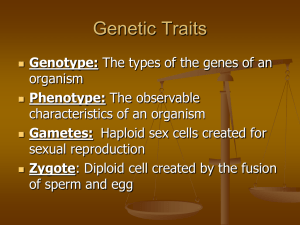
In the scheme above the dystrophin gene is cut by a pair of Zinc Finger
Nucleases (ZFNs). The dystrophin gene can be repaired by 2 different process: Non
Homologous End Joining or Homologous Recombination.
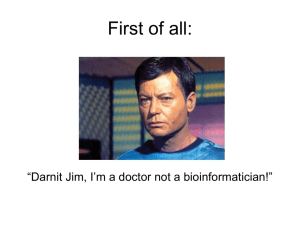
In the scheme above, the dystrophin gene in a Duchenne Muscular Dystrophy
(DMD) patient has a deletion of exon 53. This change the reading frame because this
exon does not contain a number of nucleotides, which is a multiple of 3. The normal reading frame of the dystrophin gene can be restored by inducing with a specific endonuclease a micro-deletion in exon 54 such that the total number of nucleotides deleted is now a multiple of 3 nucleotides.
These approaches of correcting the dystrophin gene with specifically designed endonucleases have been successfully tested in patient cells in culture. It will however take a few years before this can be tested in a clinical trial in Duchenne
Muscular Dystrophy patients.