Paper_Prof_Wang_final1[1]

Chronic intestinal ischemia in two patients with multiple possible presentations: Case report
Wang Zhong GAO, MD. FICA, FACA, FSVS.(USA) Distinguished Fellow of Society of
Vascular Surgery of USA
Author for correspondence: Zhong Gao Wang, MD
M.R.Kotwal MD, FACG (Usa), MRCP (London), FRCP (Edin). Medical Adviser
Government Of Sikkim India.
Corresponding Address: Xuan Wu Hospital and Vascular Institute, Capital University of
Medical Sciences, Beijing, 100053, China. Tel/Fax: 86106304 7006
E-mail: wzg@public3.bta.net.cn
, zhonggaowang@yahoo.com
SUMMARY
Arterial insufficiency or ischemia produces the target tissue or organ hypoplesia even necrosis. The first author had a case of mesenteric insufficiency and remarkable hypoplesia of the intestinal wall.
(1)
In contrast to a recently treated patient with chronic mesenteric insufficiency in whom, instead a remarkably distinctive intestinal wall hyperplasia with smooth serosa, without any other intestinal lesion was seen. With same etiology in two different patients varied outcome is rather perplexing. Could it be that different layers or part of layers of intestine behave differently to ischemic insult?
Intestinal ischemia.
Acute or chronic abdominal pain can be the result of many different pathophysiological processes. Many presentations are due to benign processes, whereas others may be life threatening if not recognized swiftly. Among the many possible causes, clinicians need to consider the possibility of intestinal ischemic disorders. The variable vessels involved, location of bowel affected, and different levels of acuity of illness all result in multiple possible presentations. The detection of such a serious condition can be a diagnostic and therapeutic dilemma.
(2)
Acute mesenteric ischemia.
The recognition of acute mesenteric ischemia can be difficult, as most patients present with non-specific symptoms, particularly abdominal pain. Classically, pain is disproportionately exaggerated relative to the unremarkable physical findings and persists beyond two to three hours. However, signs of an acute abdomen with distension, guarding (rigidity), and hypotension may also occur, particularly when diagnosis has been delayed.
(3)
The underlying process can involve emboli, arterial or venous thrombosis, vasoconstriction from low flow states or vasculitis. Embolic occlusion of the superior mesenteric artery occurs in > half of all cases.
(4)
. Most emboli originate in the heart and are potentiated by cardiac arrhythmias or depressed systolic function due to ishaemic heart disease.
Case Report.
A 65 years old male patient was admitted to our hospital due to severe acute abdominal pain and nausea with out vomiting for 3 days on 6 th
Feb 2004.On clinical examination abdomen was soft and bowel sounds were present. The white cell count was
11,200/cmm. LDH was 433 IU/L. Plain abdomen X-Ray revealed intestinal distension in
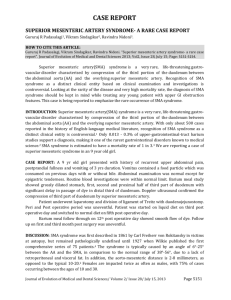
the right half of abdomen. Stool was positive for occult blood. He did not give past history of any GI symptoms, intermittent abdominal pain, diarrhoea and, constipation or weight loss. He had past history of atrial fibrillation for 8 years. Selective superior mesenteric arteriography showed filling defect at its root with poor blood flow and an occlusion at the distal ileocolic artery. Collaterals between the common hepatic artery and SMA could be seen (fig 1). A diagnosis of acute mesenteric embolism was made and an immediate SMA embolectomy was planned. However his attending surgeon decided to do laparoscopy. No bowel necrosis was found on laparoscopy. He was managed conservatively. Nil orally, intravenous perfusion and gastrointestinal decompression. He was perfused 250,000 IU of urokinase via the angiographic catheter inserted into the
SMA for angiography and the catheter was with drawn. He was better for some time and discharged on 16 th
Feb.
Fig 1. Superior mesenteric arteriography with filling defect at the root of SMA and an occlusion of the distal ileocolic artery. Collaterals between hepatic artery and SMA seen.
On 22 nd
Feb he was readmitted with intolerable abdominal pain for nearly 16 hours. He had temperature 38.1C, X- Ray abdomen showed multiple air fluid levels. Again he was treated conservatively in hospital till 27 th
May. He lost 13 Kg of weight. At this point of time the family approached the first author who initially wanted to treat him surgically i.e. SMA embolectomy. Thrombus with partial fibrosis was attached to the wall of artery.
Surgical embolectomy of the SMA was completed. Approximately 40- 60 Cms long
ileum sausage-in consistency like a good real sausage feeling and cyanotic in color with very smooth serosa at about 50 cm proximal to Caecum was found. Proximal intestine was slightly dilated, and no other intestinal and peritoneal lesions were found. The diseased segment of ileum was then removed and end- to- end anastomosis carried out.
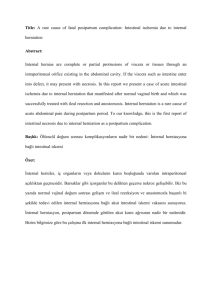
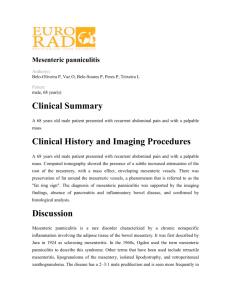
The removed ileum wall was markedly thickened, hypertrophied without irregular appearance and with a very narrowed lumen (fig 2). Histopathological report was “ an unusual widening in the layers of submucosa and serosa with fibrous proliferation and cell infiltration mainly lymphocytes and plasma cell (fig 3). No specific diagnosis could be made out pathologically.
The patient had an uneventful recovery and discharged after 10days. Follow-up six months later the patient was completely asymptomatic and had gained 12 kg weight.
Fig 2. Intestinal wall hypertrophy with mesenteric involvement and narrow lumen.
Fig 3. Widening of the submucosal (left) and adventitious layers (right) with fibrous tissue proliferation. Infiltration of lymphocytes and plasma cells (x 10; Pathology No.
156108)
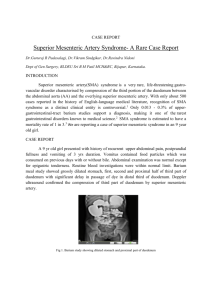
2nd patient.
Another patient 69 years old women had repeated abdominal pain and lower gastrointestinal bleeding for one and half year. She was anemic (HB 4g%) and had lost 8
Kg weight. Angiography showed an occlusion of superior mesenteric artery (SMA) and formation of a huge Riolan’s arch. During surgery intestinal wall was found very thin, as thin as layers of paper in some areas, light of colonoscopic illumination could easily be seen from the lumen of intestine. After aorto-superior mesenteric artery (SMA) bypass, the SMA pulsation could then be felt and seen as intestinal wall became thicker.
Postoperative recovery was uneventful. She became asymptomatic, gained weight of 5
Kg and HB rose to 10g% at 4 weeks and was discharged.
(1.)
Discussion.
The diagnosis of intestinal ischemia begins with the ability of the clinician to suspect and recognize it. The clinical history of abdominal pain and non-specific findings may be misleading. However, common clinical conditions should be quickly excluded and mesenteric vascular disease aggressively pursued. Traditionally, conventional angiography has been regarded gold standard imaging method. Approximately 90% of patients with acute mesenteric ischemia who undergo angiography before the onset of peritoneal signs survive, demonstrating the value of angiography and early diagnosis.
Advantage of angiography includes the ability for concomitant endovascular treatment.
Multiple therapeutic approaches are available for intestinal ischemia, depending on acuity and extent of disease. Resection of infracted bowel as well as embolectomy can be accomplished during surgery.
Mesenteric ischemia accounts for approximately 0.1% of hospital admissions and is found in1 % of patients with acute abdomen.
(5)
The non-specificity of clinical signs and symptoms associated with the early stages of ischemia often delays diagnosis until extensive and irreversible bowel infarction has occurred. These delays in diagnosis substantially contribute to the poor prognosis associated with this disorder, with mortality
rates exceeding 60%,
(6,7)
. In our case unnecessary delay increased morbidity of the patient though this patient was lucky to have uneventful recovery after surgery.
Mesenteric ischemia most often results from SMA embolization or thrombosis, and less commonly, venous occlusion or nonocclusive process. Remobilization of the SMA accounts for nearly 50% of cases, with thrombosis responsible for another 25% of cases.
(8,9) Early identification of the disorder requires a high index of suspicion in patients with significant risk factors, such as congestive heart failure, cardiac dysrythmias, recent myocardial infarction, severe valvular heart disease, generalized atherosclerosis, intraabdominal malignancy, previous atrial emboli, pancreatitis or hemorrhage.
(8,9)
In our case it was perhaps atrial emboli.
In terms of clinical presentation, mesenteric ischemia may present with increasing abdominal pain and decompensation over a period of hours or with symptoms progression over several days. Abdominal pain is the most common symptom. It occurs in over 75% of patients and varies in severity, nature, and location
(9)
Pain is often associated with vomiting, diarrhea and fever.
(10)
Unfortunately, despite these symptoms, clinical examination of the abdomen is often normal. Evidence of generalized or localized peritonitis may not be evident until infarction has occurred. Other late signs include hematochezia, hematoemesis, positive fecal occult blood testing, massive abdominal distention, back pain, hypotension, and shock,
(9)
.
Findings on plain abdominal X-Ray are normal or nonspecific in more than 25% of cases of early mesenteric ischemia,
(8,9) this was true for our first case as well. Thrombolytic therapy may benefit selected patients with early diagnosis of SMA thrombosis unassociated with bowel necrosis. Conservative treatment with thrombolytic therapy did not help our patient. In fact unnecessary delay could have jeopardized patient’s survival.
In most cases, as in our both cases surgical exploration was emergently performed to restore intestinal arterial flow and resect irreparably damaged bowel. Very thin ischemic hypotrophied bowel in second case is in contrast to the first case where ischemic bowel segment was remarkably thickened or hypertrophied with smooth and normal serosa without any other lesions. We fail to understand as to why in two cases where same etiology of mesenteric ischemia could lead to different pathological processes?
References.
1 Wang ZG, Tseng XJ. Acute mesenteric insufficiency. Chin J Surg 1985; 284 –
288.
2 Diagnosis and management of intestinal ischemic disorders. Jayaprakash
Sreenarasimhaiah BMJ Vol. 21 June 2003,1372 –1376.
3 Edwards MS, Cherr GSCraven TE, Olsen AW. Plonk GW.Geary RL, et alAcute occlusive mesenteric ischemia: Surgical management and out comes. Ann vasc.surg 2003.17.72-79
4 Brandt LJ, Boley SJ. AGA technical review on intestinal ischemia.
Gastroenterology 2000; 118:954-68
5 Klein H, Lensing R, klosterhalfen B et al. diagnostic imaging of mesenteric infarction. Radiology.1995; 197: 79-82.
6 Horton KM, Fishman EK. Multi-detector row CT of mesenteric ischemia: Can it be done? Radiographics.2001; 21: 1463-1473.
7 Kaufman SL, Harrington DP, Siegelman SS. Superior mesenteric artery embolization: An angiographic emergency. Radiology. 1977: 124:625-630.
8 McKinsey JF, Gewertz BL. Acute mesenteric ischemia. Surg Clin North Am.
1997; 77: 307-318.
9 Kaleya RN, Sammartano RJ, Boley SJ. Aggressive approach to acute mesenteric ischemia. Surg Clin North Am. 1992; 72: 157- 182.
10. Heys SD, Brittenden J, Crofts TJ. Acute mesenteric ischemia: The continuing
difficulty in early diagnosis. Postgrad Med J. 1993; 9:48-51.