File

PATIENT NAME:
MR #:
SURGEON:
DATE OF SURGERY:
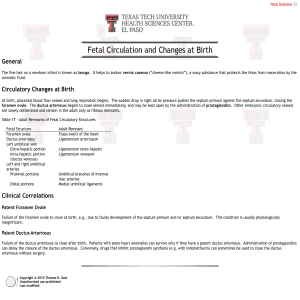
PREOPERATIVE DIAGNOSIS
Patent ductus arteriosus.
POSTOPERATIVE DIAGNOSIS
Patent ductus arteriosus.
NAME OF OPERATION
Ligation of patent ductus arteriosus.
Baby Girl Smith
12-34-56
Megan Lewis, MD
03/16/20XX
INDICATIONS
The patient is on day of life number 3, born at approximately 24+2 weeks estimated gestational age. She was intubated at birth and has remained in the neonatal intensive care unit in critical condition since the time of delivery.
Over the course of the last 12 to 16 hours, her oxygen requirements have increased and she has become more hemodynamically unstable. Echocardiography revealed a large patent ductus arteriosus, and the pediatric surgical service was consulted and requested to ligate the patent ductus arteriosus.
INFORMED CONSENT
Informed consent was obtained from the baby’s parents.
PROCEDURE
The patient was placed in the right lateral decubitus position, and her left hemithorax was prepared and draped in the usual sterile fashion. After induction of appropriate anesthesia, a left posterolateral thoracotomy was made in and carried down through the subcutaneous tissues to the level of the chest wall muscles. The chest wall muscles were split, and the 5th interspace was entered after division of the intercostal muscles. After adequate retraction of the lung utilizing brain spatulas, the ductus arteriosus was identified and dissected free of surrounding subcutaneous tissues. A trial closure of the dutus revealed no evidence of worsening hemodynamics, and a surgical clip was applied to the ductus arteriosus. This was accomplished without difficulty.
At this point the interspace was reapproximated utilizing two 4-0 Vicryl sutures in interrupted fashion. The chest wall muscles were reapproximated utilizing a single 4-0 Vicryl suture. The skin was closed in subcuticular fashion utilizing 5-0 Monocryl suture. It should be noted that prior to closing the incision, a 10-French chest tube was placed into the left hemithorax and positioned under direct visualization. The chest tube was brought out through the left anterior chest wall. The chest tube was secured to the skin utilizing a 5-0 Monocryl suture. The incision was closed utilizing a 5-0 Monocryl suture in subcuticular fashion, and the wound was dressed with Steri-Strips.
All sponge and needle counts were correct. The patient remained intubated in critical condition in the neonatal intensive care unit at the completion of the case.
COMPLICATIONS
There were no complications.
______________________
Megan Lewis, MD
ML/ps
D: 03/16/20XX
T: 03/16/20XX