A Multicenter Risk Index for Atrial Fibrillation After Cardiac Surgery
advertisement

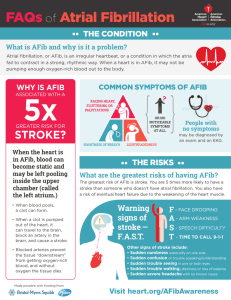
A Multicenter Risk Index for Atrial Fibrillation After Cardiac Surgery JAMA 2004;291:1720-29. Background -Worldwide 1 million CABG/year -Roughly 15% major adverse event (MI/CVA/ARF) -In 2002 – Database of over 5000 pt undergoing CABG in 17 countries created -Primary Purpose: Assess benefit of early ASA tx post CABG -Incidence Afib 27-40%; associated with CHF, renal failure, stroke, prolonged hospitalization -Goals: 1. Identify factors a/w AFib and derive Risk Index to predict onset of AF post-op. 2. Identify adverse outcomes a/w AF Methods -Prospective, observational study -Inclusion: 5,436pts, 70 hospitals, 17 Countries; scheduled CABG 1996-2000 +/- valve surg, on pump -Exclusion: Pts undergoing CEA, pts with chronic AF -Database - 7500 fields data per patient (demographics, history, imaging/Echo; intraop and post-op variab) -Assessed for adverse outcomes -AF – included aflutter. Detected on monitor/12-lead or PE -MI, CHF, CVA, renal failure Statistics - χ2 test for categorical values; t-test contin vals - AFib Risk Index 1. Used first 2/3 patients to derive Index 2. Identified risk factors a/w afib, after multivariate analysis, kept factors significant with p<.01 3. Calculated relative weights of each factor and assigned relative points to create Risk Index 4. Used last 1/3 patients to evaluate model (ROC) (ROC Curves, an aside) Results Patients: -Av Age 64, 80% male, 92% white -30% DM, 68% HTN, 9% prior AF -6%CABG,40% ACE,64% B-blk,32%CCB Incidence AF: 32%. 43% > 1 episode 22% > 2 episod; Usu 2 days post-op -Table 2: Sig independent predictors + protective factors, relative risk points assigned to e/ predictor -AF Risk Index calculated by adding risk points -Area under ROC curve using validtn cohort: 0.77 Adverse Outcomes a/w AF (Table 4):- Cognitive Changes, ARF, sepsis; death 4.7% vs 2.1% (p< 0.001) - longer hospital stay (2d) more rehab, more resources on testing Negative Association: MI/CHF/IABP use Discussion -AF is very common post CABG and a/w adverse outcomes and increased use of resources\ -Association does NOT equal causality -Adverse outcomes due to afib or sicker, older patients get afib AND independently have adv outcomes -“Does preventing AFib prevent adverse outcomes a/w afib” -Need prospective randomized studies -This study theory generating: use of ACE, amio, NSAID perioperatively -Is afib “protective” for MI/CHF? -Should we calculate AF risk index score on our patients going to CABG? Marco Perez, Journal Club, Nov. 16, 2004 1 Receiver Operator Characteristic Curves – An Aside Derived from Signal Detection Theory developed during WWII for reading of radar images. Radar (Receiver) Operators had to decide if blips on screen were enemy targets/friendly ships or noise. Statistical methods to analyze how well the Receiver Operators made these distinctions were devised. Their abilities to do so became the Receiver Operator Characteristics Tests are not 100% accurate. For any given test result, there will be an overlap of patients with and without disease. For tests that can produce continuous variable, sensitivity and specificity are going to depend on threshold value chosen for positivity or negativity of test. The less strict the threshold, the higher the sensitivity, but the lower the specificity. (ex, if we lower our threshold Tpn T value for MI to 0.04 instead of 0.09, then we’ll “catch” more true MIs, but at the same time we’ll incorrectly label other patients as having MI) If you plot the Sensitivity and 1-Specificity for different threshold values, create ROC curve The closer to the upper left border, the more accurate the test. The area under this curve can be measured. The closer to 1.0, the more accurate the test. This same method has been validated for prediction rules, such as AF Risk Index. Areas under the ROC Curve: Marco Perez, Journal Club, Nov. 16, 2004 .90-1 = excellent (A) .80-.90 = good (B) .70-.80 = fair (C) .60-.70 = poor (D) .50-.60 = fail (F) 2