QME/AME Information Questionnaire - Pain & Headache Assessment
advertisement

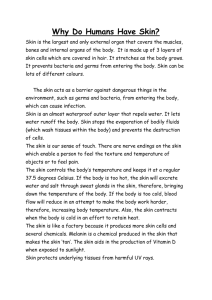
FIRST NAME: MI: LASTNAME: QME / AME INFORMATION QUESTIONNAIRE Wayne E. Anderson, D.O. A Medical Corporation Chronic Intractable Pain Disorders Headache & Facial Pain Disorders Neurotoxin Therapy You have an upcoming QME/AME appointment. During this appointment, we will discuss the history and impact of your injury. We then will perform a physical examination. Please note that the QME/AME appointment does not establish a physician–patient relationship and that no medical advice or prescriptions are provided. After your appointment, we will combine your medical records and the information you have provided to us and issue a report. In order for the report to be as accurate as possible, it is important that you complete this information to the best of your ability. This information must be completed before the appointment. Date of Birth: Date of Appointment: Board Certified Neurology American Board of Psychiatry & Neurology Board Certified Pain Medicine American Board of Psychiatry & Neurology in association with the American Board of Anesthesiology Subspecialty Certified Headache Medicine United Council for Neurological Subspecialties Qualified Medical Evaluator Member of the California Pacific Neuroscience Institute Date of Injury: Sex: Male / Female THE PROBLEM Where on the body is the problem? Please include right or left, front or back. When did the problem begin? How did it begin? (Accident, injury, unknown, etc.) If an accident or injury, please describe how the accident or injury happened: Correspondence to: 45 Castro Street Suite 225 San Francisco CA 94114 415.558.8584 tel 415.513.4521 fax www.wayneanderson.net How often does it occur? CONSTANT/INTERMITTENT/EPISODES If in episodes, how often? DAILY / WEEKLY / MONTHLY / OTHER: If in episodes, how long last? SECONDS/MINUTES/HOURS/DAYS/CONSTANT Progression of problem: STAYING SAME / GETTING BETTER / GETTING WORSE? Page 2 of 6 What makes it worse: UNKNOWN / STRESS / INCREASED ACTIVITY / OTHER: What makes it better: UNKNOWN / MEDS / REST / ICE / HEAT / OTHER: Please circle any words or phrases below that you associate with this problem. Not all persons will have these problems. WORSE WITH ACTIVITY/AVOID LOUD NOISES/AVOID BRIGHT LIGHTS/NAUSEA/VOMITING/SEEING FLASHING LIGHTS/NIGHTTIME/ TIGHT BAND/PULSATING/SPEECH PROBLEM / DIZZINESS /CHILLS/WAKES ME UP / SEX / ORGASM / MENSTRUAL RELATED/FEVER/ TEARING OR NOSE RUNNING/EYEBALL PAIN/ DOUBLE VISION / DEAFNESS / RINGING IN EARS /CAN’T WALK PROPERLY/CONFUSION/ PASSING OUT/BLINDNESS/TRUE WEAKNESS OR PARALYSIS/ FEELING OF WEAKNESS / NUMBNESS OR TINGLING IN ANY PART(S) OF THE BODY/ THIS PROBLEM RUNS IN THE FAMILY / PRIOR HEAD INJURY / PRIOR BRAIN PROBLEM Please circle any things below that you have done to diagnose or treat this problem. EMG / NCV / MRI / CT / XRAY / SPINAL TAP / EEG / OTHER DIAGNOSTIC TESTS: SURGERY / FACET INJECTIONS/EPIDURAL INJECTIONS/TRIGGER POINT INJ/BOTOX / SPINAL CORD STIMULATOR/TENS UNIT / MEDICATION / MEDITATION / YOGA / GYM/ HOME EXERCISE/ACUPUNCTURE/PSYCHOLOGY/CHIROPRACTIC/OSTEOPATHIC MANUAL TREATMENT/OTHER: Please tell us how severe your problem is, where 10 is the most severe anything could be: How severe is the problem in general? 0 1 2 3 4 5 6 7 8 9 10 MILD (HATE IT BUT CAN KEEP DOING THINGS) / MODERATE (SLOWS DOWN THINGS I TRY TO DO) / SEVERE (RESTRICTS MANY THINGS I TRY TO DO) / VERY SEVERE (HAVE TO STOP EVERYTHING ELSE) MEDICAL HISTORY Current medical conditions for which you are currently being treated or monitored: Past medical conditions (major things you had in the past but no longer have): Surgeries (please include the approximate year of surgery): Family history (please include things that run in the family if they are related to the injury): Social history: Alcohol PLEASE LIST YOUR ALCOHOL USE: Illicit drugs YES / NO? Smoking CURRENT / FORMER / NEVER? Abuse PHYSICAL ABUSE IN PAST / PHYSICAL ABUSE CURRENTLY (THIS IS A PAIN RISK FACTOR) Home ABLE TO TAKE CARE OF SELF-CARE / HAVE CARE GIVER / OTHER: Please do not write below this line. Please do not write below this line. Please do not write below this line. Page 3 of 6 Review of systems: THIS IS A LIST OF YOUR POSSIBLE CURRENT SYMPTOMS AT THIS EXACT TIME, NOT A LIST OF CONDITIONS THAT YOU MAY HAVE. For example, if you have asthma, you would list ASTHMA above under current medical conditions. If you are not having asthma problems today, you would not circle “wheezing” on the list below. But, if you ARE wheezing today, you would circle “wheezing” on the list below. Please circle any conditions that you are experiencing currently: ENERGY / SWEATING / BLEEDING / WEIGHT CHANGES / WORST HEADACHE OF LIFE / SINUS / STIFF PAIN (WHERE: ) NECK / MUSCLE SPASM / DOUBLE VISION / SENSITIVE TO LIGHT / VISION PROBLEMS / EYELID DROOP DISCHARGE (WHERE: ) / HEARING PROBLEMS / RINGING / HOARSENESS / CHOKING / CAN’T SWALLOW / DENTAL ISSUE / BAD TASTE / CAN’T TALK PROPERLY / WRONG HEARTBEAT / CONGESTED / SHORT OF BREATH / LUMPS (WHERE: ) COUGHING / WHEEZING / APPETITE PROBLEM / DIFFICULTY SWALLOWING / HEARTBURN / NAUSEA / LESIONS (WHERE: ) DIARRHEA / CONSTIPATION / CAN’T CONTROL BOWELS-INCONTINENT / BLOOD / ABNORMAL URINE SORES (WHERE: ) / CAN’T CONTROL URINE / PREGNANT / TRYING TO BECOME PREGNANT /WATER INTAKE / SWEATING / HOT FLASHES / FEEL WEAK / SEXUAL DIFFICULTY / BRUISING / STIFFNESS IN BODY PART SWELLING (WHERE: ) / CLICKING JOINT / GRINDING JOINT / CRAMPS / MUSCLES SHRINKING / DIZZY / FAINTING / BLEEDING (WHERE: ) CONCENTRATION / MEMORY LOSS / CONVULSIONS / ABILITY TO SMELL / ABILITY TO TASTE / BALANCE / COORDINATION / NEW OR UNEXPLAINED WEAKNESS / NEW OR UNEXPLAINED SENSORY LOSS / MOOD / SLEEP / BAD THOUGHTS / DANGEROUS THOUGHTS /SKIN SENSITIVITY / FINGERNAIL OR HAIR ISSUES / OTHER: MEDICATION HISTORY Allergies: Please list any medications or substances you are either allergic to or cannot tolerate. Please also list the reason why you cannot use the medication: Current medications: Please list your current prescription medications, over the counter medications, and supplements. You may attach a list if you like, but the list must include all six (6) columns listed below. Medication Size How taken Example: Aspirin 81mg 1 pill daily Example: Vicodin 5/500 1 every 4 hrs if needed If as needed, total in a day Average 3 per day Purpose Prescriber Prevent heart attack Dr. John Doe Knee pain Dr. Jane Doe Please do not write below this line. Please do not write below this line. Please do not write below this line. Page 4 of 6 Past medications: Although it may be difficult to remember things that you have tried for this condition, it is important that you do your best. Knowing what was tried and why it is no longer used can be helpful to determine what types of medications are appropriate and, obviously, to avoid retrying something that caused problems. Prior medication How long taken Why no longer used Example: aspirin 81mg Every day for 3 years Caused stomach bleeding STANDARDIZED QUESTIONNAIRES Please read this carefully. The following questionnaires are not written by us. They are standard questionnaires used to help validate your condition and your responses are especially important in work comp cases and legal cases. The questionnaires are not valid if you skip or change any questions. Therefore, please answer each question to the best of your ability, choosing the closest answer if there is no exact answer. Please note that you might not need to answer each questionnaire (see the top of each questionnaire). CHRONIC PAIN CLAIMS ONLY: PLEASE COMPLETE THE FOLLOWING SECTION Please circle a number for each of the pain words below. 0=don’t have it, 1=some, 2=more, 3=describes my pain a lot: 0123 Gnawing 0123 Splitting 0123 Burning 0123 Frightening 0123 Tender 0123 Throbbing 0123 Shooting 0123 Tiring 0123 Stabbing 0123 Cramping 0123 Heavy 0123 Cruel 0123 Aching 0123 Sharp 0123 Sickening HEADACHE CLAIMS ONLY: PLEASE COMPLETE THE FOLLOWING SECTION On how many days in the last 3 months did you miss work or school because of your headaches? (IF YOU DO NOT WORK OR GO TO SCHOOL, THE ANSWER IS ZERO) How many days in the last 3 months was your productivity at work or school reduced by half or more because of your headaches? (DO NOT INCLUDE DAYS COUNTED IN QUESTION 1.) On how many days in the last 3 months did you not do household work (such as housework, home maintenance, shopping, caring for children and relatives) because of your headaches? How many days in the last 3 months was your productivity in household work reduced by half of more because of your headaches? (DO NOT INCLUDE DAYS COUNTED IN QUESTION 3.) On how many days in the last 3 months did you miss family, social or leisure activities because of your headaches? TOTAL OF NUMBERS: Please do not write below this line. Please do not write below this line. Please do not write below this line. Page 5 of 6 ALL QME/AME CASES: PLEASE COMPLETE THE FOLLOWING SECTION For each question below, please choose a number from zero to ten (0-10) to let us know how much the pain affects your ability. For convenience, we have provided examples of what a ten would represent. Does your pain … Example of ten (10) …interfere with your normal work inside and outside the home? 0 1 2 3 4 5 6 7 8 9 10 Can’t work at all …interfere with personal care? 0 1 2 3 4 5 6 7 8 9 10 Need help with bathroom …interfere with traveling? 0 1 2 3 4 5 6 7 8 9 10 See doctors only …affect your ability to sit or stand? 0 1 2 3 4 5 6 7 8 9 10 Lay down always …affect your ability to lift objects off the floor, bend, stoop, or squat? 0 1 2 3 4 5 6 7 8 9 10 Cannot do at all, ever …affect your ability to lift overhead, grasp objects, or reach for things? 0 1 2 3 4 5 6 7 8 9 10 …affect your ability to walk or run? 0 1 2 3 4 5 6 7 8 9 10 In wheelchair only, can never walk or run …force you to see doctors much more than before your pain began? 0 1 2 3 4 5 6 7 8 9 10 See doctors every week …interfere with your ability to see the people who are important to you as much as you would like? 0 1 2 3 4 5 6 7 8 9 10 Never see people who are important to me 0 1 2 3 4 5 6 7 8 9 10 Can’t do any activities that are fun, ever 0 1 2 3 4 5 6 7 8 9 10 Lost ALL income 0 1 2 3 4 5 6 7 8 9 10 Every day 0 1 2 3 4 5 6 7 8 9 10 Need help with most everything all the time 0 1 2 3 4 5 6 7 8 9 10 Severe depression 0 1 2 3 4 5 6 7 8 9 10 Severe emotional problems …interfere with recreational activities and hobbies that are important to you? Has your income declined since your pain began (because of the pain)? Do you choose to take pain medication every day to control your pain? Do you need the help of your family and friends to complete everyday tasks because of your pain? Do you now feel more depressed, tense, or anxious than before your pain began? Do the emotional problems caused by your pain interfere with your family, social or work activities? Cannot do at all, ever Please do not write below this line. Please do not write below this line. Please do not write below this line. Page 6 of 6 ALL QME/AME CASES: PLEASE COMPLETE THE FOLLOWING SECTION For each of the ten (10) lines below, please circle the one (1) phrase that best describes your situation. It is understood that your situation may not be exactly like the phrases below, but please choose the one phrase in each line that is the closest to your exact situation. Please do not change any questions or skip any questions or the questionnaire will not be valid. 1 2 3 4 5 6 7 8 9 10 I can tolerate the pain without using pain killers I can look after myself normally without extra pain I can lift heavy weights without extra pain Pain does not prevent me walking I can sit in any chair as long as I like I can stand as long as I want Pain does not prevent me from sleeping well My sex life is normal with no extra pain My social life is normal and gives me no extra pain I can travel anywhere PAIN IS BAD BUT I MANAGE WITHOUT PAIN KILLERS I CAN LOOK AFTER MYSELF NORMALLY BUT IT CAUSES EXTRA PAIN I CAN LIFT HEAVY WEIGHTS BUT IT GIVES EXTRA PAIN PAIN PREVENTS WALKING MORE THAN 1 MILE I CAN SIT IN A SPECIAL CHAIR AS LONG AS I LIKE I STAND AS LONG AS I WANT BUT WITH EXTRA PAIN I CAN SLEEP WELL ONLY BY TAKING PILLS MY SEX LIFE IS NORMAL BUT CAUSES EXTRA PAIN MY SOCIAL LIFE IS NORMAL BUT CAUSES EXTRA PAIN I CAN TRAVEL Pain killers give complete relief from pain It is painful to look after myself and I am slow and careful I can manage heavy weights if conveniently positioned Pain prevents me walking more than 0.5 miles Pain prevents me sitting more than 1 hour Pain prevents standing for more than 1 hour Even with pills I have less than 6 hours sleep Sex life nearly normal but is very painful Pain limits some activities such as dancing PAIN KILLERS GIVE MODERATE RELIEF FROM PAIN I NEED SOME HELP BUT MANAGE MOST OF MY PERSONAL CARE LIGHT OR MEDIUM WEIGHTS IF CONVENIENTLY POSITIONED PAIN PREVENTS ME WALKING MORE THAN 0.25 MILES PAIN PREVENTS ME FROM SITTING MORE THAN 0.5 HOURS PAIN PREVENTS STANDING FOR MORE THAN 30MIN EVEN WITH PILLS I HAVE LESS THAN 4 HOURS SLEEP SEX LIFE IS SEVERELY RESTRICTED BY PAIN PAIN KEEPS ME FROM GOING OUT AS OFTEN WITH EXTRA PAIN Pain is bad but I manage journeys over 2 hours I ONLY DO TRIPS OF LESS THAN 1 HOUR i ii iii ANYWHERE BUT Pain killers give very little relief from pain I need help every day in most aspects of self-care I can lift only very light weights I can only walk using a stick or crutches Pain prevents sitting more than 10 minutes Can’t stand for more than 10 min Even with pills I have less than 2 hours of sleep Sex life is nearly absent because of pain Pain has restricted me to my home I only do necessary trips under 30 minutes Pain killers have no effect on the pain I do not get dressed wash with difficulty and stay in bed I cannot lift or carry anything at all I am in bed most of the time and crawl to the toilet Pain prevents me from sitting at all Pain prevents me from standing at all Pain prevents me from sleeping at all Pain prevents any sex life at all I have no social life at all because of pain Pain prevents me from traveling except to the doctor iv End of questionnaires. Thank you. Please do not write below this line. Please do not write below this line. Please do not write below this line. v