Leukemias - Virtual Medic
advertisement

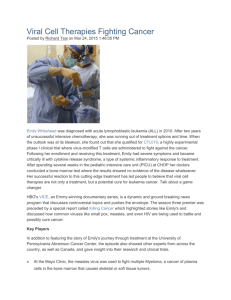
Leukemias CFU-Lymphocyte T T lymphocyte T lymphoblast T lymphocyte CFU-Lymphocyte B B lymphocyte B lymphoblast B lymphocyte CFS-Monocyte Myeloblast Promonocyte Monocyte CFS-G Myeloblast Promyelocyte Neutromyelocyte Stab Cell Neutrophil CFU-Eosinophil CFU-Eosinophil Myeloblast Promyelocyte Eosinophil Myelocyte Eosinophil Metamylocyte Stab Cell Eosinophil CFU-Basophils CFS-Basophil Myeloblast Promyelocyte Basophil Myelocyte Basophil Metamylocyte Stab Cell Basophil BFU-Erythrocyte CFU-Erythrocyte Basophilic Erythroblast Polychromatophilic Erythroblast Orthochromatophilic Erythroblast Reticulocyte Erythrocyte CFU-Megakaryoblast Megakaryoblast Promegakaryocyte Megakaryocyte Platelet Lymphoid Stem Cells CFU-GM Haemopoetic Pluripotent Stem Cell Myeloid Stem Cells L1 - Medium-sized homogenous blasts Acute Lymphoblastic Leukemia L2 - Heterogenous blasts cells Chronic Lymphocytic Leukemia L3 - Homogenous basophilic Burkitt-type blast cells Lymphoid Lineage M1 - Myeloblast without differentiation M2 - Myeloblast with evidence of maturation Leukemias M3 - Acute Promyelocytic Leukemia Acute Myeloid Leukemia M4 - Acute Myelocytic Leukemia Myeloid Lineage M5a - Monoblast Chronic Myeloid Leukemia M5 - Acute Monocytic/Monoblastic Leukemia M5b - Monocyte M6 - Erythroleukemia / Di Guglielmo's Syndrome M7 - Megakaryoblastic Leukemia FAB Classifications Morphology Etiology Clinical course Leukaemogenesis Clinical Manifestations Acute Lymphoblastic Leukemias (ALL) L1 L2 Medium-sized homogenous Heterogenous lymphoblasts lymphoblasts Some a marked, some a Immunologically nonmarking nonmarking Mostly marked as T cells Common in children Common in adult 85% cases of ALL 14% cases of ALL The best prognosis Bad prognosis As a result of genetic alterations within single cell in the marrow 1. Epidemiological evidence a. Hereditary’s Factors i. Fanconi’s anemia ii. Down’s syndrome iii. Ataxia telangiectasia b. Chemical agents i. Benzene ii. Phenylbutazone iii. Arsenic iv. Drug 1. Alkylating agent 2. Chloramphenicol 3. Antimetabolite c. Viral related i. HTLV1 ii. EBV 1. Acute clinical course with rapid development 2. ↓in one of more normal heamopoetic elements as bone marrow is overrun by leukemic cells a. Anemia i. Pallor ii. Hypoxic symptoms iii. Normochromic-normocytic RBC b. Thrombocytopenia i. Heamorrhage ii. Purpura c. Neutropenia i. Persistent infection 3. Metabolic imbalances a. Hyperuriceamia due to high cellular turnover 4. Generalized lymphadenopathy 5. Bone pain and tenderness 6. Gum hypertrophy 2. 7. 8. 9. L3 Homogenous basophilic Burkitt-type blast cells Mark as B cells Children I% cases of ALL (children) Worse prognosis Molecular Evidence a. Alteration in Oncogene i. Oncogene codes for protein involved in cellular 1. Proliferation 2. Differentiation ii. It is altered through 1. Chromosomal translocation 2. Point mutation 3. Inactivation Invasion of other organs a. Hyperluekocytosis leads to ↑in blood viscosity; predispose to i. Microthrombi ii. Acute bleeding b. Involved i. Brain ii. Lung iii. Eyes c. Injudicious use of packed cells transfusion worsen the blood viscosity Leukostatic tumour a. Lodging of blast cells in vessels forming a macroscopic pseudotumour; may erode the vessels b. Rare Hidden relapse sites a. Meninges b. Testes Acute Myeloblastic Leukemia (AML) FAB Classifications M0 o o o o Characteristics o o o o o Epedimiology M1 Minimally differentiated myeloblast Blasts are stained with Myeloperoxida se (MPO) PAS NSE Negative for all T & B cells antigens Platelets glycoproteins Erythroid glycophorin A Positive for all myeloid antigens CD13 CD33 CD11b 2-3% of incidence >90% are myeloblasts Myeloblast without differentiation 3% are stained with MPO CD8+ often seen M2 M3 30-90% are myeloblasts Myeloblasts with evidence of maturation 15-20% of incidence 10-15% of incidence T(15:17)(q22;q21 ) Fusion between o 17q21 transcribing for RARa gene o 15q22 transcribing for PML gene M4-Eo (with eosinophil) o Del/inv16q MYH1116p13 CBFbeta – 16q22 o Marrow eosinophil at about 6-35% Del (11q) t(9;11) t(11;19) Unrecorded o o 30-40% of incidence 15 % with t(8:21) CD13 Cytogenetic Aberration Clinical Manifestations o Unrecorded Markers 5-10% of incidence <35 years old CD34 CD33 Gum hypertrophy in M5 Mass effect on the eyes o Leukemic infiltration on the lower chamber of the eye obsecures the iris Chloroma in the eye in M2 Raised lesions on the tongue Acute Myelomonocytic Leukemia 20-80% are o Monocytes o Promonocytes Is believed to arise from CFU-GM ↑incidence of CNS involvement o o Divided into subtypes o M5a – monoblasts without maturation o M5b – monoblasts with differentiation (<5%) M7 Erythroleukemia/ Di Guglielmo >50% of all nucleated marrow elements are of erythroid precursors 30-50% more are of myeloblasts o <30% are myelodyspl asia <5% of AML cases (rare) <5% of AML cases (rare) t(1;22) Associated with 1. Gums a. Gum hypertrophy 2. Skin a. Eryhematou s skin rash b. Weakness c. Diffused bleeding M6 o M5 Acute Promyelocytic leukemia Promyelocytes characterized with Numerous darkly stained azurophilic granules Auer rod/faggot cells may be seen Classical hypergranular – 80% leukopenic Variant hypogranular – leukocytosis Granules contained procoagulant Leads to DIC o 20% of incidence M4 Acute Megakaryoblastic leukemia Associated with fibrosis Confirm origin with o Platelet peroxidase with Electron microscopy Methyleneblue/basic fuchsin/Azu re II (MAb) vWF glycoprotein CD33 CD13 Marked Petechiae Ecchymoses Pathologic fracture Periorbital bacterial skin infection Necrotic erythematous skin ulcer Brain infection o Aspergillosis Oral candidiasis Types of Leukemias Epidemiology Definition Precursors cells involved FAB classifications Morphology Clinical Features Acute Leukemias Acute Lymphoblastic Leukemia Less common Predominantly occurs in young children o Peak incidence at 3-4 years old Presence in the bone marrow an peripheral blood of uniform large cell That resembles the proliferating lymphoblasts in fetal development Lymphoblasts of lymphoid lineage L1,L2,L3 Fewer nucleoli Condensed nuclear chromatin Scanty rim of cytoplasm Cytoplasmic granules are absent Absence of Auer rod/faggot cells Presence of lymphadenopathy Absence of chloroma or granulocytic sarcoma Acute Myeloblastic Leukemia More common Predominantly occurs in young adults o Peak incidence at 15-20 years old Proliferation of cells of the granulocytes series usually Neutrophils Concomitant proliferation of basophils and eosinophils are uncommon Myeloblasts of myeloid lineage M0, M1, M2, M3, M4, M5, M6, M7 More prominent nucleoli Delicate/dispersed nuclear chromatin Fairly significant rim of cytoplasm Presence of azurophilc cytoplasmic granules Presence of Auer rod/faggot cells – a cytoplasmic inclusion Lymphadenopathy is usually absent Presence of chloroma or granulocytic sarcoma Chronic Leukemias Types of Chronic Leukemia Definition Morphology Staging/Phasing Epidemiology Chronic Lymphocytic Leukemia Proliferation of small mature lymphocytes Resemble that of resting lymphocytes in the peripheral blood 95% are of B cells lineage 5% are of T cells lineage Peripheral blood o Small round lymphocytes o Rim of cytoplasm o Smudged cells Bone marrow o Mature small lymphocytes infiltrating between residual normal heamopoetic elements Rai Staging* 1. Stage 0 a. Lymphocytosis only (>15,000/mm3) 2. Stage 1 a. Lymphocytosis b. Lymphadenopathy 3. Stage 2 a. Lymphocytosis b. Splenomegaly w/o hepatomegaly 4. Stage 3 a. Lymphocytosis b. Anemia (Hg <11g/dL) c. With or without i. Lymphadenopathy ii. Hepatosplenomegaly 5. Stage 4 a. Lymphocytosis b. Thrombocytopenia (Plt<100,000/UL) c. With or without i. Anemia ii. Lymphadenopathy iii. Hepatosplenomegaly *There’s another staging called The Binet Staging System Median age o 65-70 years old Sexual predeletion o Male to Female = 2 : 1 More common compared to CML Chronic Myelocytic Leukemia Proliferation of cells of the granulocyte series That have matured beyond the myeloblast stage Peripheral blood o Cells in all stages of granulocytic development o Myeloblast o Promyelocytes o Metamyelocytes o Myelocytes o Stab cells Bone marrow o ↑granulocytes and precursor blast cells o Small megakaryocytes Present with 3 phases according to occurrence 1. Chronic phase a. 1-5% of myeloblasts present 2. Accelerated phase a. 5-19% of myeloblasts present b. >20% basophils in the blood or bone marrow c. Platelet count <100,000, unrelated to therapy d. Platelet count >1,000,000, unresponsive to therapy e. Increasing splenomegaly or white blood cell count, unresponsive to therapy 3. Blast phase a. 20-30%* of myeloblast present i. *more than 30% of myeloblasts will fall into AML category b. Large clusters of blasts in the bone marrow on biopsy c. Development of a chloroma (solid focus of leukemia outside the bone marrow) Median age o SEA – 25-45 years old o Western world – 45-55 years old Incidence increase by age; 30% more than 65 y/o Sexual predeletion o Male to Female = 1.3 : 1 85% diagnosed during chronic phase Less common compared to CLL Types of Chronic Leukemia Chronic Lymphocytic Leukemia Aetiology Clinical features Diagnostic tools Chronic Myelocytic Leukemia Family history o 2-7 folds of risk No documented environmental factors No viral aetilogical evidence Genetic mutations o Del 3q14 o Del 11q22/ del 11q23 o Trisomy 12 (20-25%) Intermediate prognosis o Del in chrom 17 and 6 (less common) 20% are assymptomatic Herpes zoster viral infection o Infecting the 5th cranial nerve of V1 opthalmic nerve Herpes simplex eruptions on o Lips o Skin Extensive oral candidiasis Generalized lymphadenopathy Hepatosplenomegaly – splenomegaly tends to be extensively huge; due to o ↑sequestration of leukemic cells o Infiltration of leukemic cells Flow cytometry o CD19 w/o CD20 w Coexpressed with CD5 o Weak expression of surface Ig sIgM sIgD o May be expressed CD21 CD23 CD24 Bone marrow aspirates o Not require for diagnosis o For determining the extent of disease for prognostic implications Diffuse infiltration shows poor prognosis Other lab’s findings o Hypogammaglobulinaemia (>50%) o Small monoclonal peak (5-10%) o Positive Coomb’s test (30%) o Autoimmune hemolytic anemia (<10%) o Thrombocytopenia (<10%) Due to exposures of o Radioactive ray o Chemicals Benzene Found in byproducts of laser printers and copy machine Genetic mutations o Philadelphia Chromosome T(9:22), fusion of Moving ABL gene from 9p34 Fuse with BCR gene on 22q11 70% present with symptoms like o Fatigue o Abdominal discomfort o Weight loss o Sweating Hepatosplenomegaly – splenomegaly tends to be extensively huge; due to o ↑sequestration of leukemic cells o Infiltration of leukemic cells Left abdominal discomfort is due to spleen infarction caused by o Aggregations of granulocytes Retinal heamorrhage Hyperuriceamia ↑buffy coat in blood tube Flow cytometry Karyotyping **Pathogenesis in BCR-ABL translocation Translocation of BCR-ABL gene leads to 1. Encodes of protein a. BCR gene encodes for fusion protein b. ABL gene encodes for Tyrosine Kinase 2. In normal myeloid progenitor cell, it needs signal generation from GH in order to a. Proliferate b. Differentiate 3. But BCR-ABL gene tends to reduce the requirement of GH activation through a. Tyrosine kinase in which it generates constitutive signals b. These signals mimic in that of GH-factor receptor activation