CONSULTATION DRAFT Haemorrhoids Haemorrhoid symptoms
advertisement

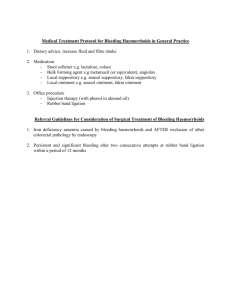
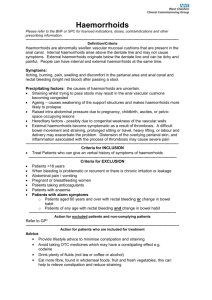
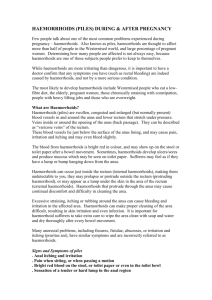
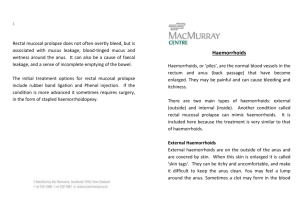
CONSULTATION DRAFT 6.2 Haemorrhoids Haemorrhoid symptoms are common in pregnancy, particularly in the second and third trimesters. Advice on avoiding constipation may assist women to prevent or lessen the effects of haemorrhoids. Topical products can be used to ease continuing symptoms. 6.2.1 Background Haemorrhoids are enlarged, swollen veins around the anus that are characterised by anorectal bleeding, painful bowel movements, anal pain and anal itching. While the mechanism is not clear, this is thought to be a result of prolapse of the anal canal cushions, which play a role in maintaining continence. Constipation (see Section 7.9 of Module I) is the major precipitating factor for haemorrhoids. Pregnancy also facilitates development or exacerbation of haemorrhoids, due to increased pressure in rectal veins caused by restriction of venous return by a woman’s enlarged uterus (Avsar & Keskin 2010). Incidence during pregnancy • Haemorrhoids that were present previously may become symptomatic for the first time in pregnancy. Haemorrhoidal symptoms are most common in the second and third trimesters of pregnancy and after birth (Avsar & Keskin 2010). • While estimates vary, it is thought that 25–35% of pregnant women are affected by haemorrhoids (Staroselsky et al 2008; Abramowitz & Batallan 2003). One observational study found that 8% of pregnant women (n=165) experienced thrombosed external haemorrhoids in the last 3 months of pregnancy (Abramowitz et al 2002). Diagnosis Pain with bowel movements, bleeding and itching are often the first signs and symptoms of haemorrhoids. Diagnosis is made by examining the anus and anal canal, usually by inspection. Digital rectal examination and endoscopy (sigmoidoscopy and colonoscopy) may also be used. It is important to rule out more serious causes of bleeding (Avsar & Keskin 2010). 6.2.2 Discussing haemorrhoids Summary of the evidence Treatment during pregnancy aims mainly to relieve symptoms and control pain (Avsar & Keskin 2010). Most evidence for the effectiveness of haemorrhoid treatments comes from studies of non-pregnant patients. Given the overall lack of evidence, there is consensus in clinical reviews for conservative management in pregnancy including avoiding constipation, dietary modification, dietary fibre supplementation and stool softeners (Avsar & Keskin 2010; Dietrich et al 2008; Wald 2003). Topical products with analgesics and anti-inflammatory effects provide short-term local relief of symptoms. There is no evidence on the effectiveness or safety of creams used in pregnancy; however, the small doses and limited systemic absorption mean that they are unlikely to harm the third trimester infant (Starolesky et al 2008). While surgical removal of haemorrhoids may be a consideration in extreme circumstances, surgery is rarely an appropriate intervention for pregnant women as haemorrhoidal symptoms often resolve spontaneously after the birth (Staroselsky et al 2008). Consensus-based recommendation vii Offer women who have haemorrhoids information about increasing dietary fibre. If clinical symptoms remain, advise women that they can consider using standard haemorrhoid creams. CONSULTATION DRAFT 6.2.3 Practice summary: haemorrhoids When: A woman had haemorrhoids before pregnancy or has symptoms of haemorrhoids. Who: Midwife; GP; obstetrician; Aboriginal and Torres Strait Islander Health Practitioner; Aboriginal and Torres Strait Islander Health Worker; multicultural health worker. Provide advice: Advise women that avoiding constipation (see Section 7.9 of Module I) is the best way to prevent and manage haemorrhoids during pregnancy and they should also try to avoid straining with bowel motions. Discuss treatments: Advise women that haemorrhoid creams can be used to further ease their symptoms. Take a holistic approach: Explore culturally appropriate, low cost ways for women to increase their fibre intake. 6.2.4 Resources NHMRC (2012) Australian Dietary Guidelines for Australian Adults. Canberra: Commonwealth of Australia. 6.2.5 References Abramowitz L & Batallan A (2003) Epidemiology of anal lesions (fissure and thrombosed external hemorroid) during pregnancy and post-partum. Gynecol Obstet Fertil 31(6): 546–49. Abramowitz L, Sobhani I, Benifla JL et al (2002) Anal fissure and thrombosed external hemorrhoids before and after delivery. Dis Colon Rectum 45(5): 650–55. Avsar A & Keskin H (2010) Haemorrhoids during pregnancy. J Obstet Gynaecol 30(3): 231–37. Buckshee K, Takkar D, Aggarwal N (1997) Micronized flavonoid therapy in internal hemorrhoids of pregnancy. Int J Gynecol Obstet 57: 145–51. Dietrich C, Hill C, Hueman M (2008) Surgical diseases presenting in pregnancy. Surg Clin North America 88: 403–19. Staroselsky A, Nava-Ocampo AA, Vohra S et al (2008) Hemorrhoids in pregnancy. Can Fam Phy 54(2): 189–90. Wald A (2003) Constipation, diarrhea, and symptomatic hemorrhoids during pregnancy. Gastroenterol Clin North America 32: 309–22.