Lecture 10
advertisement

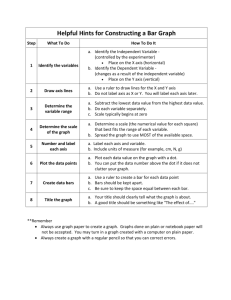
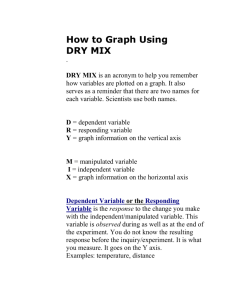
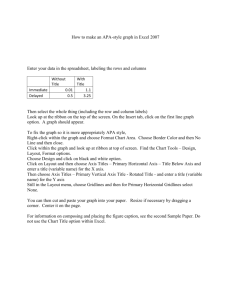
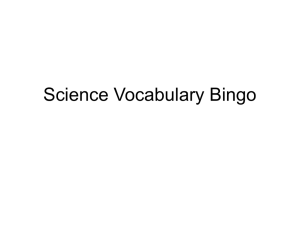
CARDIOVASCULAR PHYSIOLOGY Lecture 10 Axis of bipolar and unipolar limb lead Each lead is actually a pair of electrodes connected to the body on opposite sides of the heart, and the direction from negative electrode to positive electrode is called the “axis” of the lead. Lead I is recorded from two electrodes placed respectively on the two arms. Because the electrodes lie exactly in the horizontal direction, with the positive electrode to the left, the axis of lead I is 0 degrees. In recording lead II, electrodes are placed on the right arm and left leg. The right arm connects to the torso in the upper right-hand corner and the left leg connects in the lower left-hand corner. Therefore, the direction of this lead is about +60 degrees. By similar analysis, it can be seen that lead III has an axis of about +120 degrees; lead aVR, +210 degrees; aVF, +90 degrees; and aVL -30 degrees. The directions of the axes of all these leads is known as the hexagonal reference system. Figure1: the hexagonal reference system. Einthoven triangle. In 1901, Einthoven recognized that the heart possessed electrical activity, and he recorded this activity using two sensors attached to the two forearms. Einthoven proposed that the heart is located in the center of an equilateral triangle in the trunk. Such a triangle with the heart at its center can be approximated by placing electrodes one both arms and on the left leg. When these electrodes are connected, the border of triangle is formed which represents the three standard limb leads I, II, and III. The base of triangle formed by Lead I which connects the right and left arms, with its positive pole to the left, and its angle is zero(0˚). The other 2 border of triangle represent the axis of lead II and III, the Lead II connects the right arm and left leg, and its positive pole and orientation are downward and leftward and its angle is 60˚ and Lead III connects the left arm and right leg, and its positive pole and orientation are downward and rightward and its angle is 120˚. The relationship between the voltage of the complexes in the limb leads (‘standard leads’) is summarized by Einthoven’s law, which states that the net voltage of the complex in lead II equals the algebraic sum of the voltage in leads I and III (LII = LI + LIII). 1 Figure2: Einthoven triangle. Use of vectors to represent electrical potentials Depolarization of the myocardial cells generates electrical forces that move in three dimensions, changing direction continuously over the course of each heart beat. These forces collectively exhibit both magnitude and direction, constituting a vector. Clearly all the minute electrical forces generated by the myocardial syncytium cannot be considered individually, but they can be averaged together at any given moment during systole to identify a single net amplitude and direction called the instantaneous vector. Combining all the instantaneous vectors during systole into a single vector that represents the entire depolarization process results in the net or mean cardiac vector. To further simplify the process, the mean vector is calculated for only one plane in threedimensional space. The resulting vector is the mean QRS axis. Which consider as the mean electrical axis of the heart .Like other vectors the vectors the mean QRS axis is denoted in terms of degrees, the QRS vector of normal ventricles is at 59˚ and directed to the left. Figure3: the QRS axis(mean electrical axis of the heart). 2 Axis deviation Analysis of the axis may help to determine the location and extent of cardiac injury, such as ventricular hypertrophy, bundle branch block, or changes in the position of the heart in the chest (from, e.g., pregnancy or ascites). The average mean electrical axis of the heart (QRS vector of normal ventricles) is at 59˚, and directed to the left. However, the normal range of the axis of normal heart lie between - 30 and +90 degrees. The causes of this normal variations are mainly anatomical differences in the distribution of Purkinje system or in the musculature mass of the heart. When the heart axis lie between -30 to -90 degrees, the subject said to have left axis deviation and when the heart axis between +90 to +180 degrees. the subject said to have right axis deviation (RAD). Clinically, the electrical axis of the heart usually is estimated from the standard bipolar limb lead electrocardiograms . However, a quick estimate of the cardiac axis can be made by looking at leads I and aVF; in normal axis both Lead I and Lead aVF are positive, in left axis deviation Lead I is positive and Lead aVF is negative, in right axis deviation Lead I is negative and Lead aVF is positive, and in extreme right axis deviation both Lead I and Lead aVF are negative. Figure4: Normal axis and right and left axis deviation The common causes of left axis deviation (LAD)include: left bundle branch block left ventricular hypertrophy( LVH),horizontal heart; due to high diaphragm like ascites. Figure5: left axis deviation (Lead I is positive and Lead aVF is negative ) 3 The common causes of right axis deviation are ; right ventricular hypertrophy, right bundle branch block, lateral myocardial infarction,Pulmonary embolism, Dextrocardia, mechanical shifts or emphysema causing a vertical heart. Mild RAD is considered normal in children, adolescents, and young adults. Figure 6:right axis deviation (Lead I is negative and Lead aVF is positive). Change in the position of the heart in the chest. Under certain physiological condition the heart is angulated to the left or to the right, accordingly the mean electrical axis of the heart also shifts to the left or to the right. 1.physiological conditions that shift electrical axis of the heart to the left: (1)at the end of deep expiration. (2) when a person lies down, because the abdominal contents press upward against the diaphragm. (3) in stocky, fat people whose diaphragms normally press upward . (4) pregnancy. 2.physiological conditions that shift electrical axis of the heart to the right: (1) at the end of deep inspiration. (2) when a person stands up. (3) normally in tall, lanky people whose hearts hang downward. Conditions that cause abnormal voltages of the QRS complex I. Conditions that cause increased Voltage of the QRS complex 1.Left ventricle hypertrophy; commonly due to high blood pressure or aortic stenosis. The increased quantity of muscle causes generation of increased quantities of electricity by the heart . The ECG criteria for diagnosing LVH are increase R wave amplitude in left side leads and increase S wave amplitude in right side leads. Secondary ST segment and T wave abnormalities. Prolonged QR interval in V6. Figure 7:Left ventricle hypertrophy 4 2.Right ventricle hypertrophy(RVH) The common cause of right ventricle hypertrophy(RVH) is stenosis of pulmonary valve. Some of the generally accepted diagnostic criteria for RVH are shown below are: right axis deviation,. R:S ratio in V1 greater than 1.0 , deep S wave in V5 or V6 . (note: Patients with pulmonary hypertension or massive pulmonary embolus may exhibit S waves in all three standard leads – the S1,S2,S3 sign – an indicator of a poor prognosis in subjects with cor pulmonale). Figure 8:Right ventricle hypertrophy II.Conditions that cause decreased Voltage of the QRS complex The main conditions that lead to decreased QRS voltage. 1.diminished muscle mass due to series of myocardial infarction . This causes the depolarization wave to move slowly through the ventricles, consequently, there is prolongation of the QRS complex along with the decreased voltage. 2.Pericardial effusion. 3.Pleural effusion. 4.Pulmonary emphysema. 5