paper_ed27_33[^]
advertisement

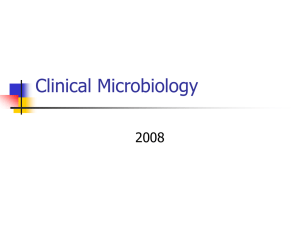
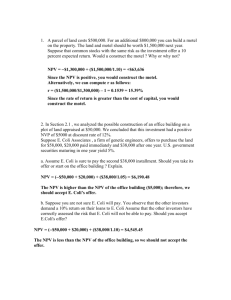
Journal of Babylon University/Pure and Applied Sciences/ No.(1)/ Vol.(22): 2012 College of Science/Babylon University Scientific Conference Survey of Antibiotic susceptibility of Escherichia coli Isolated from Patient with Significant Bacteriurea Jenan Mohammed Hussein Ali Almohana Department of Biology Department of Microbiology College of Education for Girls College of Medicin Eman Jar-Allah Kufa University, Department of biology sciences college / Babylon University Abstract Multiple resistances to antimicrobial drugs arising in Escherichia coli isolates may complicate therapeutic management of urinary tract infection (UTI) by this organism. In order to assess the multidrug resistance (MDR) among urinary E. coli isolates, we have tested 27 antimicrobial drugs against 192 isolates from patients with significant bacteriurea from 3 hospitals in Najaf during june to Augest 2011. The number of patients with urinary tracts infection was higher in females, 136 (70.9%) compared to males, 56 (29.1%). The antibiotic susceptibility patterns of isolates were determined by disk diffusion method. Among the isolates from the hospital patients, 95.3%, 94.3%, 93,8%, 92.2%, 91.7%, and 90.1% were resistant to carpencillin, ticarcillin, ampicillin, cefepim, cefamandol, and pipracillin, respectively; Resistant profile for cefoxitin, and amoxicillin was 85.4% and 80.2%, respectively. Uoropathogenic E. coli was resistant to cefotaxime, cefetriaxon, and Aztreonam (71.4%), and resistance to trimetheoprim, doxicycllin, ceftazidim, amoxiclave, and nalidixic acid were 69.8%, 68.2%, 68.8%, 67.2%, and 61%, respectively. susceptibility prfile to aminoglycosid antibiotics (tobramycin, gentamycin, and amikacin) were 56.8%, 53.1%, and 10.4%, respectively. And for fluoroquinolons (ciprofloxacin, norfloxacin, ofloxacin, and levofloxacin) were 49%, but for gatifloxacin, resistant was 40.6%. E. coli was resistance to chloramphenicol and nitroforantoin 17.7% and 12%, respectively.The high prevalence of drug resistance among UTI patients calls for continuous surveillance to assure effective control of this infection. 1. Introduction Urinary tract infections (UTIs) having as etiologic agent Escherichia coli are common infections with an estimated annual global incidence of at least 250 million cases, being costly to both patients and health care funding system (Ronald et al., 2001). Non-complicated infections, particularly in women, account for the highest number of UTIs. Women diagnosed for acute uncomplicated cystitis are usually treated as outpatients: the microbiologic characteristics of this infection are highly predictable even in otherwise healthy subjects. Physicians have therefore been advised that empirical antimicrobial treatment not requiring culture is appropriate in such cases (Hooton et al., 1997) Therefore, the empirical therapy has been so widely used that a few UTIs were routinely cultured. However studies clearly demonstrated an increasing antibiotic resistance in E. coli causing both community- and nosocomially acquired UTIs (Gupta et al.,1999 ; Gales et al., 2000). Updated knowledge of causal bacteria and their susceptibility patterns are important for proper selection and use of antibiotics as well as for an appropriate prescribing policy. The aim of the present study was to define current occurrence and phenotypes of multidrug-resistant (MDR) E. coli among UTI isolates from Najaf hospitals. 267 2 Material and Methods 2.1 Bacterial Isolates Escherichia coli isolates were identified depending on the traditional morphological and biochemical tests according to the methods of Cowan (1985), Holt et al. (1994), and MacFaddin (2000). (Table 2-1), and Media used in this study listed in Table (2-2) were prepared in accordance with the manufacturer's instructions fixed on their containers. All the media were sterilized in the autoclave at 121°C for 15 min Table (2-1): Phenotypic characterization of 117 E. coli isolated from urine samples of patients with significant bacteriuria % of positive results 100% 100% 0 0 100% 100% 0 0 3% 95% 100% 98% 36% 99% 100% Test Gram-negative bacilli Catalase Oxidase H2S Indole Methyl red Vogas-Proskaur Citrate utilization Urease Motility Acid from Glucose D-mannose Sucrose D-xylose Lactose Triple sugar iron agar acid/acid 100% Table (2-2): Culture Media Medium Manufacturer (Origin) Brain heart infusion broth and agar CHROMagar orintation Mast Diagnostic (UK) ChroMagar (France) Eosin methylen blue agar Himedia MacConkey agar Biolife (Italy) Muller Hinton agar Oxoid (UK) MR-VP broth Oxoid Peptone water Biolife Simmons citrate agar Mast Diagnostic Triple sugar iron agar Biolife 268 Journal of Babylon University/Pure and Applied Sciences/ No.(1)/ Vol.(22): 2012 College of Science/Babylon University Scientific Conference Table (2-3): Antibiotic disk Antibiotic name symbol Content Origin Ampicillin Am 10 µg Himedia (India) Aminopenicillin Amoxicillin Ax 25 µg Himedia Carboxypenicillin Carbenicillin PY 100 µg Himedia Piperacillin PRL 100 µg Bioanalyse (Turkey) Ticarcillin TIC 75 µg Bioanalyse Amoxi-clavc Ac Cefotaxime CTX 30µg Bioanalyse Ceftazidime CAZ 30µg Bioanalyse Ceftriaxone CRO 30 µg Bioanalyse Cephalosporin IV Cefepime FEP 30µg Bioanalyse Cephamycin Cefoxitin FOX 30µg Bioanalyse Cephalosporin I Cefamandole MA 30µg Bioanalyse Aztreonam AZT 30µg Bioanalyse Imipenem IPM 10µg Bioanalyse Amikacin AK 30µg Himedia Tobramycin TOB 10µg Himedia Gentamicin CN 10µg Bioanalyse Nalidixic acid NA 30µg Himedia Ciprofloxacin CIP 5µg Himedia Norfloxacin NX 10µg Himedia Ofloxacin OFX 5µg Himedia Levofloxacin Lev 5µg Himedia Gatifloxacin GT 5µg Himedia Folate pathway inhibitors Trimethoprim TMP 5µg Bioanalyse Tetracyclines Doxycyclin DO 30µg Bioanalyse Nitrofurans Nitrofurantoin F 300µg Bioanalyse Phenicols Chloramphenicol C 30µg Bioanalyse Antibiotic class Penicillin Antibiotic subclass Ureidopencillin -lactame/ß-lactamaseß inhibitor combinations Cephalosporin III Cephems (parenteral) Cephems (parenteral) Monobactams Penems Carbapeneme Aminoglycosides Quinolone 30µg Himedia Fluoroquinolone 269 2. 2 Susceptibility Testing Antimicrobial susceptibility was determined by the Kirby-Bauer disk diffusion method following the definition of the National Committee of Clinical Laboratory Standards (NCCLS) for agar diffusion tests (CLS, 2010) using antibiotic containing disks. Antibiotic disks listed in Table(2-3). Quality control was performed using E. coli ATCC 25922. An isolate was considered multidrugresistant (MDR) if it was resistant to at least three of the antimicrobial agents tested. 3 Results and Discusions 3.1 Survey and Etiological Agent According to demographic data, it was observed that the number of patients with urinary tracts infection was higher in females, 136 (70.9%) compared to males, 56 (29.1%) and statistical analysis showed high significance at (P ≤ 0.01) in female patients (Figure 3-1). The finding that females had higher prevalence of urinary tracts infection than males agrees with earlier studies (Anochie et al., 2001; Hadi, 2008; Mordi et al., 2010). The reason may be due to the higher number of the females than the males in the present study populations, or may be because those males are less potent UTI, possibly their longer urethra and the presence of antimicrobial substances in prostatic fluid (Orhiosefe et al., 2009). The high frequency of UTI in females, which might be due to diversity of factors related with females, such as the close proximity of the female urethral meatus to the anus and they lack the bacteriostatic properties of prostatic secretions (Lipsky, 1989; Akinloye et al., 2006). Alterations in vaginal microflora that play a critical role in encouraging vaginal colonization with coliforms that may lead to UTI (Hooton et al., 1997; Aiyegoro et al., 2007). In Nigeria, UTI is prevalent among men and women, but is more common among women, especially during pregnancy (Johnson et al., 1995). In agreement with present study, Todar (2002) reported that the UTIs are fourteen times more common in females than males by virtue of the abbreviated urethra. However, Ryan and Ray (2004) statement that UTI is more widespread in females, 40.0% of women have an episode in their lifetime. Sexually active females are also more predisposed to UTI than their male counterparts (Reid et al., 1987; Younis et al., 2009). In young sexually active women, sex is the cause of 75-90% of bladder infections, with the risk of infection related to the frequency of sex (Nicolle, 2008). The term "honeymoon cystitis" has been applied to this phenomenon of frequent UTI during early marriage. Male Female 70.9 29.1 Figure (3-1): The percentage incidence rate of urinary tract infection according to 270 Journal of Babylon University/Pure and Applied Sciences/ No.(1)/ Vol.(22): 2012 College of Science/Babylon University Scientific Conference sex. Nevertheless, in male UTI most commonly occur in older men with prostatic disease, outlet obstruction, or urinary tract instrumentation. In later life, UTI is more common among men until the age of prostatic hypertrophy (above 40 years of age) (Schroeder et al., 1990). An enlarged prostate means the gland has grown bigger. As the gland grows, it can press on the urethra causing obstructs the urethra, leading to increased difficulty in micturition. Because there is less urin flushing the urethra, there is a higher incidence of E. coli colonization (Nicolle, 2008). However, the infection occurs in all persons regardless of sex or age, with particular impact on the young and the very elderly (Rubin et al., 1986). 3.2 Survey of Susceptibility to Antibiotics Problems associated with the development and spread of antibiotic resistance in clinical practice have been increasing since the early 1960s and are currently viewed as a major threat to the public health on a global level (Ashraf et al., 2007; Levy et al., 2004). The prevalence of resistance among pathogenic bacteria also varies widely, among bacterial species and geographical regions, but it is raising enough to be considered a health threat (Amábile et al., 2009). In this investigation, all the 192 isolates of E. coli were tested for their antibiotic susceptibility to 27 antibiotics using Kirby-Bauer disk diffusion method on MullerHinton agar (Bauer et al, 1966), and were interpreted according to Clinical and Laboratory Standard Institute guidelines (CLSI, 2010). The antimicrobial potency of selected antibiotics against the E. coli is summarized in Figure (3-2). E. coli isolates from urine samples were frequently resistant to aminopenicillins including drugs commonly prescribed in the outpatients setting, including ampicillin (93.8%) and amoxicillin (80.2%) Several reports have indicated that these drugs were also less effective against E. coli and other bacterial agents isolated in previous studies in Najaf (Almohana, 2004; Hadi, 2008; Al-Hilali, 2010), largely because they are inexpensive and can be obtained easily without a medical prescription. Resistance is probably due to indiscriminate antibiotics usage (drug abuse) which could result in plasmid-mediated antibiotic resistance found to be common in E. coli (Taneja et al., 2008). In this investigation, the resistant effect of isolates to carboxypenicillins including carbenicillin and ticarcillin are comparable, the rates of resistance were 95.3% and 94.3%, respectively. The present results revealed high rate of resistant in E. coli isolates to carboxypenicillins, this rate is consistent with those reported by Al-Hili (2010) who found that 95% of E. coli isolates obtained from Merjan teaching hospital in Hilla to be resistant to carbenicillin. In recent study in Najaf, 90.9% and 86.4% of enteropathogenic E. coli isolates were found resistant to carbenicillin and ticarcillin, respectively (AlHilali, 2010). This high rate of resistant is probably due to the extensive use of β-lactam antibiotics in Najaf hospitals and the current empirical antibiotic therapy. Present study observed a high rate of E. coli isolates resistant to piperacillin (90.1%) E. coli is typically resistant to extended-spectrum penicillins, such as ampicillin and piperacillin, due to production of β-lactamase(s). The first plasmid-mediated βlactamase isolated from Gram-negative bacteria was TEM-1, described in E. coli, and mediates resistance to ampicillin, piperacillin, ticarcillin and first generation cephalosporins. 271 Unfortunately, resistance to amoxycillin clavulanic acid appeared first in E. coli isolates, then in other species of enterobacteria (Speldooren et al., 1998). This study permitted an evaluation of the frequencies of amoxyclave resistance in urinary isolates of E. coli in Najaf hospitals. The present result found that the majority of isolates (67.2%) were resistant to amoxyclave. This is often due to the production of excessive amounts of TEM-1 β-lactamase that swamp the activity of clavulanic acid (Bradford, 2001). However, carbapenemase and AmpC β-lactamases producing E. coli are not inhibited by the presence of clavulanic acid (Mirela and Ariana, 2011; Peter et al., 2011). Antibiotic susceptibility testing of isolates revealed high rate of resistance (91.7%) to second-generation cephalosporin including cefamandole. In the mid 1970s, the cefamandole (β-lactamase-stable cephalosporin compound) was marketed (Moellering et al., 1978). This antibiotic is a potent inducer, when E. coli isolates are exposed to two β-lactam antibiotics when of which is cefamandole, antagonism between the two antibiotics may result (Rao, 2006). In regards to third generation cephalosporins, results from Figure (3-2) revealed that E. coli isolates were highly resistant to cefotaxime (71.4%), ceftriaxone (71.4%), and ceftazidime (68.8%). The resistance to third generation cephalosporins was caused mainly by mutations in the common group of class A β-lactamases, which consisting of TEM, SHV and CTX-M β-lactamases that has extended hydrolytic spectrum activity on cephalosprins, The excessive use of expanded-spectrum cephalosporins in clinical practice is the main factor responsible for the appearance of ESBLs in the enteric bacteria and several studies have found a relationship between third generation cephalosporin use and acquisition of ESBL producing strains (Livermore et al., 1996; Kjerulf et al., 2008). Therefore, clinicians should be familiar with the clinical importance of these enzymes and potential strategies for dealing with them. In this study, the vast majority of E. coli isolates recovered from patients with significant bacteriuria was resistant to cefepime; the resistance rate was 92.2%. The present result was much higher than result recently conducted by Al-Muhannak (2010) who revealed that 63.5% of E. coli clinical isolates were resistant to cefepime. In Turkey, Kiremitci et al. (2009) found that high resistance rates for both E. coli and K. pneumoniae against cefepime (81.7%). However, an Australian study confirmed that more than 40% of Enterobacter spp. isolates from humans were resistant to cefepime. Therefore, present study concluded that treatment using fourth generation cephalosporins is also not recommended before the susceptibility testing is known. Aztreonam is used primarily as an alternative to aminoglycosides and for the treatment of aerobic Gram-negative infections. Approved indications for its use include infections of the urinary tract or lower respiratory tract, intra-abdominal and gynecologic infections, septicemia, and cutaneous infections caused by susceptible organisms (Scully and Neu, 1985). Beside, the present study revealed that 137 (71.4%) of 192 uropathogenic E. coli isolates recovered from patients with significant bacteriuria were resistant to aztreonam. The high rates of resistance might be as marker for the production of ESBLs by these isolates. Generally, an isolate is suspected to be an ESBL producer, when it shows in vitro resistance to the third-generation cephalosporins and to aztreonam (Samaha-Kfoury and Araj, 2003). However, clinical failure of cephalosporin and aztreonam therapy due to ESBLs is a growing problem in Najaf hospitals (Hadi, 2008; 272 Journal of Babylon University/Pure and Applied Sciences/ No.(1)/ Vol.(22): 2012 College of Science/Babylon University Scientific Conference Al-Muhannak, 2010; AL-Sehlawi, 2012) as they go undetected by current isolation and susceptibility tests. The major causes of cefoxitin resistant in E. coli are encoding of plasmid mediated AmpC β-lactamase or other factors might cause the reduce susceptibility of E. coli to cefoxitin (Tan et al., 2009). Present results revealed, the cefoxitin resistant E. coli isolates are disseminated in Najaf hospitals. This may due to the presence of contributed factors like; over expression of the chromosomeal ampC genes, acquisition of plasmidic ampC genes, porin or permeability mutations, or a combination of these factors (Mulvey et al., 2005) Carbapenems are considered the most potent agents for treating multi-drug resistant (MDR) Gram-negative bacteria the present study revealed that the most effective antibiotic in vitro among the uropathogenic E. coli isolates was imipenem. None of the isolates demonstrated resistance to this antibiotic (100% susceptible). The high efficiency of this antibiotic may be due to rarely usage in Najaf hospitals. Present results revealed that amikacin was the most prescribed empirical antibiotic followed by gentamicin and tobramycin. The results of this study also support the recommendation of the aminoglycoside, amikacin as suitable antibiotic for treating uropathogenic E. coli infections. In this study, the better activity of amikacin may be due to its less vulnerability to bacterial enzymes than other aminoglycosides. However, aminoglycosides like gentamicin and amikacin, which are known to have good coverage against P. aeruginosa, and other bacteria that resistant to other antibiotics are usually reserved for serious urinary tracts infection and used in combination with other antibiotics (Farrell et al., 2003). Nitrofurantoin is considered one of the oldest urinary anti-infective drugs in use, acts by inhibiting several protein synthesis-and-assembly steps at the ribosomal level. This drug remained the most active agent and as it can be administered orally and is highly concentrated in urine, it may therefore be the most appropriate agent for empirical use in uncomplicated UTI (Younis et al., 2009). Surprisingly, resistance to this drug remains minimal as seen in Figure (3-2), it seems that nitrofurantoin, because of the lower resistance in E. coli isolates as compared with other antibiotics, 273 Percentage 93.8 Am 80.2 AX 95.3 PY 94.3 TIC 90.1 PRL 67.2 AC 91.7 MA 71.4 CTX 71.4 CRO 68.8 CAZ 92.2 Fep 85.4 FOX 71.4 AZT 0 IPM 10.4 AK 56.8 TOB 53.1 CN 12 F 69.8 TMP 17.7 C 68.2 DO 61 NA 49 CIP 49 NX 40.6 GT 49 OFX 49 Levo 0 20 40 60 80 100 Figure (3-2): Susceptibility profil of E. coli for different antibiotics. Am: Ampicillin; Ax: Amoxicillin; PY: Carpencillin; TIC: Ticarcillin; PRL: Pipracillin; Ac: Amoxicillin MA: Cefamandol; CTX: Cefotaxime; CRO: Cefetriaxon; CAZ: Ceftazidim; Fep: Cefepim; FOX: Cefoxitin AZT: Aztreonam; IPM: Imipenim; AK: Amikacin; TOB: Tobramycin; CN: Gentamycin; F: Nitrforantoin TMP: Trimetheoprim; C: Chloramphenicol; DO: Doxicycllin; NA: Nalidixic acid; CIP: Ciprofloxacin; NX: Norfloxacin; GT: Gatifloxacin; OFX: Ofloxacin; Levo: Levofloxacin. can be considered as a good alternative therapy in E. coli urinary tracts infection in Najaf. This investigation also confirmed high resistant rate (69.8%) against trimethoprim. In agreement with present study, Hadi (2008) found that 60.5% of E. coli isolates recovered from patients with significant bacteriuria in Najaf were resistant to trimethoprim. In the UK, trimethoprim is usually recommended for empirical treatment of episodes of uncomplicated cystitis in the community (Baerheim et al., 2001). However, the major cause of trimethoprim resistance in Gram-negative bacteria is plasmid-borne dihydrofolate reductase (dfr) genes, which are commonly found as gene cassettes in class 1 integrons (Ashraf et al., 2007). 274 Journal of Babylon University/Pure and Applied Sciences/ No.(1)/ Vol.(22): 2012 College of Science/Babylon University Scientific Conference Present investigation showed that the other active antibiotic to treat infection caused by uropathogenic E. coli was chloramphenicol, with a resistance percentage of 17.7%. The low rate of resistance against chloramphenicol probably due to rarely use of this antibiotic to treatment of urinary tracts infection and other infections caused by E. coli. In this study, a relatively high occurrence of resistance in E. coli isolates was observed for nalidixic acid (61%). The resistant effect of isolates to fluoroquinolones including; ciprofloxacin, norfloxacin, ofloxacin, levofloxacin, and gatifloxacin are comparable, the rates of resistance were 49 % for ciprofloxacin, norfloxacin, ofloxacin, levofloxacin, whereas 40.6% of the isolates were resistant to gatifloxacin (Figure 3-2). Many factors may have contributed to such high rates of nalidixic acid resistance. These including misuse of antibiotic by health care professionals or non-skilled practitioners, misuse of antibiotic by the general public (antibiotic can be purchased in Najaf without a prescription), and may be inadequate surveillance due to lack of information arising from routine antimicrobial susceptibility testing, like reports from other developing countries (Oðuz and Bünyamin, 2004; Pittet et al., 2008). Refrences Ronald A.R.; Nicolle, L.E.; Stamm E.; et al. Urinary tract infection in adults: research priorities and strategies. Int. J. Antimicrob. Agents 2001;17:343-8. Hooton T.M., Stamm W.E. Diagnosis and treatment of uncomplicated urinary tract infection. Infect Dis Clin North Am 1997;11:551-81. Gales A.C., Sader H.S., Jones R.N., et al. Urinary tract infection trends in Latin American hospitals: report from the SENTRY antimicrobial surveillance program (1997-2000). Diag Microb Infect Dis 2000;44:289-99. Gupta K.; Hooton T.M.; Wobbe C.L.; et al. (1999). The prevalence of antimicrobial resistance among uropathogens causing acute uncomplicated cystitis in young women. Int J Antimicrob Agents;11:305-8. Cowan, S.T. (1985). Cowan and Steels Manual for Identification of Medical Bacteria. 2 nd ed., Cambridge Univ. Press, U.K. Holt, J.G.; Krieg, N.R.; Sneath, H.A.; Stanley, J.T. and Williams, S.T. (1994). Bergeys manual of determinative bacteriology.9th ed.,Baltimore;Wiliams and Wilkins, USA. MacFaddin, J.F. (2000). Biochemical tests for identification of medical bacteria (3rd ed.), Lippincott Williams and Wilkins, USA Clinical and Laboratory Standards Institute (CLSI). (2010). Performance standards for antimicrobial susceptibility testing; 20th . Informational Supplement. Approved standard M07-A8. Clinical and Laboratory Standards Institute. Anochie, I.C.; Nkanginieme, K.E.O. and Eke, F.U. (2001). The influence of instruction about the method of urine collections and storage on the prevalence of urinary tract infection. Niger J. Paediatr., 28: 39-42. Hadi, Z.J. 2008. Detection of extended-spectrum beta-lactamases of Escherichia coli and Klebsiella spp. isolated from patients with significant bacteriuria in Najaf. M.Sc. Thesis, College of Medicine. Kufa University. Mordi, R.M.; Osazuwa E.; Taiwo, S.S.; Alli, O.; Ogbolu, D.O.; Akanni, E.O.; Anukam, K.C. (2010). Klebsiella has taken lead among uropathogens in University of Benin Teaching Hospital, Benin City, Nigeria-An observation New York Science Journal;3(11) 61-64 275 Orhiosefe, O.; Lawrence, O.; Patience, U.; Gladys, I. (2009). Department of Microbiology, Ambrose Alli University, Ekpoma, Nigeria International Journal of General Medicine International Journal of General Medicine: 2 171–175 Lipsky, B.A. (1989). Urinary tract infections in men: Epidemiology, pathophysiology, diagnosis, and treatment. Ann Intern Med. 110:138–150. Akinloye, O.; Ogbolu, D.O.; Akinloye, O.M. and Terry Alli, O.A. (2006). Asymptomatic bacteriuria of pregnancy in Ibadan, Nigeria: a re-assessment. Br. J. Biomed. Sci., 63: 109-112. Hooton, T.M. and Stamm, W.E. (1997). Diagnosis and treatment of uncomplicated urinary tract infections. Infect. Dis. Clin. North. Am., 11:551-581. Aiyegoro, O.A.; Igbinosa, O.O.; Ogunmwonyi, I.N.; Odjadjare, E.E.; Igbinosa, O.E. and Okoh, A.I. (2007(. Incidence of urinary tract infections (UTI) among children and adolescents in Ile-Ife, Nigeria. African J. Microbiol. Res., pp: 013-019. Johnson, J.R.; Tiu, F.S. and Stamm, W.E. (1995). Direct antimicrobial susceptibility testing for acute urinary tract infections in women. J. Clin. Microbiol., 33: 23162323. Todar, K. (2002). Pathogenic Escherichia coli Todar's Oline Textbook of Bacteriology Ryan, K.J., and Ray, C.G. (2004). Sherries medical microbiology 4th ed. McGraw-HillNew York. S5-9. Reid, G.; Sobel, J.D. (1987). Bacterial adherence in the pathogenesis of urinary tract infection: a review. Rev Infect Dis.9:470–487. Nicolle, L.E. (2008)."Uncomplicated urinary tract infection in adults including uncomplicated pyelonephritis". Urol. Clin. North Am. 35 (1): 1–12. Younis, N.; Quol, K.; Al-Momani, T.; Al-Awaisheh, F.; Al-Kayed, D.J.; Nepal, M.A. (2009). Antibiotic Resistance in Children with Recurrent or Complicated Urinary Tract Infection; JNMA I, 48 ISSUE 173,48, (173):14-9. Schroeder, S.A.; Krupp, J.A.; Tierney, L.M.; Mephee, S.J. (1990). Current Medical Diagnosis and Treatment. New York, NY: Appleton and Lange, 622–628. Rubin RH, Tolkoff RNE, Contran RS. (1986). Urinary tract infections: pyelonephritis and reflux nephropathy. Pediatrics.83:1085–1141. Ashraf, M.A.; Yusuke, M.; Maiko, S.; Akito, M.; Hitoshi, W.; Yukio, F. and Tadashi, S. (2007). Zoo animals as reservoirs of Gram-negative bacteria harboring integrons and antimicrobial resistance genes. Appl. Environ. Microbiol., 6686–6690 Levy, S.B. (1992). Antibiotic resistance: microbial adaptation and evolution. In: The antibiotic paradox: how miracle drugs are destroying the miracle. New York: Plenum Press. Amábile-Cuevas, C.F.; Arredondo-García, J.L.; Cruz, A. and Rosas, I. (2009). Fluoroquinolone resistance in clinical and environmental isolates of Escherichia coli in Mexico City. J. Appl. Microbiol., 108: 158-162. Bauer, A.W.; Kirby, W.M.M.; Sherris, J.C. and Turck, M. (1966). Antibiotic susceptibility testing by a standardized single disc method. Amer. J. Clin. Pathol., 45: 493-496. Almohana, A.M. (2004). Prevalence and characterization of verotoxin producing Escherichia coli isolated from patients with diarrhea in Baghdad and Najaf. Ph.D. Thesis. Al-Mustansiryia University. 276 Journal of Babylon University/Pure and Applied Sciences/ No.(1)/ Vol.(22): 2012 College of Science/Babylon University Scientific Conference Al-Hilali, S.A.H. (2010). Occurance and molecular characterization of enteropathogenic Escherichia coli (EPEC) serotypes isolates from children with diarrhea in Najaf. M.Sc. Thesis, Kufa University, College of Medicin. Taneja, N.; Rao, P.; Arora, J., and Dogra, A. (2008). Occurrence of ESBL and AmpC βlactamases and susceptibility to newer antimicrobial agents in complicated UTI. Indian J. Med. Res., 127: 85-88. Al-Hilli, Z.B. (2010). Dissemination of β-lactamases in Escherichia coli and Klebsiella spp. isolated from Merjan teaching hospital in Hilla City. M.Sc. Thesis, Kufa University, College of Science. Speldooren,V.; Heym B.; Labia, R., and Marie-Helene, N.C. (1998). Discriminatory detection of inhibition-resistant B-lactamases in Escherichia coli by single- strand conformation polymorphism-PCR. Antimicrob. agents and chemother., 42 (4): 879889. Bradford, P.A. (2001). Extended-spectrum beta-lactamases in the 21 st century: characterization, epidemiology, and detection of this important resistancethreat. Clin. Microbiol. Rev., 14: 933-951. Mirela, F.; Ariana, A. (2011). Phenotypic methods for detection of beta lactamasemediated resistance in E. coli and Klebsiella pneumoniae Infectious Diseases Hospital Cluj-Napo XV, 15, N. 1/ 23 Iuliu Moldovan Str., Cluj-Napoca, Romania Peter, G.; Polsfuss, S.; Poledica, M.; Hombach, M.; Giger, J.; Böttger, E. C.; Zbinden, R., and Bloemberg, G.V. (2011), Detection of mpC beta-lactamase in Escherichia coli: comparison of three phenotypic confirmation assays and genetic analysis American Society for Microbiolog p 30/32. Moellering, A., and Jr R.C. (1978) Cefamandole-a new member of the cephalosporin family. J Infect Dis.;137 Suppl:S2-S9. Rao, A.N.; Barlow, M.; Clark, L.A. (2006). Class 1 integrons in resistant Escherishia coli and Klebsiella spp. US hospitals. Emerg. Infect. Dis., 12. 1011-1014 Kjerulf, A.; Hansen, D.S.; Sandvang, D.H.; Frimodt, M.N. (2008). The prevalence of ESBL-producing E. coli and Klebsiella strains in the Copenhagen area of Denmark. APMIS; 116:118-124. Livermore D.M.; Williams J.D. (1996). β-lactams: mode of action and mechanisms of bacterial resistance. In: Lorian V (Editor), Antibiotics in Laboratory Medicine. Baltimore, USA Al-Muhannak, F.H. (2010). Spread of some extended-spectrume ß- lactamases in clinical isolates of Gram-negative Bacilli in Najaf. M.Sc. Thesis, Kufa University, College of Medicin. Kiremitci, E.C.; Dinleyici, N.; Erben, G.; Durmaz, Z.A.; Yargic, A.D.; Aybey, G.; Usluer, E. O. ( 2009). In Vitro Activity of Ertapenem and Other Carbapenems Against Extended-Spectrum Beta-Lactamase Producing Escherichia Coli and Klebsiella Pneumoniae Clinical Isolates in a Tertiary Care Center in Turkey University Faculty of Medicine, Eskisehir, Turkey IMED, Australia pp.10 Scully, B.E.; Neu, H.C.; Am, J. (1985). Use of aztreonam in the treatment of serious infections due to multiresistant gram-negative organisms, including Pseudomonas aeruginosa.78(2):251-61. 277 Samaha-Kfoury, J. N., and G.F. Araj, (2003). Recent developments in ß-lactamases and extended spectrum ß-lactamases Br. Med. J. , 327:1209-1213. Al-Sehlawi, Z.S.R. (2012). Occurrence and characterization of AmpC Beta-lactamases in Klebsiella pneumoniae isolated from Najaf Hospitals. Ph.D. Thesis, College of Science, Babylon University. Tan, T. Y.; Yong, N.g.; He, L.S.; Koh, J.T.H., and Hsu, L.Y. (2009). Evaluation of screening methods to detect plasmid-mediated AmpC in Escherichia coli, Klebsiella pneumoniae, and Proteus mirabilis . Antimicrob. Agents Chemoth., 53(1): 146-149. Mulvey, M. R.; Bryce, E.; Boyd, D.A.; Ofner, A.M.; Christianson, S.; Simor, A.E.; Paton, S. (2004). Ambler class A extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella spp. In Canadian hospitals. Antimicrob. Agents Chemother., 48(4): 1204 Farrell, D.J.; Morrissey, I.; De Rubeis, D.; Robbins, M. and Felmingham, D. (2003). A U.K. multicentre study of the antimicrobial susceptibility of bacterial pathogens causing urinary tract infection. J. Infect., 46: 94. Baerheim, A.(2001).Empirical treatment of uncomplicated cystitis. BMJ,323:1197-1198. Oðuz, T.; Bünyamin, I. (2004). Increasing incidence of quinolone-resistant E. coli from urinary cultures in Ankara–Pursaklar region. International Journal of Antimicrobial Agents 23, 416–417 Pittet, D.; Allegranzi, B.; Storr, J.; Nejad, SB.; Dziekan, G.; Leotsakos, A.; Donaldson L. (2008). Infection control as a major World Health Organization priority for developing countries. Journal of Hospital Infection, 68:285-292. 278