ERCP: Endoscopic Retrograde Cholangiopancreatography Guide
advertisement

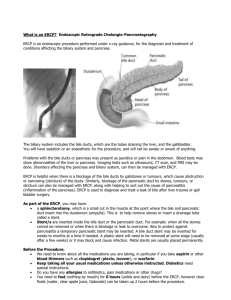
Endoscopic Retrograde Cholangiopancreatography ERCP During ERCP an X-ray is taken of the pancreatic duct and bile ducts. With newer diagnostic imaging technologies emerging, the diagnostic role of ERCP is diminishing and ERCP is evolving into a predominantly therapeutic procedure. Procedure The patient is sedated and given potent (opiate) pain relief after on overnight fast. A local anaesthetic is sprayed to the back of the throat. Using a modified endoscope, the ampulla of Vater is located and a thin catheter is passed through an opening in the endoscope and through the ampulla. A dye is then injected into the pancreatic and bile ducts, enabling images of these ducts to be obtained. Uses For many years ERCP was the investigation of choice for investigating pancreatic and biliary disorders. The availability of CT and MRI scan has now reduced the indications for investigation by ERCP. The following list of uses is taken from the US National Institute of Health guidelines1. Choledocholithiasis o Diagnosis of choledocholithiasis: magnetic resonance cholangiopancreatography2, endoscopic ultrasound and ERCP have comparable sensitivity and specificity. o Patients undergoing cholecystectomy do not require ERCP preoperatively if there is low probability of having choledocholithiasis. Laparoscopic common bile duct exploration and postoperative ERCP are both safe and reliable in clearing common bile duct stones. o ERCP with endoscopic sphincterotomy and stone removal is a valuable therapeutic modality in choledocholithiasis with jaundice, dilated common bile duct, acute pancreatitis or cholangitis. Benign strictures: o Strictures can initially be managed with intermittent biliary balloon dilatation at the time of ERCP or simple endoscopic stent placement. Pancreatic or biliary cancer o The main benefit of ERCP is palliation of biliary obstruction when surgery is not elected. In patients who have pancreatic or biliary cancer and who are surgical candidates, there is no established role for preoperative biliary drainage by ERCP. o ERCP the most commonly performed procedure for cholangiocarcinoma and can provide a tissue diagnosis through brush cytology of the bile duct. Relief from biliary obstruction can be provided with temporary plastic stenting or permanent metal stenting3. o Tissue sampling for patients with pancreatic or biliary cancer not undergoing surgery may be achieved by ERCP, but this is not always diagnostic. o ERCP is the best means to diagnose ampullary cancers. o Pancreatitis o ERCP has no role in the diagnosis of acute pancreatitis except when biliary pancreatitis is suspected. In patients with severe biliary pancreatitis, early intervention with ERCP reduces morbidity and mortality compared with delayed ERCP. o ERCP with appropriate therapy is beneficial in selected patients who have either recurrent pancreatitis or pancreatic pseudocysts. In patients with acute, relapsing and chronic pancreatitis a variety of endoscopic therapies can be performed. After pancreatic sphincterotomy, stones can be removed from the pancreatic duct, strictures can be stented. Peripancreatic fluid collections and pseudocysts can also be managed by pancreatic duct drainage or direct endoscopic cyst puncture and stenting techniques. Sphincter of Oddi dysfunction. Complications The main complications of the ERCP as a diagnostic procedure are pancreatitis, infection and bleeding4. The insertion of a therapeutic stent increases the risk of bleeding, pancreatitis, bile duct damage and leakage, and infection. Less than 1 in 10 patients will have such a complication and severe life-threatening complications only occur in 1-2% of patients. The risk of a complication when a sphincterotomy is not performed is less (2-5%) and depends on the number and size of the stents inserted. References Used 1. National Institute of Health; Statement on Endoscopic Retrograde Cholangiopancreatography (ERCP) For Diagnosis and Therapy. Volume 19, Number 1; January 14-16, 2002. 2. Health Technology Assessment; A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography. 2004; Vol 8: number 10. 3. Brugge WR; Endoscopic techniques to diagnose and manage biliary tumors. J Clin Oncol 2005 Jul 10;23(20):4561-5. 4. Freeman ML et al; Adverse outcomes of endoscopic retrograde cholangiopancreatography. Rev Gastroenterol Disord 2002 Fall;2(4):147-68. Internet and Further Reading OMNI: Cholangiopancreatography, Endoscopic Retrograde. Last issued 02 Nov 2005