Review article - The Ethiopian Journal of Health Development
advertisement
Review article Risk factors for acute lower respiratory infections in under-five children in Addis Ababa, Ethiopia Derege Kebede1 Acute respiratory tract infections (ARI), and more importantly acute lower respiratory tract infections (ALRI), are now recognized as major global health problems (1,2). Control strategies for ALRI include case management of affected children, immunization and modification or reduction of risk factors (3). Risk factors for ALRI can be categorized on three levels: on the societal level there are risk factors such as socio-economic level of a community; on the household level factors such as parental characteristics, household size and income, and indoor air pollution; and on the individual level characteristics of children such as the presence of malnutrition (protein-energy and micro-nutrient deficiencies) and immunity to micro-organisms (4). Risk factors on the household and individual levels are potentially modifiable on the short and medium term, although societal factors are more robust (5). Several studies have been conducted worldwide to identify and quantify the various risk factors for ARI and ALRI. Most of these studies focused more on ARI than on ALRI. Of those that studied ALRI, a large proportion defined outcome (ALRI) based on a combination of symptoms instead of clinical diagnosis, definitions with potentially higher sensitivity but lower specificity than those based on clinical diagnoses. This can increase the likelihood of both random and systematic misclassification and thus bias result of studies (6). Furthermore, even for fairly well established risk factors, only a few reported findings of a comparison of outcome for several level of each risk factors, for example, several levels of nutritional status (several, moderate, mild, normal) instead of a dichotomous level (severe with normal), and evaluation of a dose-response relationship (7). Studies on vitamin A supplementation, on the other hand, have given conflicting results on its effect on ARI and ALRI morbidity, in spite of showing protection against mortality (8,9). Very few studies have been reported that examined the relationship between dietary vitamin A and risk of mortality (10), morbidity in general, or ALRI in particular. The Magnitude of ALRI: Acute lower respiratory infections have been shown to be major causes of infant and childhood mortality in the developing countries (1) reported annual mortality rates from ARI to be 48-60 per 100,000 live births in children under five years of age in developed countries and 140 per 100,000 in developing countries. For infants under one year of age mortality from ARI was 1,000 per 100,000. They estimated that ARI mortality in Africa was 1,454.1 and 467 per 100,000 for children under-one and under-five years of age, respectively (2) calculated that 2.5 million infants and 1.5 million children aged 1-4 years die from ARI each year, approximately 98% of those deaths occurring in developing countries. It has now been shown that mortality from ARI is highest in Africa and Central America, followed by South America and Asia, with much lower rates in North America and Europe (11). Despite the large differential in ARI mortality between the developed and developing world, reported morbidity figures are fairly similar globally: 5-9 episodes per child per year. This has been ______________________________________ 1 From the Department of Community Health, Faculty of Medicine, P.O. Box 1176 Addis Ababa, Ethiopia (which were similar) and the patterns of mortality (which were different) indicated that a component 2 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── shown by early family studies in Cleveland (12), UK (13), Seattle (14), and Tecumseh (15,16). Studies from India (17,18), Bangladesh (19), Ethiopia (20) and Cost Rica (21) also showed similar morbidity figures. The discrepancy between the pattern of morbidity of ARI in developed and developing countries part of ARI, specifically ALRI occurrence may be higher in developing countries. Studies in several developing countries completed in 1980s showed this to be the case (3) after reviewing available data reported that the annual incidence of pneumonia ranged between 3 and 4 percent in under-five children in industrialized countries as compared to 10-20 percent in developing countries, and that mortality due to pneumonia is ten to fifty times higher in developing than developed countries. Eight major longitudinal studies on ARI conducted in Africa between 1972 and 1985 have also confirmed the discrepancy between ARI and ALRI incidence between the north and the south (22). Furthermore, ARI accounted for 25-66% of all episodes of illness, 17-41% of health facility attendances, and between 9-42% of hospital admissions. Similar figures have been reported for the whole of the developing world (23). The excess morbidity and mortality rates from ARI in the developing world indicated that several risk factors could be responsible. Several studies were thus undertaken to identify risk factors for ARI and subsequently a number of potential risk factors were identified. These included household characteristics such as indoor air pollution, crowding and parental education and child characteristics such as poor nutritional status, low birth weight, incomplete immunization, and being a male child under 2 years of age (7,24,3). Although a large body of data exists on the microbial etiology of ARI, as a result of several studies conducted particularly after the introduction of methods of virus identification in 1960s (25), the current consensus is that colonization of the respiratory tract by potential viral or bacterial pathogens, which is universal in developing country children (26), is not a sufficient cause for the development of ALRI (4). Control strategies for ALRI include case management of children with ARI, immunization (27) and reduction or modification of risk factors. Identification of modifiable risk factors is thus important although the effectiveness and feasibility of modification of already identified risk factors in the control of ARI remains to be elucidated (3). Risk factors of ALRI: Conceptual models describing societal, household and individual determinants of mortality and morbidity have been proposed (33,5). Societal risk factors, particularly socio-economic development, have had a major impact in the decrease of respiratory mortality in industrialized countries over the past one hundred years (34). Although socio-economic development, controlled population growth, reversal of environmental degradation, alleviation of poverty and ignorance and increase in the availability and accessibility of health services would most likely decrease mortality and morbidity from ARI, these societal determinants are less modifiable than intermediate variables (household characteristics) or proximate determinants (characteristics of children) at least in the medium term (5). With regards to identification and quantification of risk factors a number of unresolved issues remain. Most of the risk factor studies focused more on ARI than on ALRI. Of those which studied ALRI a large proportion defined outcome (ALRI) based on a combination of symptoms instead of clinical diagnosis: definitions with potentially higher sensitivity but lower specificity than those based on clinical diagnoses. Analytic epidemiologic studies evaluating putative risk factors need to be based on a case definition with the highest possible specificity. Otherwise the likelihood of both random and systematic misclassification can increase and thus bias result of studies (6). Several studies which have evaluated the specificity of definitions of ALRI based on simple symptomatology and respiratory counts have shown variable specificity, ranging between 65% in Kenya (28), to 93% in the Gambia (29) and with intermediate values being reported from India (30), Indonesia (31) and Lesotho (32). Furthermore, only a few studies reported findings for several levels of each risk factor, instead of for Risk factors for ALRI 3 ──────────────────────────────────────────────────────────── dichotomous levels, and evaluated dose-response relationships while adjusting for several potentially confounding variables (7). Studies on vitamin A supplementation, on the other hand, have given conflicting results regarding its effect on ARI and ALRI morbidity (discussed below), in spite of showing protection against mortality (8,9). Very few studies have been reported which examined the relationship between dietary vitamin A and risk of mortality (10), morbidity in general, or ALRI in particular. Thus the identification and quantification of risk factors for ALRI is still important. Household characteristics Maternal factors: Several studies have shown the association between maternal education and child survival (35) have reviewed the findings of these studies which mainly used data from national Demographic and Health surveys (DHS) carried out in Africa, Asia, and Latin America. The large majority of these surveys show very little association between levels of mother's education and the prevalence of cough or difficult breathing in the four weeks preceding the data collection (36). However, ARI-specific infant mortality rate was 14 per 1,000 live births in mothers with no schooling, 7 in those with 1-4 years of schooling, 4 in those with 5-8 years of schooling and 1 per 1,000 in those with over eight years of schooling in a large population cohort study of children in south Brazil (37). Hospital admissions due to pneumonia was also inversely and linearly associated with maternal education in the crude analysis. After adjustment for potential confounders only associations with birth weight and z-scores of weight for height, weight for age and height for age persisted. The impact of maternal education on child's height has also been reported from north-east Brazil (38). Mother's education was also inversely and linearly associated with ALRI mortality both in crude and adjusted analysis in a case-control study from south Brazil which enrolled 127 ALRI specific infant deaths as cases and 254 age and neighborhood matched live controls (39). In a Gambian case-control study, 129 children under-two years of age who were thought to have died from ALRI (by use of verbal autopsy method) were matched with one live and one dead control child, by age, sex, ethnic group and time and place of death (40). Maternal education was not associated with ALRI mortality both in the crude and adjusted analysis. No significant association between mothers' education and the incidence of ARI or ALRI was found in studies conducted in Columbia, Uruguay and Guatemala (26) or in urban Thailand (41). However, these studies reported only findings from a crude analysis. Thus, although the association of maternal education to child survival is well documented, its association to the incidence of ALRI is not well established. The independent effect of maternal employment and age on ALRI risk was examined in very few studies. In the crude analysis no consistent association between maternal age and incidence of ARI or ALRI was reported from studies in Columbia, Uruguay and Guatemala (26), but maternal income and employment outside of home was significantly associated with decreased ARI incidence in urban Thailand (41). Maternal education is strongly and linearly related to maternal income levels (42) and thus adjustment in analysis is important. In the south Brazil case-control study (39), mother's age was inversely and linearly related to ALRI mortality, both in the crude and adjusted analysis. Mother's employment outside of home was not significantly associated. In the Gambian case-control study (40) maternal age was not associated with ALRI mortality when cases were compared to matched dead controls but was positively associated with mortality when cases were compared to live controls. Thus the few well designed and analyzed studies which examined maternal age and employment did not give consistent results. Paternal factors: Very few studies have examined the independent role of father's education (independent of family income, maternal education etc.,) on ALRI occurrence. Crude analysis showed association with father's education with ARI incidence in Guatemala city (43) but not in urban Thailand (41). In both, adjusted analysis were not reported. In developing countries, father's education is closely linked to income of the head of the household, and thus income level of the household, 4 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── because maternal employment outside of home is fairly low. One study which adjusted for these variables showed an association between father's education and ALRI mortality (39). Household income level: Classic family studies conducted in developed countries have shown an association between ARI and low family income. (12,13,14,16). Household income level was inversely and linearly related in the Gambian case-control study when cases were matched to live controls, but not when matched with dead controls (40). Inverse and linear relationship was also demonstrated by the south Brazilian case-control study both in the crude and adjusted analysis (39). Crowding and family size: Crowding favors propagation of microbial agents of respiratory infections. In fact, colonization of the respiratory tract of children by potential pathogens is almost universal in developing countries (26). Increased incidence of ARI with crowding has also been reported in many studies in developed and developing countries, as reviewed by (7,3). A study from urban Guinea-Bissau indicated that crowding increased the severity of measles (for example, measles pneumonia) and case-fatality rate (44). However, studies of the relationship between ALRI and crowding that have adjusted for potential confounders, such as income, are very limited. The Gambian case-control study (40) showed a decreasing trend of ALRI mortality with increasing number of under-five children sharing a bedroom with a case, but an increased risk of ALRI with increasing number of people (over five years of age) sharing room with a case. A linear increase in the risk of ALRI mortality with increasing people in a child's bedroom and increasing number of under fives in a household was reported in adjusted analyses by the south Brazilian case-control study (39). Thus, crowding has been shown to be a risk of for ARI in several studies, but only a few have shown it be a determinant of ALRI occurrence. Environmental tobacco smoke (ETS): Large number of studies have examined the relationship between maternal and paternal smoking and the risk of ARI in children. They were reviewed by the 1986 Surgeon General Report on smoking and health (45), a report of the National Research Council (46,47,3). Studies have consistently shown an increase in the risk of ARI with ETS. More recently, studies from China showed a significant linear trend between parental smoking and occurrence of ALRI both in crude and adjusted analysis (48). The Gambian case-control study also showed a linear trend of risk for ALRI mortality with parental smoking but this was only limited to comparison of cases with live controls (40). Another report from the Gambia has also reported a strong linear association between the father's smoking behavior with difficulty in breathing (presumably ALRI) in children (49). The south Brazilian case-control study, on the other hand, (using an adjusted analysis) showed no increase in risk when either of the parents smoked, although a non-significant 30-40% increased risk was observed when both parents smoked (39). Indoor air pollution: In the developed world the major indoor air pollutants (other than ETS) are radon and radon decay products, asbestos fibre, and combustion products such as nitrogen oxide, carbon monoxide and sulphur dioxide (50). In developing countries, pollution of the indoor air from biomass fuel predominates. Particulate concentrations in cooking areas of African households ranged between 300 and 1,500 micrograms per cubic meter in lowland Kenya, 2,700-7,900 in highland Kenya, 1,000-2,500 in the Gambia, and 1,300 in Zimbabwe. This is very high compared with the maximum standard 24 hours limit set by the USA: 260 micrograms per cubic meter, and the one-hour standard set by Japan: 200 micrograms per cubic meter (51). A number of studies done in the developed world have implicated indoor air pollution as a risk factor for lower respiratory symptoms in children (52,53,54,55,56), while others have found no association (57,58,59). Although several studies from developing countries have shown associations of ALRI with indoor air pollution in the crude analysis very few have attempted to adjust for potential confounders (60,61,62,63,64,43). Campell et al (1989) have reported a significantly increased risk of ALRI in children who were carried on their mother's back and presumably exposed to higher indoor air pollution during cooking. An almost three-fold increase in risk was seen adjusting for several potential confounders. Another Risk factors for ALRI 5 ──────────────────────────────────────────────────────────── study, from the Gambia (40) did not show any consistent association between an index of indoor air pollution and ALRI mortality. Thus, although indoor air pollution has been regarded as a major occupational hazard to women in developing countries (65) and by implication a hazard to their children, the degree of risk to children has not been well quantified. Characteristics of children Protein-energy malnutrition (PEM): Many of the earlier population-based studies done in developing countries were unable to evaluate the relationship between PEM and ALRI because of their inadequate sample size. Thus, the 110 families in Vellore, India (71), the 159 families in Bangladesh, (19), 248 in Mexico, 292 in Ethiopia (20), were not able to generate sufficient number of ALRI cases for this purpose, although a study in Cost Rica did find a strong association between moderate/severe PEM and incidence of Pneumonia (21). A two-year ambulatory study in Cali, Columbia has shown PEM as a risk factor for pneumonia (23). A strong linear association between weight-for-age z-scores and ALRI was also demonstrated by a hospital-based study (66), and a community-based study in Manilla, Philippines (67), Uruguay, and Guatemala, (26). Case-control studies from both Gambia and south Brazil have reported a linear relationship between weight-for-age z-scores and ALRI mortality (40,39), as well as a hospital based study in Papua New Guinea (68). Weight-for-height and height-forage z-scores were associated with risk of ALRI in studies in Thailand (41), and ALRI mortality in south Brazil (39). Thus PEM has been consistently reported as a determinant of ALRI and ALRI mortality from studies conducted in several countries over the past two decades. This underlies the importance of considering this variable as a potential confounder in any evaluation of ALRI and potential risk factors. Vitamin A deficiency: The effect of vitamin A on tissue growth and differentiation and the consequences of its deficiency on epithelial tissue and the body's resistance to infection has been recognized for some time (69,70). The recognition of mild vitamin A deficiency as a predictor of childhood mortality was more recent (71), with the demonstration of xerophthalmia as a risk factor for ALRI independent of PEM (72). Subsequently, several trials were conducted in many countries to evaluate the effect of vitamin A supplementation on childhood mortality. Meta-analysis of these trials showed average reductions in mortality between 23% and 30% (8,9). On the other hand, the effects of vitamin A supplementation on morbidity particularly respiratory infections have not been consistent. Vitamin A supplementation did not influence the incidence, severity, or duration of respiratory infection in Tamil Nadu, India (73), Hyderabad, India (74), Indonesia (75), Nepal (76), and Ghana (77). A trial in Haiti reported an increased risk of respiratory signs of both ARI and ALRI after vitamin A supplementation (3). However, trials from north Thailand (78) and among Australian children (79) have reported reduced risk of ARI after vitamin A supplementation . In the vitamin A trial in the Sudan, dietary vitamin A intake was associated with reduced risk of cough with fever, but with an increased risk of cough alone (Fawzi et al 1995 unpublished data). Earlier reports from the trial had shown that dietary vitamin A intake was a strong predictor of xerophthalmia (8) and mortality (10). On the other hand, two community trials in Indonesia have shown an increased weight gain (76) and height gain (80) after vitamin A supplementation. Vitamin A may thus influence the occurrence of ALRI through its effect on PEM, since PEM has been shown to be a strong predictor of ALRI (see above). However, the quantification of vitamin A deficiency states and the risk of ALRI awaits further research. Breast feeding: The methodologic difficulties in studying breast feeding, which is a proxy to complex physical and social determinants of risk to ALRI, has been stated (81). More recently, (82), after reviewing twenty studies on breast feeding and infection in industrialized countries, concluded that only six studies met acceptable methodological standards. In a large national sample of US children under 1-2 years of age at the time of the survey in 1981, (83) has reported breast feeding as providing some protection for pneumonia after an adjusted analysis. 6 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Studies on breast feeding and infection, particularly diarrhoea, conducted in developing countries, have generally shown a protective role of breast feeding (82). Studies from Rwanda (83), and south Brazil (84) have shown protective role of breast feeding, against ALRI mortality. The Gambian casecontrol study (40) did not show protection of breast feeding against ALRI mortality. All three studies had a retrospective data collection design and were thus susceptible to the usual methodologic limitations of retrospective studies. Thus, although ALRI mortality was evaluated by few studies in developing countries, ALRI incidence was not adequately studied. Established determinants: Increasing age, female sex, birth weight over 2,500 grams, and immunization against measles, pertussis, S.pneumoniae, H.influenzae type B, C.diphteriae and influenza virus are individual factors that are known to be protective of ARI and ALRI (7,3). Although further research into these may not be recommended, data on these variables need to be included in ALRI risk factor studies to adjust for them in the analysis. ARI in Ethiopia: Earlier studies from Ethiopia have shown high rates of ARI with eight and four episodes of ARI in urban and rural children, respectively (20,85). ARI in the 1970s was probably the cause for a third to half of the infant mortality rate of 150-200 per 1,000 live births (86). Respiratory illnesses accounted for 10.6% of all admission to a pediatric ward (87). More recent studies have shown that in rural areas ARI was responsible for one-fifth of the under-five mortality and about onethird of the infant mortality (88). Prospective home surveillance studies in rural Ethiopia showed that ill children had 1.13 episodes of ARI (0.20-0.40 episodes of ALRI) in Butajira (89), 0.8 episodes per year in Dubluk, Borena and 0.6 episodes per year in Elka, Arssi (90). Microbiological studies have shown that colonization of the respiratory tract of children by potential pathogens is universal, 85% of children harbouring H. influenzae, 83% M. catarrhalis, and 90% S. pneumoniae in the naso-pharynx (91). Methods The study was a one-year follow-up of 1,992 children under-five years of age, randomly selected from the inner-city area of Addis Ababa, and was conducted between November 1991 and December 1992. Study area and population: The study area was Woreda (district) 3, one of the 25 city districts, and located at the center of Addis Ababa. Selection of this study area was based on logistic grounds and because it was not appreciably different from other districts of the city in terms of the population age and sex structure, ethnic and religious mix, and socio-economic development. At the onset of the study it was divided into 11 Kebeles (sub-districts) and had an estimated 14,318 households, a population of 71,591, and 8,590 under-five children (PHCC 1987). In November of 1991 we conducted a census of all eleven sub-districts to enumerate all children under-five living in the area. Using systematic sampling (every fourth household with an under-five child), we enrolled 2,025 households with one child under-five at the time of the census. In households where more than one child under-five lived, we enrolled the youngest child. Refusals to participate were very few (3%) and were mostly from well-to-do families. Of the 2,025 households initially enrolled, 33 families subsequently moved out of the city and were therefore excluded from the study. Data Collection: We recruited ten women with a high-school education living in the study subdistricts to interview members of households. They were given an intensive two-week training by the investigators before they started the interview. For the anthropometric measurements we obtained an experienced field worker from the Ethiopian Nutrition Institute. All data collection instruments were pilot-tested in a sub-district outside of the study area and the necessary modifications were made before they were used in the study. This sub-district was also used for field training of the field workers and supervisor. Household Characteristics: At baseline data on the following was collected: (1) socio- Risk factors for ALRI 7 ──────────────────────────────────────────────────────────── demographic characteristics of all members of households and (2) physical characteristics of homes, cooking area, and child's bedroom. Child Characteristics: Data on medical history of each child, including family history of respiratory ailments were also collected at baseline. We requested mothers to present the child's vaccination cards and for over 95% of children data on immunization status were collected from these cards. Breastfeeding information, including supplementary feeding practices, were collected at baseline and every month thereafter for children under one-year of age and every three months for older children. Weight and height/length were also measured at baseline and subsequently every month for children under one year and every three months for older children. Weight was measured to the nearest 100 g using a digital bathroom scale, standardized several times during the course of the study. For small children, both mother and child were weighed first, followed by the mother alone and the child weight was calculated by difference. Height was measured to the nearest 0.5 cm using a height stick with movable head piece against a flat surface. For small children, length was measured in a recumbent position with a length board. Dietary information was collected using food frequency questionnaires developed locally. An experienced dietitian from the Ethiopian Nutrition Institute was invited to participate in the process of identifying the relevant food items to be included in the FFQ, with the aim of measuring intakes of total calories and vitamin A in Addis Ababa. Food composition tables for use in Ethiopia, East Africa and Africa (Agren and Gibson 1968, ENI 1980, Gobezie 1970, West et al 1988, FAO 1968) were consulted to work out an initial extensive food list of over 400 items out of which 98 items deemed relevant and able to categorize children by past nutritional intake were selected. This FFQ was then pilot tested on 50 children under-five years of age in a sub-district outside of the study area before it was used in the cohort study. The FFQ was administered by trained and supervised interviewers. Mothers or other care takers were asked about their children's usual intake in the previous six months for the specific item and its portion size on the FFQ and responded in terms of frequency of intake per day, week, month, past 6 months or never. Validation sub-study: To assess the validity and reproducibility of the FFQ we selected a random sample of 100 children from the cohort study and collected multiple 24-hour diet recalls for seven days and afterwards venous blood for serum retinol determinations. This was conducted at the mid-interval of time between the administration the second and third FFQs. A diet recall form was developed for this purpose. Trained and supervised field workers made visits to selected households and interviewed caretakers on the child's diet intake during the previous 24-hours. This was repeated for seven consecutive days. A computer program was developed to calculate nutrient values from the FFQ using Ethiopian and African food composition table data. Daily, weekly or monthly frequencies for each item in the FFQ were first converted into daily frequencies of consumption. This was multiplied by the specific food composition data reflecting the nutrient content of one portion of each item in the questionnaire. The value was then summed up for all items in the FFQ giving total daily intake of the various nutrients for each child in the study. For the 24-hour multiple recalls the dietitian from the Ethiopian Nutrition Institute calculated the nutrient values manually but using the same step described above. Spearman correlation coefficients and cross-tabulation of quintiles from the FFQ and multiple 24-hour recalls and serum retinol values were used in the statistical analysis. Serum retinol determinations were conducted using high pressure liquid chromatography (HPLC) at the laboratory of the Ethiopian Nutrition Institute using the method described by Bieri et al (1979). Mothers were asked to bring their children to the clinical chemistry laboratory of a nearby referral and teaching hospital (Tikur Anbessa Hosptial) where an experienced laboratory technician drew their blood. Blood was collected by venous puncture without anticoagulant and serum was separated and stored in the dark at -200C until analysis. All-trans-retinol and all-trans-retinyl acetate, both in pure crystalline form, were from Sigma 8 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Chemical Company (St Louis, MO, USA). Methanol, absolute ethanol, and n-hexane were HPLC grade from Aldrich Chemical Company (Milwaukee, WI, USA) and were used without further purification as standards. The HPLC system was a Varian 5000 Liquid Chromatograph (Palo Alto, CA, USA) with 100-Variable UV-detector and a Varian 4270 integrator. Injector was a 7125 Rheodyne (Cotali, CA, USA) with a 50 microliter loop. The column was a 4 mm x 30 cm C 18 (10 micrometer particle size) Micropak. A 4 mm x 2 cm Serva (Heidelberg, Germany) guard column packed with a mixture of 95 parts methanol to 5 parts water at a flow rate of 2.5 ml/min. The column effluent was monitored at 280 nm. Sample preparation Before assay, serum samples frozen at -20oC were thawed and held at room temperature for 15 minutes under subdued light. Serum (100 microliter) was pipetted into 10 x 75 mm glass test tube. The internal standard of retinyl acetate solution in ethanol (50 microliter) is added and the contents mixed vigorously on a vortex mixer for 15 sec. For extraction of lipid, 100 microliter nhexane is added and the contents mixed vigorously intermittently for 45 seconds on a vortex mixer. The tubes are centrifuged for 1 minute at 1000 x g to separate the phases. A micropipette was used to remove the top (hexane) layer, which was transferred to a 5-ml conical centrifuge tube. The tubes were placed in a water bath at 60oC, and the solvent was evaporated with a stream of nitrogen. The residue in each tube was redissolved in 100 microliter methanol; 50 microliter of the solution was injected for chromatography. Quantitation Retinol and retinyl acetate standards were prepared in absolute ethanol. Concentrations of the standard solutions were determined using a Beckman Du-60 (Irvine, CA, USA) spectrophotometer. The retinol concentration was computed from a standard curve of peak area ratios. To prepare a standard curve, we combined a constant amount of the internal standard with five different concentrations of retinol. These mixtures of retinol and retinyl acetate were chromatographed, and the peak area ratios (peak area retinol and retinyl acetate) and concentration ratios (concentration of retinol: concentration of retinyl acetate) were determined. The inter-assay coefficient of variation for retinol determination was 5.2%. Measurement of outcome (ALRI): We defined the occurrence of ALRI based on a physiciandiagnosis of pneumonia, bronchiolitis or bronchitis using historical, physical and radiological evaluation. We instituted a surveillance and screening system as follows. At enrollment mothers were requested to take their children to a nearby hospital if they developed cough and fever and were also informed that the cost for the visit would be covered by the study. The mother's agreement to do this was a pre-requisite for enrolment of a child into the study. Interviewers visited study households every two weeks and completed a simple form about symptom histories of respiratory ailments and fever. Caretakers were asked about the occurrence and duration of those symptoms in the previous two weeks; this was done continuously for the one-year of follow-up. If during the time of interview a child had cough and fever, the mother was asked to take the child to a children's hospital nearby (Ethio-Swedish Pediatric Hospital). During their visit field workers also enquired about and recorded whether the child was taken to any other health care unit in the previous two weeks. If such was the case, that health unit was visited to obtain information on the clinical details of the consultation. At the pediatric teaching hospital a nurse initially screened presenting children for occurrence of respiratory symptoms, particularly for cough, fever or breathing difficulties and they were subsequently examined by physicians using standard clinical algorithms worked out before hand. ALRI-diagnosed children were given all the necessary treatment and follow-up by the clinicians. Statistical analysis: A proportional hazards model with time dependent covariates was fitted to the data for analysis. Anthropometric measurements, breast feeding status and dietary variables were included as time dependent covariates with other baseline characteristics. Children who were lost to follow up or who died were considered censored for the rest of the study period. For nutrient and foodgroup variables, cases reported in the first half of the follow up year were allocated according to the dietary intake assessed at baseline (FFQ1), whereas cases reported in the second half were Risk factors for ALRI 9 ──────────────────────────────────────────────────────────── allocated according to the mean dietary intake at baseline and mid-year (FFQ1 and FFQ2). For breast feeding and anthropometric measurements cases reported in any month were allocated according to the value assessed at the start of the month. A number of potentially confounding variables were included in the model. To evaluate the presence of an overall trend, adjusted relative risk estimates and test of significance were calculated using continuous independent variables in the multivariate model. A probability level of 0.05 was taken as a cut-off for statistical significance. Data were entered on to a computer using the EPI-INFO program, version 5, CDC, Atlanta GA, and analyzed using the Statistical Analysis System program, version 6.04, SAS Institute, Cary NC. Scientific and ethical clearance for the study was given by the Research and Publication Committees of the Department of Community Health, the Faculty of Medicine, and the Research and Publication Office of Addis Ababa University. References 1. Bulla A and Hitze KL, Acute respiratory infections: a review Bull. WHO 1978;56(3):481-498. 2. Leowsky J. Mortality from acute respiratory infections in children under 5 years of age global estimates. World Health Stat. Q. 1986;39:138-44. 3. Stansfield SK and Shepard DS Acute respiratory infection. In: Jamison DT, Mosley WH, Measham AR and Bobadilla JL eds, Disease control priorities in developing countries. New York: Oxford university Press 1993:67-90. 4. IUATLD Working Group on ARI Acute respiratory infections: conclusions of an IUATLD workshop. Tubercle and Lung Disease. 1993;74:2-5. 5. Feachem RG, Graham WJ and Timaens I. Identifying health problems and health research priorities in developing countries. London School of Hygiene and Tropical Medicine, September 1987. 6. Rothman KJ. Modern epidemiology. Boston: Little, Brown and Company 1986. 7. Graham NM. The epidemiology of acute respiratory infections in children and adults: a global perspective. Epidemiol. Rev. 1990;12:149-78. 8. Fawzi WW, Chalmers TC, Herrera MG and Mosteller F. Vitamin A supplementation and child mortality: a meta analysis. JAMA 1993;269:898-903. 9. Gelaziou PP and Mackerras DEM. Vitamin A supplementation and child mortality: a meta-analysis Br. Med. J. 1993;306:366-70. 10. Fawzi WW, Herrera MG, Willett WW, Nestel P. Amin AE, Lipsity S and Mohamed KA. Dietary vitamin A intake and the risk of mortality among children Am. J. Clin. Nutr. 1994;59:401-8. 11. IUATLD Working Group on ARI Acute respiratory infections: a high priority. Tubercle and Lung Disease. 1993;74:1. 12. Dingle JH, Badger GF, Feller AE, Hodges RG, Jordan WS, and Rammelkamp Jr. CH. A study of Illness in a Group of Cleveland Families I plan of study and certain General Observations. Am. J. Hyg. 1953;58:16-30. 13. Brimblecombe FSW, Cruickshank R. Masters PL, Reid DD and Stewart GT, Family studies of respiratory infections. Br. Med. J. 1958;1:119-28. 14. Fox JP, Hall CE, Cooney MK, Luce RE and Kronmal RA. The Seattle Virus Watch: II Objectives, study population and its observation, data processing and summary of illnesses. Am. J. Epidemiol. 1972;96:270-285. 15. Monto AS, Napier JA and Metzner HI. The tecumseh study of respiratory illness: I plan of the study and observations on plan of the study and observations on syndromes of acute respiratory disease. Am. J. Epidemiol. 1971;94:269-279. 16. Monto AS and Ullman BM. Acute respiratory illness in an American community: The Tecumseh study. JAMA 1974;227(2):164-69. 10 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── 17. Feldman RA, Kamath KR, Sundar Rao PSS, and Webb JKG. Infection and disease in a group of south Indian families: I Introduction, methods, definitions and general observations in a continuing study. Am. J. Epidemiol 1969;89:364-374. 18. Kamath KR, Feldman RA, Sundar Rao PSS and Webb JKG. Infection and Diseases in a Group of South Indian Families. II General Morbidity patterns in Families and Family Members. Am. J. Epidemiol. 1969;89:375-83. 19. Black RE, Brown KH, Becker S. and Yunus M. Longitudinal studies of infectious diseases and physical growth of children in rural Bangladesh. I patterns of Morbidity. Am. J. Epidemiol. 1982;115:305-14. 20. Freij L and Wall S. Exploring child health and its ecology: The Kirkos Study in Addis Ababa. Acta. Pediatr. Scand. Suppl. 267 (1977). 21. James JW. Longitudinal Study of the morbidity of diarrheal and respiratory infections in malnourished children. Am. J. Clin. Nutr. 1972;25:690-94. 22. Kirkwood BR Acute respiratory infections. In: Feachem RG and Jamison DT eds, Disease and mortality in sub-Saharan Africa. New York:Oxford University Press 1991:158-72 23. Berman S. Duenas A. Bedoya A. Constain V. Leon S. Borrero I and Murphy J. Acute lower respiratory tract illnesses in Cali, Columbia: A two- year ambulatory study Paediatrics. 1983;71:210218. 24. Garenne M, Ronsmans C and Campbell H. The magnitude of mortality from acute respiratory infections in children under 5 years in developing countries. World Health Stat Q. 1992;45(2-3):18091. 25. Monto AS. Acute Respiratory Infections in children of developing countries: challenge of the 1990s Rev. Infect. Dis. 1989;11(3):498-505. 26. Selwyn BJ, et. al. The epidemiology of acute respiratory tract infection in young children: Comparison of findings from several developing countries. Rev. Infect. Dis. 1990;12:5870-5888. 27. WHO, A Programme for Controlling Acute Respiratory Infections in Children: Memorandum from a WHO Meeting. Bull. WHO 1984:62(1):47-58. 28. Wafula et al 1984 (Kenya /?/) 29. Campbell H. Byass P. Lamont AC, Forqie IM, O'Neill KP, Lloyd-Evans N. Greenwood BM. Assessment of clinical criteria for identification of severe acute lower respiratory tract infections in children. Lancet 1989 Feb. 11;1(8633):297-9. 30. Cherian T. et al. Evaluation of simple clinical signs for the diagnosis of acute lower respiratory infections. Lancet 1988;ii:125-8. 31. Mulholland EK, Simoes EA, Costales MO, McGratt EJ, Manalac EM and Gove S. Standardized diagnosis of pneumonia in developing countries. Pediatr. Infect. Dis. J. 1992 Feb;11(2);77-81. 32. Redd SC, Vreuls R, Metsing M, Mohobane PH, Patrick E. and Moteetee M. Clinical signs of pneumonia in children attending a hospital outpatient department in Lesotho. Bull. WHO. 1994;72(1):113-18. 33. Mosley WH and Chen LC. An analytical framework for the study of child survival in developing countries. Pop. Dev. Rev. 1984; 10(suppl):25-45. 34. Douglas RM, Acute respiratory infections in children in the developing world Semin. Respir. Infect. 1991 Dec; 6(4):217-24. 35. Cleland JG, and van Ginneken JK, Maternal education and child survival in developing countries: the search for pattern of influence. Soc. Sci. Med. 1988;27:1357. 36. Hobcraft JN. Women's education, child welfare and child survival: A review of the evidence. Health Transitions Review 1993; 3 (2):159-75. 37. Victoria CG, Huttly SR, Barros FC, Lombardi C, Vaughan JP. Maternal Education in Relation to Early and Late Child Health Outcomes: Findings from a Brazilian Cohort Study. Soc. Sci Med. 1992 Apr; 34(8):899-905. 38. Thomas D, Strauss J and Henriques MH, How does mother's education affect child height ? Risk factors for ALRI 11 ──────────────────────────────────────────────────────────── Journal of Human Resources 1990;26(2):183-211. 39. Victora CG, Smith PG, Barros FC, et al. Risk factors for death due to respiratory infections among Brazilian infants. Int. J. Epidemiol. 1989; 18:918-25. 40. Francisco ADE, Morris J, Hall AJ, Armstrong Schellenberg JRM and Greenwood BM. Risk factors for mortality from acute lower respiratory tract infections in young Gambian Children. Int. J. Epidemiology 1993;22:1174-82. 41. Vathanophas K. Sangchai R. Suwanee R. Pariyanonda A. Thangsuvan J. Banyaratabhandu P. Athipanyankom S. Subharee S. Jayanetra P. Wasi C. Vorachit M. and Putnarathana P. A Communitybased study of acute respiratory infection in Thai children. Rev. Infect. Dis. 1990;12:(5) 957-965. 42. Barros FC, Victoria CG, and Vaughan JP, The Pelotas birth cohort study, 1982-87. Strategies for following up 6000 children in a developing country. Pediatr. Perinat. Epidemiol. 1990;4:205-20. 43. Cruz JR, Pareja G. de Fernandez A. Peralta F. Caceres P. and Cano F. Epidemiology of acute respiratory tract infections among Guatemalan ambulatory preschool children. Rev. Infect. Dis. 1990;12:S1029-1034. 44. Aaby P. Malnutrition and over crowding/intensive exposure in severe measles infection: review of community studies. Rev. Infect. Dis. 1988;10:478-91. 45. USDHHS 1986 ETS 46. National Research council 1986. ETS 47. Samet et al ETS 1991 48. Jim C and Rossignol AM. Effects of passive smoking on respiratory illness from birth to age eighteen months, in Shangai, People's Republic of China. J. Paediatr. 1993; 123(4):553-8. 49. Campbell H, Armstron JRM and Byass P. Indoor air pollution in developing countries and acute respiratory infection in children [letter]. Lancet 1989;1:1012. 50. Spengler JD and Sexton K. Indoor air pollution: A public health perspective. Science 1983;221(4605):9-17. 51. Smith & Liw 1994 indoor air. 52. Melia RJW, Florey CduV, Altman DG and Swan AV. Association between gas cooking and respiratory disease in children. Br. Med. J 1977;2:149-152. 53. Melia RJW, Florey CduV and Chinn S. The relation between respiratory illness in primary school children and the use of gas for cooking. I result from a national survey. Int. J. Epidemiol. 1979;8:333338. 54. Honicky RE, Osborne JS and Akpom CA. Symptoms of respiratory illness in young children and the use of wood-burning stoves for indoor heating. Paediatrics 1985;75:587-93. 55. Berkey CS, Ware JH, Dockery DW, Ferris BG, and speizer FE. Indoor Air pollution and pulmonary function growth in preadolescent children. Am. J. Epidemiol. 1986;123:250-60. 57. /?/ 57. Schilling RSF, Letai AD, HUI SL, Beck GJ, Schoenberg JB and Bouhuys. Lung function, respiratory disease and smoking in families. Am. J. Epidemiol. 1977;106:274-283. 58. Keller MD, Lanese RR, Mitchell RI and Cote RW. Respiratory illness in households using gas and electricity for cooking I Survey of incidence. Environ. Res. 1979;19:495-503. 59. Hosein HR and Bouhuys A. Possible Environmental Hazards of Gas Cooking Br. Med. J. 1979;1:125 60.Kossove D. Smoked-filled Rroms and lower respiratory disease in infants. S. Afr. Med. J. 1982;61:622-24. 61. Sofoluwe GO. Smoke pollution in dwellings of infants with bronchopneumonia. Arch Environ Health 1968;16:670-2. 62. Sofoluwe GO. The effect of housing conditions on prevalence of bronchitis- bronchiolitis and bronchopneumonia in Lagos, Nigeria. West Afr. Med. J. 1969;35-42. 12 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── 63. Anderson HR, Respiratory Abnormalities in Papua New Guinea Children : The effects of locality and Domestic wood smoke pollution. Intl. J. Epidemiol 1978;7:63-72. 64. Pandey MR, Bolei JSM, Smith KR and Wafala EM. Indoor air pollution in developing countries and acute respiratory infections in Children. Lancet 1989;1:427-8. 65. Dekoning HW, Smith KR, and Last JM, Biomass Fuel Combustion and Health. Bull. WHO 1985;63(1):11-26. 66. Tupasi TE, Velmonte MA, Sanvictores MEG. Determinants of morbidity and mortality due to acute respiratory infections: Implications for Infection. J. Infect Dis. 1988;157:615-23. 67. Tupasi TE, Mangubat NV, Sunico MES, Magdangal DM, Navarro EE, Leonor ZA, Lupisan S, Medalla F and Lucero MG. Malnutrition and acute respiratory tract infections in Filipino children. Rev. Infect. Dis. 1990;12: S1047-1054. 68. Spooner V, Barker J, Tulloch S, Lehmann D, Marshall TF, Kajoi M and Alpers MP. Clinical signs and risk factors associated with pneumonia in children admitted T. Goroka Hospital, Papua New Guinea. J. Trop. Pediatr. Dec. 1989;35(6);295-300. 69. /?/ 70. LeRiche H, Kinnear AA and Smit RJ. The Diepkroof nutrition and health study on Bantu Boys, South Africa. Canad. Med. Ass. J. 1956;74:130-138. 71. Sommer A, Tarwotjo I, Hussaini G and Susanto D. Increase mortality in children with mild vitamin A deficiency. Lancet 1983;11:585-88. 72. Sommer A, Katz J and Tarwotjo I. Increased risk of respiratory disease and diarrhoea in children with preexisting mild vitamin A deficiency. Am. J. Clin. Nutr 1984;40:1090-1095. 73. Rahmathullah L, Underwood BA, Thulasira ED and Milton RC. Diarrhoea, respiratory infections, and growth are not affected by the weekly low-dose vitamin A supplement: A masked, controlled field trial in children in Southern India. Am. J. Clin. Nutr. 1991;54:568-77. 74. Vijayaraghavan K. Radhaiah G. Prakasam B. Sarma KVR, Reddy V, Effect of massive dose of vitamin A on morbidity and mortality in indian children. Lancet 1990;336:1342-1345. 75. Abdeljaber MH, Monto AS, Tilden RL, Schork A. Tarwotjo I. The impact of vitamin A supplementation on morbidity: A randomized community intervention trial. Am. J. Public Health 1991;81:1654-1656. 76. West KP, Djundaedi E, Paudji A et. al. Vitamin A Supplementation and Growth: A Randomized Community Trial. Am. J. Nutr. 1988;48: 157-64. 77. Ghana VAST study Team. Vitamin A supplementation in northern Ghana; effects on clinic attendances, hospital admissions, and child mortality. Lancet 1993;342:7-12. 78. Bloem MW, Wedel M. Egger RJ, et al. Mild vitamin A deficiency and risk of respiratory tract diseases and diarrhoea in pre school and school children in north eastern Thailand. Am. J. Epidemiol. 1990;131:332-9. 79. Pinnock CB, Douglas RM and Badcock NR. Vitamins A status in children who are prone to respiratory tract infections. Aust. Paediatr. J. 1986;22:95-99. 80. Muhilal PD, Idjradinata YR and Muherdiyantiningsih KD. Vitamins A- fortified monosodium glutamate and health, growth and survival of children: a controlled field trial. Am. J. Clin. Nutr. 1988:48:1271-76. 81. Sauls HS. Potential effect of demographic and other variables in studies comparing morbidity of breast-fed and bottle-fed. Infants. Pediatrics 1979;64:523-527. 82. Bauchner H. Leventhal JR, Shapiro E. Studies of breast feeding and infection:how good is the evidence? J.A.M.A. 1986;256:887-92. 83. Ford K and Labbok M. Breast feeding and child health in the United States. J. Biosoc. Sci 1993;25(2):187-94. 84. Victora CG, Barros FC, Vaughan JP and Reixeira AMB. Birthweight and infant mortality: a longitudinal study of 5914 Brazilian children. Int. J. Epidemiol. 1987;16:239-245. Risk factors for ALRI 13 ──────────────────────────────────────────────────────────── 85. Dodg 1970 Ethiopia. 86. Shamebo D. Fertility and infant mortality in Dembia plain, Gondar. Ethiop. Med. J. 1978;16:9597. 87. Tafesse B. Analysis of admissions of the Ethio-Swedish paediatric clinic (1970-71). Ethiop. Med. J. 1973;11:3-12. 88. Shamebo D. Epidemiology for public health research and action in a developing society: The Butajira Rural Health Project in Ethiopia. [Dissertation]. Umea, Sweden: Umeå University, 1993. 89. Muhe L. Child health and acute respiratory infections in Ethiopia: Epidemiology for prevention and control. [Dissertation]. Umea, Sweden: Umea University, 1994. 90. Lindtjorn B, Alemu T and Bjorvatn B. Population growth, fertility, mortality and migration in drought prone areas in Ethiopia. Trans. Roy. Soc. Trop. Med. Hyg. 1993;87:24-28. 91. Ringty et al 1993. Original article Socio-demographic characteristics and indoor air pollution as risk factors for acute lower respiratory infections in under-five children in Addis Ababa, Ethiopia Derege Kebede1 and Wal1ett C Willett2 Abstract: This paper reports on the findings of a one-year cohort study of 1,992 children under five years of age conducted in Addis Ababa, Ethiopia, between November, 1991 and December, 1992. The aim of the study was to quantify the relationship between household characteristics such as parental education, household income and crowding, and indoor air pollution from cooking or tobacco and risk of ALRI (physician diagnosed). There were 97 incident cases with the cumulative incidence of ALRI being 48.7 per thousand for 12 months of follow-up. Although ALRI risk was lower among children from homes with an employed head of household (Adjusted relative risk, RR: 0.56 and 95% confidence intervals, CI: 0.34, 0.93), other parental factors, such as mother's or father's education, occupation or income, were not associated with development of ALRI in children. There were increased rates of ALRI with use biomass fuel for cooking, and when the child's bedroom was not separate from the kitchen, was used for cooking and had no functional window, although none of these associations achieved statistical significance. Compared with the lowest level of estimated indoor air pollution, medium level of level of indoor air pollution level was significantly associated with ALRI risk (Adjusted RR: 2.66 and 95% CI: 1.33, 5.32), but risk did not increase further with higher levels of the pollution index. Our results suggest that indoor air pollution is a risk factor for ALRI occurrence and that this excess risk is independent of other familial or individual risk factors for ALRI in children. [Ethiop. J. Health Dev. 1997;0(0):15-25] Introduction Acute lower respiratory infections are a major cause of infant and childhood mortality in developing countries (1-3). Earlier studies from Ethiopia have shown high rates of ARI, with eight and four episodes of ARI in urban and rural children, respectively (4,5). ARI in the 1970s was probably the cause for a third to half of the infant mortality rate of 150-200 per 1,000 live births (6). Respiratory illnesses accounted for 10.6% of all admissions to a pediatric ward (7). More recent studies have shown that in rural areas ARI was responsible for one-fifth of the under-five mortality and about onethird of the infant mortality (8). Prospective home surveillance studies in rural Ethiopia showed that children had 1.13 episodes of ARI (0.20-0.40 episodes of ALRI) per year in Butajira (9), 0.8 episodes per year in Dubluk, Borena and 0.6 episodes per year in Elka, Arssi (10). Despite the large differential in ARI mortality between the developed and developing world, reported morbidity figures are fairly similar globally: 5-9 episodes per child per year. This has been shown in early family studies in Cleveland (11), UK (12), Seattle (13), and Tecumseh (14,15). Studies from India (16, 17), Bangladesh (18), Ethiopia (4) and Cost Rica (19) also showed similar morbidity ______________________________________ 1 From the Department of Community Health, Faculty of Medicine, P.O. Box 1176 Addis Ababa, Ethiopia and 2Departments of Nutritional and Epidemiology, Harvard School Public Health, 665 Huntington avenue, Boston, 02115, USA figures. The excess morbidity and mortality rates from ARI in the developing world indicated that several risk factors could be responsible. Several studies were thus undertaken to identify risk factors for ARI and subsequently a number of potential risk factors were identified. These were reviewed elsewhere (20-22). With regards to identification and quantification of risk factors, a number of unresolved issues remain. Most of the risk factor studies focused more on ARI rather than on ALRI. Of those that studied ALRI, a large proportion defined outcome (ALRI) based on a combination of symptoms instead of 15 ──────────────────────────────────────────────────────────── clinical diagnosis, definitions with potentially higher sensitivity but lower specificity than those based on clinical diagnoses. Ideally, analytic epidemiologic studies evaluating putative risk factors should be based on a case definition with the highest possible specificity to minimize the likelihood of both random and systematic misclassification, which can bias the results of studies (23). Several studies that have evaluated the validity of definitions of ALRI based on simple symptomatology and respiratory counts have shown variable specificity, ranging between 65% in Kenya (24), to 93% in the Gambia (25) and with intermediate values being reported from India (26), Indonesia (27) and Lesotho (28). Furthermore, only a few studies reported findings of a comparison of outcome for several levels of each risk factors instead of for dichotomous levels and evaluate for dose-response relationships at the same time adjusting for potentially confounding variables (20). A number of studies done in the developed world have implicated indoor air pollution as a risk factor for lower respiratory symptoms in children (29-35), while others have found no association (3638). Although several studies from developing countries have shown associations of ALRI with indoor air pollution in the crude analysis very few have attempted to adjust for potential confounders (39-44). This paper reports on the findings of a one-year cohort study of 1,992 children under five years of age conducted in Addis Ababa Ethiopia, between November 1991 and December 1992. The aim of the study was to quantify the relationship between household characteristics such as parental education, household income and crowding, and indoor air pollution from cooking or tobacco and risk of ALRI (physician diagnosed). Methods The study was a one-year follow-up of 1,992 children under-five years of age, randomly selected from the inner-city area of Addis Ababa, and was conducted between November 1991 and December 1992. Study area and population: The study area was Woreda (district) 3, one of the 25 city districts, and located at the center of Addis Ababa. Selection of this study area was based on logistic grounds and because it was not appreciably different from other districts of the city in terms of the population age and sex structure, ethnic and religious mix, and socio-economic development. At the onset of the study it was divided into 11 Kebeles (sub-districts) and had an estimated 14,318 households, a population of 71,591, and 8,590 children under five years of age a. In November of 1991 we conducted a census of all eleven sub-districts to enumerate all children under-five living in the area. Using systematic sampling (every fourth household with an under-five child), we enrolled 2,025 households with one child under-five at the time of the census. In households where more than one child under-five lived, we enrolled the youngest child. Refusals to participate were very few (3%) and were mostly from well-to-do families. Of the 2,025 households initially enrolled, 33 families subsequently moved out of the city and were therefore excluded from the study. All subjects were enrolled at the same time and followed for one year. _______________________________________ a Population & Housing Census Commission. Population and Housing Census of Ethiopia, 1984: Analytical report on results for Addis Ababa. Addis Ababa, January 1987:1(1). Data Collection: We recruited ten women with a high-school education living in the study subdistricts to interview members of households. They were given an intensive two-week training by the investigators before they started the interview. For the anthropometric measurements we obtained an experienced field worker from the Ethiopian Nutrition Institute. All data collection instruments were pilot-tested in a sub-district outside of the study area and the necessary modifications were made before they were used in the study. This sub-district was also used for field training of the field workers and supervisor. Household Characteristics: At baseline data on the following was collected: (1) socio- 16 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── demographic characteristics of all members of households and (2) physical characteristics of homes, cooking area, and child's bedroom. We categorized study children into four levels of indoor air pollution by calculating a composite score based on level of smoke clearance, separation of kitchen and the child's bedroom, absence of cooking in child's bedroom, and the presence of functional windows. The referent category represented the absence of all of the above conditions, the second level the presence of any one or two, the third any three, and the fourth level represented the combination of all of the four conditions. Child Characteristics: Data on medical history of each child, including family history of respiratory ailments were also collected at baseline. We requested mothers to present the child's vaccination cards and for over 95% of children data on immunization status were collected from these cards. Breastfeeding information, including supplementary feeding practices, were collected at baseline and every month thereafter for children under one-year of age and every three months for older children. Weight and height/length were also measured at baseline and subsequently every month for children under one year and every three months for older children. Weight was measured to the nearest 100 g using a digital bathroom scale, standardized several times during the course of the study. For small children, both mother and child were weighed first, followed by the mother alone and the child weight was calculated by difference. Height was measured to the nearest 0.5 cm using a height stick with movable head piece against a flat surface. For small children, length was measured in a recumbent position with a length board. Measurement of outcome (ALRI): We defined the occurrence of ALRI based on a physiciandiagnosis of pneumonia, bronchiolitis or bronchitis using historical, physical and radiological evaluation. We instituted a surveillance and screening system as follows. At enrollment mothers were requested to take their children to a nearby hospital if they developed cough and fever and were also informed that the cost for the visit would be covered by the study. The mother's agreement to do this was a pre-requisite for enrolment of a child into the study. Interviewers visited study households every two weeks and completed a simple form about symptom histories of respiratory ailments and fever. Caretakers were asked about the occurrence and duration of those symptoms in the previous two weeks; this was done continuously for the one-year of follow-up. If during the time of interview a child had cough and fever, the mother was asked to take the child to a children's hospital nearby (Ethio-Swedish Pediatric Hospital). During their visit field workers also enquired about and recorded whether the child was taken to any other health care unit in the previous two weeks. If such was the case, that health unit was visited to obtain information on the clinical details of the consultation. At the pediatric teaching hospital a nurse initially screened presenting children for occurrence of respiratory symptoms, particularly for cough, fever or breathing difficulties and they were subsequently examined by physicians using standard clinical algorithms worked out before hand. ALRI-diagnosed children were given all the necessary treatment and follow-up by the clinicians. 17 ──────────────────────────────────────────────────────────── Table 1: Relative risks of ALRI according to characteristics of children, Addis Ababa, 1993. Characteristic Population (%) ALRI cases(%) Adjusted RR (95 CI)a P(trend)b Sex Male 1,057 (53.1) 55 (5.2) 1.00 Female 935 (46.9) 42 (4.5) 0.88 (0.57, 1.32) Age Under 6 months 110 (5.5) 10 (9.1) 2.03 (0.96, 4.31) 0.01 6-12 months 180 (9.0) 20 (11.1) 2.88 (1.57, 5.28) Over 12 months 378 (19.0) 30 (7.9) 2.46 (1.48, 4.10) Over 24 months ,324 (66.5) 37 (2.8) 1.00 Vaccinated for measles No 378 (19.0) 26 (6.9) 1.00 Yes 1,614 (81.0) 71 (4.4) 0.90 (0.54, 1.50) Place of delivery Home 1,028 (51.6) 75 (7.3) 1.00 Health facility 964 (48.4) 22 (2.2) 0.42 (0.25, 0.68) Total 1,992 (100.0) 97 (4.9) a Terms included in the multivariate model (in addition to those shown in the table): weight-for-height z scores (3 levels), dietary vitamin A intake (5 levels), household income (3 levels), ethnicity (4 levels), crowding (4 levels) and indoor air pollution (4 levels). b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. Statistical analysis: A proportional hazards model with time dependent covariates was fitted to the data for analysis. Anthropometric measurements and dietary variables were included as time dependent covariates with other baseline characteristics. Children who died were considered censored for the rest of the study period. There was no loss to follow up. For nutrient and foodgroup variables, cases reported in the first half of the follow up year were allocated according to the dietary intake assessed at baseline (FFQ1), whereas cases reported in the second half were allocated according to the mean dietary intake at baseline and mid-year (FFQ1 and FFQ2). For breast feeding and anthropometric measurements cases reported in any month were allocated according to the value assessed at the start of the month. A number of potentially confounding variables were included in the model. To evaluate the presence of an overall trend, adjusted relative risk estimates and test of significance were calculated using continuous independent variables in the multivariate model. A probability level of 0.05 was taken as a cut-off for statistical significance. Data were entered onto a computer using the EPI-INFO program, version 5, CDC, Atlanta GA, and analyzed using the Statistical Analysis System program, version 6.04, SAS Institute, Cary NC. The free and informed consent of the parents of the study children was obtained before data collection. Scientific and ethical clearance for the study was given by the Research and Publication Committees of the Department of Community Health, the Faculty of Medicine, and the Research and Publication Office of Addis Ababa University. Results Of the total of 1,992 children under five years of age followed for one year, 53.1% were males, and at baseline 5.5% were under six months of age and 14.5% were infants under one year of age. About half of the children were born at a health facility and 19.0% were yet to be immunized (Table 1). Approximately 90% of children were from low-income families earning below 60 US Dollars per month (Table 2). Over 85% of the children were from Christian families and 39% from the Amhara ethnic group. There were 97 incident cases with the cumulative incidence of ALRI being 48.7 per thousand for 12 months of follow-up. There were 14 deaths during the follow up time. Of these two were associated with ALRI, six with diarrheal diseases, four with ARI symptoms, one with electrocution, and one with kidney disease. Of the ALRI cases, 63 were diagnosed 18 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Table 2: Relative risks of ALRI according to household characteristics, Addis Ababa, 1993. Characteristics Head of the household: Not literate Elementary Secondary Not employed Employed Muslim Christian Amhara Oromo Tigrai Others Total household income(monthly) Population (%) ALRI cases(%) 319 (16.0) 1,131 (56.8) 542 (27.2) 1,098 (58.7) 824 (41.3) 269 (13.5) 1,723 (86.5) 784 (39.3) 308 (15.4) 344 (17.2) 556 (27.9) 15 (4.7) 50 (4.4) 32 (5.9) 70 (5.9) 27 (3.2) 20 (7.4) 77 (4.4) 36 (4.5) 13 (4.2) 18 (5.2) 30 (5.4) Adjusted RR(95% CI)a 1.00 0.78 (0.43, 1.42) 0.91 (0.46, 1.81) 1.00 0.56 (0.34, 0.93) 1.00 0.62 (0.34, 1.13) 1.00 0.79 (0.40, 1.56) 0.88 (0.49, 1.60) 0.81 (0.45, 1.44) P for trendb 0.9 300 Birrc & above 217 (10.9) 8 (3.6) 1.00 0.2 101-299 Birr 343 (17.2) 20 (5.8) 0.95 (0.55, 1.62) < 100 Birr 1,432 (71.9) 69 (4.8) 0.49 (0.21, 1.14) Total 1,992 (100.0) 97 (4.9) 1.00 a Terms included in the multivariate model (in addition to those shown in the table): sex, age (4 levels), weight-for-height z scores (3 levels), dietary vitamin A intake (5 levels), birth place (2 levels), crowding (4 levels) and cigarette smoking (3 levels) and indoor air pollution (4 levels). b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. c 1 Birr = 0.20 US Dollars as bronchopneumonia, 12 as broncho-pneumonia with rickets and marasmus, eight as bronchopneumonia with otitis media, four as lobar pneumonia, and 10 as bronchiolitis. Both age and delivery in a health service were strong predictors of ALRI risk. The risk of ALRI declined with increasing age. The test for trend for this increase was statistically significant (P=0.01). The risk of ALRI was two-fold higher in children under six months of age when compared to those over 24 months of age (Adjusted relative risk, RR: 2.03 and 95% confidence intervals, CI: 0.96, 4.31). For children delivered at a hospital, health center or clinic the risk of ALRI was lower (Adjusted RR: 0.42 and 95% CI: 0.25, 0.68). Female sex and measles vaccination were associated with decreased risk of ALRI but these did not achieve statistical significance. Most of the children not vaccinated for measles were not yet nine months old, the usual age of immunization. The risk of ALRI was four-fold in children with weight-for-height z-scores less than -3.0 SD when compared to children above -2.0 SD (data not shown). ALRI risk was reduced with employment of the head of the household (Adjusted RR: 0.56 and 95% CI: 0.34, 0.93). Other characteristics of the head of the household such as educational level, ethnic and religious affiliations were not significantly associated with ALRI occurrence (Table 2). Household income level was also not associated with ALRI. ALRI risk was higher in unemployed mothers as well as in those under 20 years of age. However, these associations did not achieve statstical significance (Table 3). The predominant sources of biomass fuel in the households were wood, dried leaves, charcoal and dung. There were reductions in risk of ALRI associated with use of non-biomass fuel for cooking (Table 4), and when the child's bedroom was separate from the kitchen, was not used for cooking and had functional window. However, none of these associations achieved statistical significance. Indoor air pollution level was, assessed as a composite score of the four household characterstics noted above, was significantly associated with ALRI risk (Table 5). This effect of indoor air pollution remained after adjustment for sex, age, crowding, smoking, household income level, birthplace, dietary vitamin A intake and weight-for-height status. Risk of ALRI increased with increasing level of pollution, but this was not linear. The relative risk of ALRI among children with 19 ──────────────────────────────────────────────────────────── Table 3: Relative risks of ALRI according to parental socio-demographic characteristics, Addis Ababa, 1993. Characteristics Population (%) ALRI cases(%) Adjusted RR(95% CI)a Mother: Not literate Elementary Secondary No mother 427 (21.4) 907 (45.5) 336 (16.8) 322 (16.2) 18 (4.2) 48 (5.2) 16 (4.7) 15 (4.6) 1.00 1.21 (0.53, 2.76) 1.05 (0.57, 1.93) 0.6 Under 20 20-29 30-39 Over 40 No mother 489 (24.5) 772 (38.8) 220 (11.0) 189 (9.5) 322 (16.2) 28 (5.7) 34 (4.4) 10 (4.5) 12 (6.3) 15 (4.6) 1.00 0.62 (0.25, 1.48) 0.75 (0.33, 1.70) 0.79 (0.32, 1.94) 0.1 1,450 (72.8) 220 (11.0) 322 (16.2) 76 (5.2) 6 (2.7) 15 (4.6) 1.00 0.43 (0.18, 1.01) 159 (7.9) 755 (37.9) 528 (26.5) 550 (27.6) 1,992 (100.0) 6 (3.7) 38 (5.0) 32 (6.0) 21 (3.8) 97 (4.9) 1.00 1.04 (0.65, 1.69) 0.82 (0.33, 2.03) Unemployed Employed No mother P for trendb Father: Not literate Elementary Secondary No father Total 0.1 Terms included in the multivariate model (in addition to those shown in the table): sex, age (4 levels), weight-for-height z scores (3 levels), dietary vitamin A intake (5 levels), birth place (2 levels), crowding (4 levels), cigarette smoking and indoor air pollution (4 levels). b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. a medium pollution level compared with those experiencing the lowest level was more than those in next higher level: 2.66 (95% CI:1.33, 5.32), but the risk for those with the highest level was slightly less. When children in the highest three levels were compared with children in the lowest level indoor air pollution level was significantly associated with ALRI risk (Adjusted RR: 1.79 and 95% CI: 1.16, 2.75). There was an increase in risk of ALRI with greater number of cigarettes smoked at home, but this also did not achieve statistical significance. We observed a statistically significant reduction in the risk of ALRI with increasing number of persons per room of the household (Table 5). We evaluated whether this is due predominantly to the numerator (number of household residents) or the denominator (number of rooms in the house). There was a decrease in the rate of ALRI with both increasing number of residents and rooms (data not shown). Discussions We found that employment of the head of the household, but not other maternal or paternal characteristics, was significantly associated with decrease risk of ALRI in children. Indoor air pollution was a significant risk factor for ALRI and, to a lesser extent, use of bio-mass fuel and environmental tobacco smoke were also associated with risk of ALRI. Since data collection was done within a prospective cohort design our findings are unlikely to be due to selection bias. Non-random bias is also unlikely since information on putative risk factors was collected at baseline before the occurrence of ALRI. We have controlled in the analysis for a number of potentially confounding variables such age and nutritional status. Our finding of a significant association with the employment status of the head of the household, despite minimal association with household income level could be due to: (1) incorrect income information, related to a reluctance to volunteer such a sensitive information, (2) the variation of levels of income in the study population was not marked and (3) the effect of employment in reducing risk of ALRI may be mediated by factors separate from income levels. 20 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Table 4: Relative risks of ALRI according to the cooking environment characteristics of households, Addis Ababa, 1993. Characteristics Type of cooking fuel Electricity Kerosene Charcoal/wood/dung Smoke clearance Population (%) ALRI cases(%) Adjusted RR (95% CI)a 200 (10.0) 1,364 (68.5) 428 (21.5) 6(3.0) 69(5.0) 22(5.1) 1.00 1.08 (0.46, 2.56) 1.54 (0.61, 3.87) Inadequate Adequate Kitchen and child bedroom 471 (23.6) 1,521 (76.4) 25(5.3) 72(4.7) 1.00 0.93 (0.60, 1.45) Not separate Separate Cooking in child bedroom 1,447 (72.6) 545 (27.4) 78(5.4) 19(3.4) 1.00 0.79 (0.45, 1.37) Yes No Functional window in child bedroom 1,460 (73.3) 532 (26.7) 79(5.4) 18(3.3) 1.00 0.62 (0.35, 1.08) Not Available Available Total 1,089 (54.7) 903 (45.3) 1,992 (100.0) 60(5.5) 37(4.1) 97 (4.9) 1.00 0.82 (0.53, 1.28) 1.00 P-value (for trend)b 0.2 Terms included in the multivariate model (in addition to those shown in the table): sex, age (4 levels), weight-for-height z scores (3 levels), dietary vitamin A intake (5 levels), household income (3 levels), birth place (2 levels), crowding (4 levels) and cigarette smoking (3 levels). b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. a In our data maternal education or age were not risk factors for ALRI. Several studies have shown maternal education as a determinant of child survival (45,46), and nutritional status (47). ARI-specific child mortality was shown to be associated (48,49), and not to be associated (50) with maternal education in case-control studies. ALRI occurrence was not associated with maternal education in several studies conducted in Columbia, Uruguay and Guatemala (51), but these data were based only on crude analysis. Our findings of no association between maternal and paternal factors may be a result of our controlling for nutritional factors in the analysis. This can happen if the effect of parental factors are mediated through the effect of malnutrition. Malnutrition is a strong predictor of ALRI both in our study and as was shown by a number of other studies reviewed by Graham (20), and Stansfield and Shepard (22). On the other hand, our crude analysis also show no association between maternal or paternal factors and ALRI. This may indicate that these factors may in fact have no effect on ALRI. The relative protection against child mortality afforded by maternal education seen in other continents was not as marked in African countries (46). This has been ascribed, inter alia, to the much greater autonomy of women in sub-Saharan Africa than in many Asian and Muslim communities; enhanced outreach health service programs, in African countries may dampen the effect of maternal education on child survival. It is, however, difficult to extend these explanations to ALRI occurrence based on data from our study. We have also shown a two- to three-fold increase in risk of ALRI with indoor air pollution. Although our definition of indoor air pollution levels was not based on gaseous or particulate exposure assessment of homes, a large number of such assessments in developing countries, including African countries, have shown levels of particulate concentration between 1,000 and 8,000 micrograms per cubic meter, a five- to 30-fold increase compared to levels in industrialized countries (52). Qualitative observations of households in Addis Ababa indicate that the levels of indoor air pollution are not substantially different from the rest of the developing worldb. _______________________________________ b Ethiopian Energy Authority. Background paper on household energy presented to the workshop on Natural Strategy for Health and Household Energy, Nazareth 21-25 March 1994. 21 ──────────────────────────────────────────────────────────── Table 5: Relative risks of ALRI according to levels of indoor air pollution of homes, Addis Ababa, 1993. _______________________________________________________________________________________________________________________________ Characteristics Population (%) ALRI cases(%) Adjusted RR (95% CI)a P-value (for trend)b Indoor pollution levelc Low 422 (21.1) 11 (2.6) 1.00 0.2 Medium 513 (25.8) 35 (6.8) 2.66 (1.33, 5.32) High 738 (37.0) 35 (4.7) 1.68 (0.83, 3.40) Very high 319 (16.0) 16 (5.0) 1.88 (0.84, 4.23) Cigarette smoking in the home None < 10 /24 hrs 10 or more Number of persons per room 1,702 (85.4) 228 (11.4) 62 (3.1) 81 (4.7) 12 (5.2) 4 (6.4) 1.00 1.05 (0.56, 1.95) 1.82 (0.65, 5.07) 0.3 Under 3 3-4 5-6 Over 6 238 (11.9) 893 (44.8) 521 (26.2) 340 (17.1) 1,992 (100.0) 15 (6.3) 57 (6.3) 13 (2.5) 12 (3.5) 97 (4.9) 1.00 0.77 (0.42, 1.41) 0.36 (0.16, 0.78) 0.56 (0.25, 1.26) 1.00 0.02 Total Terms included in the multivariate model (in addition to those shown in the table): sex, age (4 levels), weight-for-height z scores (3 levels), household income (3 levels), dietary vitamin A intake (5 levels), birth place (2 levels), crowding (4 levels) and cigarette smoking (3 levels). b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. c Composite score based on levels of smoke clearance, separation of kitchen and child bedroom, cooking in child bedroom, and, availability of functional windows. a Several studies, which did not adjust for potential confounders in their analysis, have shown an excess risk of ARI due to indoor air pollution (39-44), while two studies in the Gambia which adjusted for potential confounder show an increase in the risk of ALRI (53) but no increased risk for ARI mortality (50). Biomass smoke contains significant amount of pollutants such as particulates, carbon monoxide, hydrocarbons, and to a lesser extent nitrogen oxides. Kerosine burners also increase nitrogen oxide levels in the indoor air. Animal experimental studies have shown that high levels of these pollutants affect the respiratory system adversely. Defects in macrophage phagocytic activity, bacterial uptake and decreased muco-ciliary clearance have been shown (54). Environmental tobacco smoke (ETS) has been shown to affect mechanical defense, phagocytic, T-cell, β-cell and non-specific immunity and thus increase risk of ARI. The pathogenesis of ARI from biomass fuel is similar to that of ETS (55). Although ETS was associated with ALRI in our study the risk was not statistically significant, probably as a result of the modest level of smoking in the study households. A large number of studies in developed and developing countries have now implicated ETS as a risk factor for ARI in children. (50,53,56,57). The finding of a fairly strong increased risk of ALRI with decreasing levels of crowding is a reflection of the following: a decreased ALRI risk with increasing (1) number of people living and (2) number of rooms in the household. Although a large number of studies have shown an association between ARI and crowding, as reviewed by Graham (20) and Stansfield and Shepard (22), there are only a few studies that examined the relationship between crowding and ALRI, at the same time adjusting for potential confounders. Case-control studies from the Gambia (50) and south Brazil (48) have shown an increased risk of mortality from ARI with crowding. A study of measles case-fatality from urban Guinea-Bissau indicated that crowding increases the severity of measles (and presumably the occurrence of measles pneumonia) in young children (58). This finding was based on a beforeafter comparison of severity after introduction of a vaccination program and thus did not have concurrent controls nor was any adjusted analysis done. In any case, our cohort of children was largely vaccinated for measles as a result of a national campaign between 1988 and 1990 c. An increased propagation of microbial agents as a result of crowding can explain increased ARI incidence but not ALRI recurrence. Colonization of the naso-pharynx of children by potential respiratory pathogens in developing countries (51), including Ethiopia (59), is universal and is not considered as a sufficient 22 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── cause of ALRI (60). On the other hand, we can not rule out the possibility that our finding of a linear 60-70% reduction in the risk of ALRI with crowding may be the result of a residual confounding by another household or individual risk factor for ALRI. In conclusion, these findings provide evidence that indoor air pollution is a risk factor for ALRI occurrence and that this excess risk is independent of other familial or individual risk factors for ALRI in children. Our findings emphasize the importance of enhancing current efforts to control indoor air. _______________________________________ c UNICEF. Children and women in Ethiopia. UNICEF, Addis Ababa 1993. Acknowledgement This study was done as a doctoral thesis work by Dr. Derege Kebede at the Department of Epidemiology, Harvard School of Public Health. His training at Harvard was supported by a fellowship grant from the World Health Organization. The study was supported by a grant from the Rockefeller Foundation African Dissertation Internship Awards Program. Additional support was also obtained from the Departments of Epidemiology and Nutrition at Harvard University and the Department of Community Health, Addis Ababa University and the Ethiopian Nutrition Institute. We thank Drs. Lulu Muhe, Damte Shimelis, Ferehiwot Kebede, Hana Afeworki and Tsege Y/Amlak, from the Ethio-Swedish Children's Hospital in Addis Ababa, for their assistance in the evaluation of children for ALRI; the directors and physicians of the Tekle-Haimanot Health Center, Beletshachew MCH Clinic, and Berla Clinic, for their collaborations in making available clinical data of study children seen at these facilities. We would also like to acknowledge the mothers and other caretakers of study children, field workers, supervisors, clerical workers who have made the conduct and reporting of the study possible. We are grateful to Dr. Tigest Ketsela for her expert assistance during data collection, processing and analysis, and for reviewing an earlier draft of this manuscript. References 1. Bulla A and Hitze KL. Acute respiratory infections: a review. Bull WHO 1978;56(3):481-498. 2. Leowsky J. Mortality from acute respiratory infections in children under 5 years of age global estimates. World Health Stat. Q. 1986;39:138-44 3. IUATLD Working Group on ARI. Acute respiratory infections: a high priority. Tubercle and Lung Disease. 1993;74:1. 4. Freij L and Wall S. Exploring child Health and its ecology: The Kirkos Study in Addis Ababa. Acta. Pediatr. Scand. Suppl. 267(1977). 5. Dodge, R.E. and Demeke T. The Epidemiology of Infant Malnutrition in Dabat. Ethiop Med J. 1970;8:53-72. 6. Shamebo D. Fertility and infant mortality in Dembia plain, Gondar. Ethiop Med J. 1978;16:9597. 7. Tafesse B. Analysis of admissions of the Ethio-Swedish pediatric clinic (1970-71). Ethiop Med J. 1973;11:3-12. 8. Shamebo D. Epidemiology for public health research and action in a developing society: The Butajira Rural Health Project in Ethiopia. [Dissertation]. Umea, Sweden: Umeå University, 1993. 9. Muhe L et al. A one-year Community Study of under-five in rural Ethiopia: Patterns of morbidity and public health risk factors. Public Health. in Press. 10. Lindtjorn B, Alemu T and Bjorvatn B. Child health in arid areas of Ethiopia: Longitudinal study of the Morbidity in Infections diseases. Scand J Infect. Dis. 1992;24:369-77. 11. Dingle JH et al. A study of illness in a group of Cleveland families I Plan of study and certain general observations. Am J Hyg. 1953;58:16-30. 12. Brimblecombe FSW et al. Family studies of respiratory infections. Br. Med. J. 1958;1:119-28. 23 ──────────────────────────────────────────────────────────── 13. Fox JP et al. The Seattle Virus Watch: II Objectives, study population and its observation, data processing and summary of illnesses. Am J Epidemiol. 1972;96:270-285. 14. Monto AS, Napier JA and Metzner HI. The Tecumseh study of respiratory illness: I Plan of the study and observations on syndromes of acute respiratory disease. Am J Epidemiol. 1971;94:269-279. 15. Monto AS and Ullman BM. Acute respiratory illness in an American community: The Tecumseh study. JAMA 1974;227(2):164-69. 16. Feldman RA et al. Infection and disease in a group of south Indian families: I Introduction, methods, definitions and general observations in a continuing study. Am J Epidemiol 1969;89:364374. 17. Kamath KR et al. Infection and diseases in a group of south Indian families. II General morbidity patterns in families and family members. Am J Epidemiol. 1969;89:375-83. 18. Black RE et al. Longitudinal studies of infectious diseases and physical growth of children in rural Bangladesh. I Patterns of morbidity. Am J Epidemiol. 1982;115:305-14. 19. James JW. Longitudinal Study of the morbidity of diarrheal and respiratory infections in malnourished children. Am J Clin Nutr. 1972;25:690-94. 20. Graham NM. The epidemiology of acute respiratory infections in children and adults: a global perspective. Epidemiol Rev. 1990;12:149-78. 21. Garenne M, Ronsmans C and Campbell H. The magnitude of mortality from acute respiratory infections in children under 5 years in developing countries. World Health Stat Q. 1992;45(2-3):18091. 22. Stansfield SK and Shepard DS. Acute respiratory infection. In: Jamison DT, Mosley WH, Measham AR and Bobadilla JL eds, Disease control priorities in developing countries. New York: Oxford university Press 1993:67-90. 23. Rothman KJ. Modern epidemiology. Boston: Little, Brown and Company 1986. 24. Wafula EM, Muruka J. Chest X-Rays in children with acute respiratory infections or bronchospasm at Kenyatta National Hospital. East Afr Med J. 1984;61(12):900-6. 25. Campbell H et al. Assessment of clinical criteria for identification of severe acute lower respiratory tract infections in children. Lancet 1989 Feb. 11;1(8633):297-9. 26. Cherian T et al. Evaluation of simple clinical signs for the diagnosis of acute lower respiratory tract infection. Lancet 1988;2:125-128. 27. Mulholland EK et al. Standardized diagnosis of pneumonia in developing countries. Pediatr. Infect. Dis. J. 1992 Feb;11(2);77-81. 28. Redd SC et al. Clinical signs of pneumonia in children attending a hospital outpatient department in Lesotho. Bull WHO. 1994;72(1):113-18. 29. Melia RJW et al. Association between gas cooking and respiratory disease in children. Br Med J. 1977;2:149-152. 30. Melia RJW, Florey CduV and Chinn S. The relation between respiratory illness in primary school children and the use of gas for cooking. I result from a national survey. Int J Epidemiol. 1979;8:333338. 31. Tager IB et al. Longitudinal study of the effects of maternal smoking on pulmonary function in children. N Engl J Med. 1983;309:699-703. 32. Ware JH et al. Passive smoking, gas cooking, respiratory health of children living in six cities. Am Rev Resp Dis. 1984;129:366-374. 33. Honicky RE, Osborne JS and Akpom CA. Symptoms of respiratory illness in young children and the use of wood-burning stoves for indoor heating. Paediatrics 1985;75:587-93. 34. Berkey CS et al. Indoor Air pollution and pulmonary function growth in preadolescent children. Am J Epidemiol. 1986;123:250-60. 35. Morris K et al. Wood-burning store and lower respiratory tract infection in American Indian 24 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Children. Am J Dis Child. 1990;144(1):105-8. 36. Schilling RSF et al. Lung function, respiratory disease and smoking in families. Am J Epidemiol. 1977;106:274-283. 37. Keller MD et al. Respiratory illness in households using gas and electricity for cooking I Survey of incidence. Environ Res. 1979;19:495-503. 38. Hosein HR and Bouhuys A. Possible Environmental Hazards of Gas Cooking Br Med J. 1979;1:125 39. Kossovo D. Smoked-filled Rroms and lower respiratory disease in infants. S Afr Med J. 1982;61:622-24. 40. Sofoluwe GO. Smoke pollution in dwellings of infants with bronchopneumonia. Arch Environ Health 1968;16:670-2. 41. Sofoluwe GO. The effect of housing conditions on prevalence of bronchitis- bronchiolitis and bronchopneumonia in Lagos, Nigeria. West Afr Med J. 1969;35-42. 42. Anderson HR, Respiratory Abnormalities in Papua New Guinea Children : The effects of locality and Domestic wood smoke pollution. Intl J Epidemiol. 1978;7:63-72. 43. Pandey MR et al. Indoor air pollution in developing countries and acute respiratory infections in Children. Lancet 1989;1:427-8. 44. Cruz JR et al. Epidemiology of acute respiratory tract infections among Guatemalan ambulatory preschool children. Rev Infect Dis. 1990;12:S1029-1034. 45. Cleland JG, and Van Ginneken JK. Maternal education and child survival in developing countries: the search for pattern of influence. Soc Sci Med. 1988;27:1357. 46. Hobcraft JN. Women's education, child welfare and child survival: A review of the evidence. Health Transitions Review 1993;3(2):159-75. 47. Thomas D, Strauss J and Henriques MH. How does mother's education affect child height ? Journal of Human Resources 1990;26(2):183-211. 48. Victora CG et al. Risk Factors for Death Due to Respiratory Infections among Brazilian Infants. Int J Epidemiol. 1989; 18:918-25. 49. Victoria CG et al. Maternal education in relation to early and late child health outcomes: findings from a Brazilian cohort study. Soc Sci Med. 1992 Apr; 34(8):899-905. 50. Francisco ADE et al. Risk factors for mortality from acute lower respiratory tract infections in young Gambian Children. Int J Epidemiology. 1993;22:1174-82. 51. Selwyn BJ, et. al. The epidemiology of acute respiratory tract infection in young children: Comparison of finding from several developing countries. Rev Infect Dis. 1990;12:5870-5888. 52. Smith KR and Liu Y. Indoor air pollution in developing countries. In Jonathan Samet, ed. The Epidemiology of Lung Cancer. New York: Marcel Dekker 1993:151-84. 53. Campbell H, Armstrong JRM and Byass P. Indoor air pollution in developing countries and acute respiratory infection in children [letter]. Lancet 1989;1:1012 54. Frampton MW, Samet JM, Utell MJ. Environmental factors and atmospheric pollution. Semin Resp Infect. 1991;6:194-203. 55. Bor DH, and Epstein PR. Pathogenesis of respiratory infections in the disadvantaged. Semin Respir Infect. 1991;6:194-203. 56. Samet JM. Nitrogen Dioxide. Indoor air pollution: A health perspective Samet JM and Spengler JD (eds). The Johns Hopkins Univ. Press, Baltimore 1991. 57. Jim C and Rossignol AM. Effects of passive smoking on respiratory illness from birth to age eighteen months, in Shangai, People's Republic of China J Paediatr. 1993; 123(4):553-8. 58. Aaby P. Malnutrition and over crowding/intensive exposure in severe measles infection: review of community studies. Rev Infect Dis. 1988;10:478-91. 59. Ringertz S et al. Prevalence of potential respiratory disease bacteria in children in Ethiopia. 25 ──────────────────────────────────────────────────────────── Antimicrobial susceptibility of the Pathogens and use of antibiotics among the Children. Acta Paediatr. 1993;82:843-8. 60. IUATLD Working Group on ARI. Acute respiratory infections: conclusions of an IUATLD workshop. Tubercle and Lung Disease. 1993;74:2-5. Original article Nutritional and dietary risk factors of acute lower respiratory infections in under-five children in Addis Ababa, Ethiopia Derege Kebede1, and Walter C Willett2 Summary: This paper reports on the findings of a one-year cohort study of 1,992 children under five years of age conducted in Addis Ababa, Ethiopia, between November, 1991 and December, 1992. The aim of the study was to quantify the relationship between characteristics of children, including proteinenergy malnutrition, dietary vitamin A, and breast-feeding and risk of ALRI (physician diagnosed). Nutritional assessments were conducted using anthropometric measurements (once every month for infants and every three month for older children) and food frequency questionnaires (completed three times at six months interval). Proportional hazards model was used to adjust for several potential confounders. There were 97 incident cases with the cumulative incidence of ALRI being 48.7 per thousand for 12 months of follow-up. Children with weight-for-height z scores less than -3.0 SD had more than four fold increased risk of ALRI compared to those with -2.0 or higher z scores (Adjusted RR: 4.56 and 95% CI: 1.36, 15.8). Children in the upper three quintiles of preformed vitamin A intake has a 25% lower risk of ALRI compared with children in the lowest quintile but the association did not achieve statistical significance (Adjusted RR: 0.82 and 95% CI: 0.46, 1.45). ALRI risk was 50% lower among breast fed children under two years of age (Adjusted RR: 0.55 and 95% CI: 0.22, 1.37). These findings support the importance of continuation of current interventions in the control of PEM and promotion of breast feeding in developing countries. Further larger scale research to quantify the association of vitamin A and other substances in vegetables with ALRI is required.[Ethiop. J. Health Dev. 1997;0(0):27-38] Introduction Acute lower respiratory infections are a major cause of infant and childhood mortality in the developing countries. Bulla and Hitze(1) reported annual mortality rates from ARI to be 48-60 per 100,000 live births in developed countries and 140 per 100,000 in developing countries. For infants under one year of age mortality from ARI was 1,000 per 100,000. They estimated that ARI mortality in Africa was 1,454 and 467 per 100,000 for children under-one and under-five years of age, respectively. Leowsky(2) calculated that 2.5 million infants and 1.5 million children aged 1-4 years die from ARI each year, approximately 98% of those deaths occurring in developing countries. It has now been shown that mortality from ARI is highest in Africa and Central America, followed by south America and Asia, with much lower rates in North America and Europe(3). The discrepancy between the pattern of morbidity of ARI in developed and developing countries (which were similar) and the patterns of mortality (which were different) indicated that a component part of ARI, specifically ALRI occurrence may be higher in developing countries. Studies in several developing countries completed in 1980s showed this to be the case. Stansfield and Shepard(4) after reviewing available data reported that the annual incidence of pneumonia ranged between 3 and 4 ______________________________________ 1 From the Department of Community Health, Faculty of Medicine and 2Department of Nutrition, Harvard School Public Health, 665 Huntington Avenue, Boston, MA 02115, USA percent in children under five years of age in industrialized countries as compared to 10-20 percent in Nutritional and dietary risk factors of ALRI 27 ──────────────────────────────────────────────────────────── developing countries, and that mortality due to pneumonia is ten to fifty times higher in developing than developed countries. The excess morbidity and mortality rates from ARI in the developing world indicated that several risk factors could be responsible. Several studies were thus undertaken to identify risk factors for ARI and subsequently a number of potential risk factors were identified. These included household characteristics such as indoor air pollution, crowding and parental education and child characteristics such as poor nutritional status, low birth weight, incomplete immunization in-addition to being a male child under 2 years of age(4-6). With regards to identification and quantification of risk factors a number of unresolved issues remain. Most of the risk factor studies focused more on ARI than on ALRI. Of those which studied ALRI a large proportion defined outcome (ALRI) based on a combination of symptoms instead of clinical diagnosis: definitions with potentially higher sensitivity but lower specificity than those based on clinical diagnoses. Ideally, analytic epidemiologic studies evaluating putative risk factors should be based on a case definition with the highest possible specificity to minimize the likelihood of both random and systematic misclassification, which can bias the results of studies(7). Several studies which have evaluated the validity of definitions of ALRI based on simple symptomatology and respiratory counts have shown variable specificity, ranging between 65% in Kenya(8), to 93% in the Gambia(9) and with intermediate values being reported from India(10) and Lesotho(11). Furthermore, only a few reported findings of a comparison of outcome for several levels of each risk factors instead of for dichotomous levels and evaluate for dose-response relationships at the same time adjusting for potential confounders(5). Studies on vitamin A supplementation, on the other hand, have given conflicting results on its effect on ARI and ALRI morbidity (discussed below), in spite of showing protection against mortality(12,13). Very few studies have been reported which examined the relationship between dietary vitamin A and risk of mortality(14) and none on morbidity in general or ALRI in particular. Thus the ident-ification and quantification of risk factors for ALRI is still important today. This paper reports on the findings of a one-year cohort study of 1,992 children under five years of age conducted in Addis Ababa Ethiopia, between November 1991 and December 1992. The aim of the study was to quantify the relationship between children characteristics, including of protein-energy malnutrition, dietary vitamin A intake, and breast-feeding and risk of ALRI (physician diagnosed). Methods The study was a one-year follow-up of 1,992 children under-five years of age, randomly selected from the inner-city area of Addis Ababa, and was conducted between November 1991 and December 1992. Study area and population: The study area was Woreda (district) 3, one of the 25 city districts, and located at the center of Addis Ababa. Selection of this study area was based on logistic grounds and because it was not appreciably different from other districts of the city in terms of the population age and sex structure, ethnic and religious mix, and socio-economic development. At the onset of the study it was divided into 11 Kebeles (sub-districts) and had an estimated 14,318 households, a population of 71,591, and 8,590 children under five years of age(15). In November of 1991 we conducted a census of all eleven sub-districts to enumerate all children under-five living in the area. Using systematic sampling (every fourth household with an under-five child), we enrolled 2,025 households with one child under-five at the time of the census. In households where more than one child under-five lived, we enrolled the youngest child. Refusals to participate were very few (3%) and were mostly from well-to-do families. Of the 2,025 households initially enrolled, 33 families subsequently moved out of the city and were therefore excluded from the study. All subjects were enrolled at the same time and were followed for one year. All subjects were enrolled at the same time and followed for one year. 28 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Data Collection: We recruited ten women with a high-school education living in the study subdistricts to interview members of households. They were given an intensive two-week training by the investigators before they started the interview. For the anthropometric measurements we obtained an experienced field worker from the Ethiopian Nutrition Institute. All data collection instruments were pilot-tested in a sub-district outside of the study area and the necessary modifications were made before they were used in the study. This sub-district was also used for field training of the field workers and supervisor. Household Characteristics: At baseline data on the following was collected: (1) sociodemographic characteristics of all members of households and (2) physical characteristics of homes, cooking area, and child's bedroom. We categorized study children into four levels of indoor air pollution by calculating a composite score based on level of smoke clearance, separation of kitchen and the child's bedroom, absence of cooking in child's bedroom, and the presence of functional windows. The referent category represented the absence of all of the above conditions, the second level the presence of any one or two, the third any three, and the fourth level represented the combination of all of the four conditions. Child Characteristics: Data on medical history of each child, including family history of respiratory ailments were also collected at baseline. We requested mothers to present the child's vaccination cards and for over 95% of children data on immunization status were collected from these cards. Breastfeeding information, including supplementary feeding practices, were collected at baseline and every month thereafter for children under one-year of age and every three months for older children. Weight and height/length were also measured at baseline and subsequently every month for children under one year and every three months for older children. Weight was measured to the nearest 100 g using a digital bathroom scale, standardized several times during the course of the study. For small children, both mother and child were weighed first, followed by the mother alone and the child weight was calculated by difference. Height was measured to the nearest 0.5 cm using a height stick with movable head piece against a flat surface. For small children, length was measured in a recumbent position with a length board. Z scores were computed to categorize levels of weight-for-height, weight-for-age and height-forage, according to the NCHS standard. Normal: >-2.0 SD, moderate: between -2.0 and -3.0, and severe: -3.0 SD and below(16). Dietary information was collected using food frequency questionnaires developed locally. An experienced dietitian from the Ethiopian Nutrition Institute was invited to participate in the process of identifying the relevant food items to be included in the FFQ, with the aim of measuring intakes of total calories and vitamin A in Addis Ababa. Food composition tables for use in Ethiopia, East Africa and Africa(17-21) were consulted to work out an initial extensive food list of over 400 items out of which 98 items deemed relevant and able to categorize children by past nutritional intake were selected. This FFQ was then pilot tested on 50 children under-five in a sub-district outside of the study area before it was used in the cohort study. The FFQ were administered by trained and supervised interviewers. Mothers or other caretakers were asked about their children's usual intake in the previous six months for the specific item and portion size on the FFQ and responded in terms of frequency of intake per day, week, month, past 6 months or never. The FFQ was also tested for its validity and reproducibility by comparison to serum retinol determination and seven-day multiple 24-hour diet recall. The findings of the validation study are reported elsewhere (Kebede et al. Submitted to the Int.J.Epidemiol. 1995). We have also examined the role of foodgroups and individual foods as risk factors of ALRI. Foodgroups were categorized as follows. Vegetables included 32-items; all sauce preparations containing kale (Brassica carinata), cabbage, or pepper (Capsicum anuum); carrots, peas, chickpeas, broad beans, split lentils, potatoes, sweet potatoes, pumpkin and tomato. Green leafy vegetables included were sauce preparations containing kale, cabbage, with or without pepper. Non-leafy Nutritional and dietary risk factors of ALRI 29 ──────────────────────────────────────────────────────────── vegetables included the rest of the vegetable group. Fruits included grapes, guava, lemon, orange, prickly pear, banana, papaya, and peach. Dairy included milk (whole, dried, skimmed, powder), wet cheese, yoghurt, butter milk, butter. Meat includes beef, mutton, fish, and poultry. We estimated the frequency of use of specified portion sizes of the foodgroups and foods to evaluate the risk of ALRI in the various quintiles of intake. Measurement of outcome (ALRI): We defined the occurrence of ALRI based on a physiciandiagnosis of pneumonia, bronchiolitis or bronchitis using historical, physical and radiological evaluation. We instituted a surveillance and screening system as follows. At enrollment mothers were requested to take their children to a nearby hospital if they developed cough and fever and were also informed that the cost for the visit would be covered by the study. The mother's agreement to do this was a pre-requisite for enrolment of a child into the study. Interviewers visited study households every two weeks and completed a simple form about symptom histories of respiratory ailments and fever. Caretakers were asked about the occurrence and duration of those symptoms in the previous two weeks; this was done continuously for the one-year of follow-up. If during the time of interview a child had cough and fever, the mother was asked to take the child to a children's hospital nearby (Ethio-Swedish Pediatric Hospital). During their visit field workers also enquired about and recorded whether the child was taken to any other health care unit in the previous two weeks. If such was the case, that health unit was visited to obtain information on the clinical details of the consultation. At the pediatric teaching hospital a nurse initially screened presenting children for occurrence of respiratory symptoms, particularly for cough, fever or breathing difficulties and they were subsequently examined by physicians using standard clinical algorithms worked out before hand. ALRI-diagnosed children were given all the necessary treatment and follow-up by the clinicians. Statistical analysis: A proportional hazards model with time dependent covariates was fitted to the data for analysis. Anthropometric measurements, breast feeding status and dietary variables were included as time dependent covariates with other baseline characteristics. Children who died were considered censored for the rest of the study period. There was no loss to follow up. For nutrient and foodgroup variables, cases reported in the first half of the follow up year were allocated according to the dietary intake assessed at baseline (FFQ1), whereas cases reported in the second half were allocated according to the mean dietary intake at baseline and mid-year (FFQ1 and FFQ2). For breast feeding and anthropometric measurements cases reported in any month were allocated according to the value assessed at the start of the month. A number of potentially confounding variables were included in the model. All nutrient estimates included in the model were first energy-adjusted using regression method as described by Willett22 before their inclusion. To evaluate the presence of an overall trend, adjusted relative risk estimates and test of significance were calculated using continuous independent variables in the multivariate model. A probability level of 0.05 was taken as a cut-off for statistical significance. Data were entered onto a computer using the EPI-INFO program, version 5, CDC, Atlanta GA, and analyzed using the Statistical Analysis System program, version 6.04, SAS Institute, Cary NC. 30 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Table 1: Relative risks of ALRI according to characteristics of children, Addis Ababa, 1993. Characteristics Sex Male Female Age Under 6 months 6-12 months Over 12 months Over 24 months Vaccinated for measles Population (%) ALRI cases(%) Adjusted RR (95 CI)a 1,057 (53.1) 935 (46.9) 55 (5.2) 42 (4.5) 1.00 0.88 (0.57, 1.32) 110 (5.5) 180 (9.0) 378 (19.0) 1,324 (66.5) 10 (9.1) 20 (11.1) 30 (7.9) 37 (2.8) 2.03 (0.96, 4.31) 2.88 (1.57, 5.28) 2.46 (1.48, 4.10) 1.00 No Yes Place of delivery 378 (19.0) 1,614 (81.0) 26 (6.9) 71 (4.4) 1.00 0.90 (0.54, 1.50) P(trend)b 0.01 Home 1,028 (51.6) 75 (7.3) 1.00 Health facility 964 (48.4) 22 (2.2) 0.42 (0.25, 0.68) Total 1,992 (100.0) 97 (4.9) a Terms included in the multivariate model (in addition to those shown in the table): weight-for-height z scores (3 levels), dietary vitamin A intake (5 levels), total caloric intake (5 levels), household income (3 levels), ethnicity (4 levels), crowding (4 levels) and indoor air pollution (4 levels). b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. Scientific and ethical clearance for the study was given by the Research and Publication Committees of the Department of Community Health, the Faculty of Medicine, and the Research and Publication Office of Addis Ababa University. Results A total of 1,992 children were followed for one year. Of these, at baseline 14.5% were infants under one year of age and over 80% were vaccinated for measles (Table 1). About 90% of the households of study children had reported income less than 60 US Dollars per month. The head of the household was unemployed in 58.7%, not literate in 16% or had elementary level education for over 56%, of study children (data shown in paper I). There were 97 incident cases with the cumulative incidence of ALRI being 48.7 per thousand for 12 months of follow-up. There were 14 deaths during the follow up time. Of these two were associated with ALRI, six with diarrheal diseases, four with ARI symptoms, one with electrocution, and one with kidney disease. Of the ALRI cases, 63 were diagnosed as bronc opneumonia, 12 as bronchopneumonia with rickets and marasmus, eight as broncho-pneumonia with otitis media, four as lobar pneumonia, and 10 as bronchiolitis. Both age and delivery in a health service were strong predictors of ALRI risk. The risk of ALRI increased with decreasing age. The test for trend for this increase was statistically significant (P=0.01). The risk of ALRI doubled in children under six months of age when compared to those over 24 months of age (Adjusted relative risk, RR: 2.03 and 95% confidence intervals, CI: 0.96, 4.31). For children delivered at a hospital, health center or clinic the risk of ALRI was lower (Crude RR: 0.42 and 95% CI: 0.25, 0.68). Female sex and measles vaccination were associated with decreased risk of ALRI but this did not achieve statistical significance. Weight-for-height z score was independently and significantly associated with ALRI risk (Table 2). Children with z scores less than -3.0 SD had more than a four fold increased risk of ALRI compared to those with -2.0 or higher z scores (Adjusted RR: 4.56 and 95% CI: 1.36, 15.8). Weight-for-age zscores and height-for-age z scores were not associated with ALRI risk. There was a 25% reduction in the risk of ALRI associated with increased dietary intake of total vitamin A but the association did not achieve statistical significance (Adjusted RR: 0.74 and 95% CI: 0.33, 1.65). This relative risk estimate was somewhat attenuated as a Nutritional and dietary risk factors of ALRI 31 ──────────────────────────────────────────────────────────── Table 2: Relative risks of ALRI according to levels of anthropometric measurements of children, Addis Ababa, 1993. Characteristics Population (%) ALRI cases(%) Adjusted RR (95% CI)a P-value (for trend)b Weight-for-height(wasting) More than -2.0 SD 1,759 (88.3) 86 (4.9) 1.00 0.02 Between -2.0 and -3.0 Sd 34 (1.7) 4 (11.7) 0.40 (0.05, 2.84) Less than -3.0 SD 199 (9.9) 7 (3.5) 4.65 (1.36, 15.8) Weight-for-age (under-weight) More than -2.0 SD Between -2.0 and -3.0 Sd Less than -3.0 SD Height-for-age (stunting) 1,338 (67.1) 361 (18.1) 293 (14.7) 52 (3.9) 22 (6.1) 23 (7.8) 1.00 0.53 (0.19, 1.50) 1.35 (0.52, 3.50) 0.6 More than -2.0 SD Between -2.0 and -3.0 Sd Less than -3.0 SD Total 962 (48.3) 443 (22.2) 587 (29.4) 1,992 (100.0) 46 (4.8) 12 (2.7) 39 (6.6) 97 (4.9) 1.00 0.71 (0.30, 1.68) 0.91 (0.40, 2.05) 0.5 Terms included in the multivariate model: age (4 levels), sex, dietary vitamin A intake (5 levels), total caloric intake (5 levels), household income (3 levels), birth place (2 levels), crowding (4 levels) and indoor air pollution (4 levels). b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. c Z scores were computed to categorize levels of weight-for-height, weight-for-age and height-for-age based on the NCHS standards. a result of adjustment for both total caloric intake and when other socio-demographic and anthropometric variables were included in the model. There was a similar attenuation of the RR associated with preformed vitamin A and total caloric intake. There was no association between provitamin vitamin A and risk of ALRI. Likewise, there was no association between folic acid intake and risk of ALRI. We observed no overall relation between vegetables, green leafy vegetables, and fruits and vegetables and the risk of ALRI (Table 4). Intake of eggs, diary or meat products (beef, mutton or poultry) were not appreciably associated with ALRI. We have also compared children in the upper four quintiles of intake of nutrients and foodgroups with children in the lowest quintile. The adjusted RR (95% CI) for nutrients were as follows: total vitamin A: 0.85 (0.48, 1.52), preformed vitamin A: 0.82 (0.46, 1.45), provitamin A: 1.01 (0.55, 1.87), folic acid: 1.15 (0.60, 2.22), and total caloric intake: 1.64 (0.73, 3.68). For foodgroups the following were obtained: vegetables: 1.00 (0.41, 2.42), leafy vegetables: 1.27 (0.62, 2.62), non-leafy vegetables: 0.97 (0.41, 2.31), fruits: 0.94 (0.49, 1.78), diary: 0.73 (0.42, 1.26), egg: 1.27 (0.65, 2.50) and meat: 0.94 (0.49, 1.79). There was a nonsignificant 50% reduction in ALRI risk with breast feeding in children under two years of age (Adjusted RR: 0.55 and 95% CI: 0.22, 1.37). Terms included in the multivariate model were sex, age, weight-for-height z scores, household income, birth place, maternal age and education, religion, ethnicity, crowding and indoor air pollution. Discussion We have reported on the association of a number of nutritional factors with ALRI risk. Our findings are unlikely to be due to non-random bias as data were collected prospectively prior to the occurrence of illness in cases and without the knowledge the case/non-case status of study children. We have also controlled for a number of potential confounders in the analysis. Age and place of delivery of child were strong predictors of ALRI children. Sex and measles vaccination were not significantly associated with risk of ALRI. The majority of studies which have examined the relationship of age to ARI and ALRI occurrence and mortality have reported an inverse association(4,5,23). Place of delivery of a child is probably a proxy for several household and individual risk factors for ALRI. Most of the 19% of children not vaccinated for measles in our study were not vaccinated because they were under nine months of age. The generally 32 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Table 3: Quintiles of total vitamin A, provitamin A, preformed vitamin A, folic acid and total caloric intake in relation to the risk of developing ALRI in 1,992 children under five years of age in Addis Ababa, Ethiopia 1993 Dietary variable Total vitamin A intake Range of intake (RE/d) Age and sex adjusted RR ..energy-adjusted Rrb Multivariate Rrc Preformed vitamin A Range of intake (RE/d) Age and sex adjusted RR ..energy-adjusted RR Multivariate RR Provitamin A Range of intake (RE/d) Age and sex adjusted RR ..energy-adjusted RR Multivariate RR Folic acid Range of intake (mcg/d) Age and sex adjusted RR ..energy-adjusted RR Multivariate RR Total caloric intake Range of intake (kcal/d) Crude RR (95% CI) Age and sex adjusted RR Multivariate RR (95% CI) Quintile of intake 1 2 <218 218-338 1.00 0.63 (0.28, 1.40) 1.00 0.69 (0.31, 1.53) 1.00 0.63 (0.27, 1.41) P(trend)a 3 339-458 1.04 (0.50, 2.15) 1.05 (0.52, 2.13) 1.12 (0.53, 2.37) 4 459-680 0.80 (0.35, 1.80) 0.73 (0.34, 1.57) 0.95 (0.41, 2.17) 5 >680 0.65 (0.30, 1.41) 0.60 (0.28, 1.31) 0.74 (0.33, 1.65) 0.1 0.2 0.3 <0.80 1.00 1.00 1.00 0.80-5.8 0.38 (0.15, 1.00) 0.39 (0.15, 1.00) .39 (0.15, 1.00) 5.9-15.8 0.74 (0.34, 1.60) 0.75 (0.35, 1.61) 0.88 (0.40, 1.90) 15.9-49 0.92 (0.44, 1.88) 0.85 (0.42, 1.75) 1.03 (0.50, 2.15) >49 0.85 (0.42, 1.71) -0.87 (0.43, 1.75) 1.07 (0.52, 2.24) 0.3 0.4 0.5 <203 1.00 1.00 1.00 203-322 .80 (0.41, 2.01) 0.97 (0.45, 2.11) 0.99 (0.44, 2.22) 323-430 0.93 (0.40, 2.17) 0.88 (0.40, 1.95) 1.07 (0.46, 2.52) 431-657 0.91 (0.37, 2.21) 0.74 (0.33, 1.67) 0.97 (0.39, 2.40) >657 1.09 (0.52, 2.31) 0.94 (0.45, 1.93) 1.21 (0.57, 2.50) 0.8 0.9 0.8 <93 1.00 1.00 1.00 93-134 1.42 (0.63, 3.18) 1.22 (0.55, 2.68) 1.25 (0.56, 2.80) 135-171 0.78 (0.32, 1.94) 0.72 (0.30, 1.74) 0.80 (0.33, 1.96) 172-237 .16 (0.51, 2.64) 1.08 (0.49, 2.40) 1.28 (0.57, 2.86) >237 1.08 (0.48, 2.44) 0.98 (0.44, 2.17) 1.37 (0.61, 3.10) 0.6 0.4 0.4 <874 1.00 1.00 1.00 874-1 0.61 (0.26 1.07 (0.38 1.18 (0.42 1,232-1,587 1.26 (0.64,2.50) 1.88 (0.76,4.68) 2.01 (0.80,5.01) 1 1.59 (0.84,3.02) 2.24 (0.92,5.48) 2.54 (1.02,6.31) >1,975 0.83 (0.41,1.70) 1.06 (0.39,2.88) 1.27 (0.46,3.53) 0.3 0.4 0.2 Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. In addition to age and sex, total caloric intake (5 levels) included in the model. Terms included in the multivariate model: age (4 levels), sex, weight-for-height z scores (3 levels), total caloric intake (5 levels), household income (3 levels), birth place (2 levels), crowding (4 levels) and indoor air pollution (4 levels). a b c very high level of vaccination observed at baseline in our study was a reflection of a city-wide characteristic due to a national campaign of vaccination conducted between 1988 and 1990 that had effectively reached universal immunization levels in urban centers, particularly Addis Ababa(24). In our study wasting was a strong predictor of ALRI. Our results are in accord with several studies conducted in the past two decades(25-33). Acute protein energy malnutrition rather than chronic may be more important as a risk factor for ALRI. This may explain our finding of no association of between height-for-age z scores and ALRI risk. As was shown by other studies 95% of the variance in weightfor-age is accounted by weight-for-height and height-for-age taken together(34). This may have accounted for the attenuated risk of ALRI associated with weight-for-age z scores. Starting with the early evidence of waning cell-mediated immunity as a result of starvation observed by Jewish physicians of the Warsaw Ghetto in 1942, the mechanism of immune depression is now fairly well described(35,36). To a larger extent PEM affects cell-mediated immunity, and to a lesser degree, humeral immunity but mechanical defense and non-specific immunity are also affected. The findings we reported on dietary vitamin A intake indicate only a modest association between risk of ALRI and low intake of dietary vitamin A intake. Our findings may be due to several factors: (1) there may be due to a low variation in the level of intake of vitamin A among the study children. Total vitamin intake varied between 340 RE/d or below in the lowest two quintiles and 460 RE/d or above in the upper two quintiles. Similarly, provitamin A intake varied between 322 RE/d or below and 431 RE/d and above, in the two Nutritional and dietary risk factors of ALRI 33 ──────────────────────────────────────────────────────────── Table 4: Relationship of food groups and individual foods to the risk of ALRI in 1,992 children under five years of age in Addis Ababa, Ethiopia 1993 Food groupsa Vegetables Green leafy vegetables Non-leafy vegetables Fruits Vegetable & fruits Diary Meat Eggs Quintile of intake 1 2 1.00c 0.58 (0.19, 1.78) 1.00 1.30 (0.55, 3.05) 1.00 0.56 (0.18, 1.67) 1.00 0.77 (0.34, 1.75) 1.00 0.85 (0.30, 2.45) 1.00 0.47 (0.19, 1.12) 1.00 0.82 (0.36, 1.85) 1.00 1.68 (0.93, 3.03) P(trend)b 3 1.26 (0.45, 3.56) 1.28 (0.54, 3.04) 1.21 (0.43, 3.36) 1.13 (0.52, 2.46) 1.10 (0.38, 3.16) 0.65 (0.30, 1.38) 0.67 (0.29, 1.56) 2.21 (0.94, 5.22) 4 0.65 (0.20 0.56 (0.14 0.83 (0.27 0.97 (0.43 0.68 (0.21 0.73 (0.27 1.47 (0.57 1.57 (0.80 5 1.00 (0.29, 3.43) 1.43 (0.62, 3.28) 1.03 (0.31, 3.40) 0.92 (0.38, 2.24) 1.22 (0.34, 4.27) 0.93 (0.47, 1.82) 0.99 (0.44,2.23) 1.03 (0.38, 2.77) 0.3 0.8 0.5 0.6 0.4 0.2 0.5 0.3 Vegetables included (32-items): all sauce preparations containing kale (Brassica carinata), cabbage, or pepper (Capsicum anuum); carrots, peas, chickpeas, broad beans, split lentils, potatoes, sweet potatoes, pumpkin and tomato. Green leafy vegetables included were sauce preparations containing kale, cabbage, with or without pepper. Non-leafy vegetables included the rest of the vegetable group. Fruits included grapes, guava, lemon, orange, prickly pear, banana, papaya, and peach. Dairy included milk (whole, dried, skimmed, powder), wet cheese, yoghurt, butter milk, butter. Meat includes beef, mutton, fish, and poultry. b Test for trend was obtained from the multivariate model with the characterstics included as continuous independent variables. c Terms included in the multivariate model: age (4 levels), sex, weight-for-height z scores (3 levels), total caloric intake (5 levels), household income (3 levels), birth place (2 levels), crowding (4 levels) and indoor air pollution (4 levels) a lower and two upper quintiles of distribution of intake, respectively. Such variations in these nutrients among the study children were modest. On the other hand, variations in intake of preformed vitamin A were more marked, there being a three-fold difference in preformed vitamin A intake between the two lowest and two upper quintiles. (2) The precision of the food frequency questionnaire which we have used to collect data may not be sufficiently high to discriminate the underlying differences. The correlation coefficients of the FFQ with serum retinol determinations among a sub-sample of study children were modest, 0.22 and 0.15, 0.25, for total, pro- and preformed vitamin A, respectively (Kebede et al. Submitted to the Int.J.Epidemiol. 1995). Although these results could be manifestations of the use imperfect gold standards, such as serum retinol levels(22), it is difficult to evaluate this in the present study. (3) A lack of adequate statistical power considerations could also explain our results. The number of cases was modest, which is reflected in the wide 95% confidence intervals of our relative risk estimates. (4) Another possibility is that long term intake rather than medium term intake may be a risk factor. The time period of enquiry for levels of dietary intake in our study was between one and one-half year. Although dietary intake pattern prior to this time may in theory be relevant, and thus not taken into account, the relevant period of exposure for ALRI in children is unlikely to be beyond two years (5). Although we have tried to adjust for a number of potential confounders in our study, we cannot rule out the possibility of a negative confounding by an unmeasured variable attenuating the relative risk estimates. (6) Finally, it is possible that vitamin A in fact may not be related to the risk of ALRI, and that other nutrients or substances may be responsible for the reduction in risk of ALRI. Our data also suggest that folic acid is not protective of ALRI, although the results should be interpreted with caution. Folic acid levels in foods are labile as they are markedly affected by food storage and processing, and food composition data on them are not very reliable(22). The results indicate a need for further research, as substances in vegetables and diary foods other than vitamin A could also protect against ALRI. The reduction of child mortality as a result of vitamin A supplementation is now fairly well established(12,13). On the other hand, the effects of vitamin A supplementation on morbidity, particularly respiratory infections have not been consistent. Vitamin A supplementation did not influence the incidence, severity or duration of respiratory infections in Tamil Nadu, India(37), Hydrabad, India(38), Indonesia(39), Nepal(40) or in Ghana(41). A trial from Haiti reported an increased risk of respiratory signs of both ARI and ALRI after vitamin A supplementation(42). However, trials from north Thailand(43) and Australia(44) have reported reduced risk of ARI after vitamin A supplementation. There are very few reports of studies that evaluated dietary vitamin A intake and ARI. In the 34 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── vitamin A trial in the Sudan dietary vitamin A intake was associated with reduced risk of cough and fever, but with an increased risk of cough alone (Fawzi et al 1995 unpublished data). Earlier reports from the same trial had shown that dietary vitamin A intake was a strong predictor of xerophthalmia(45), and mortality(14). Furthermore the effects of vitamin A level on ALRI risk could be mediated through its effect on growth. Two community trials in Indonesia have shown an increased weight gain(46) and height gain(47) after vitamin A supplementation. PEM has been shown to be a strong predictor of ALRI in this study. Although not fully resolved the weight of the evidence seems to indicate that dietary vitamin A intake to be protective of ALRI but the variation in vitamin A intake levels were not that high for the study to detect an association. The effect of vitamin A on tissue growth and the consequences of its deficiency on epithelial tissue and the body's resistance to infection has been recognized for some time(48,49). Vitamin A deficiency also impairs muco-ciliary clearance(50), and systemic defense mechanisms(36) increasing the risk of ALRI. Our data on breast feeding show the protection is afforded to children against ALRI. Because of the small number of young children who are cases in our sample the relative risk estimate did not achieve statistical significance despite a 50% reduction in risk. This finding of reduced risk of ALRI due to breast feeding is in accord with other studies conducted in Rwanda(51) and south Brazil(52), although a well designed case-control study from the Gambia did not show the protection of breast feeding against ARI mortality(33). On the other hand, several studies from industrialized countries have given conflicting results on the effects of breast feeding on ARI. The methodologic difficulties in studying breast feeding which is a proxy to complex physical and social determinants of risk of ALRI has been stated(53). Bauchner et al(54) after reviewing twenty studies on breast feeding and infection in industrialized countries concluded that only six studies met acceptable methodological standards. The result of these studies suggested that breast feeding had a minimal protective effect on risk of infections in industrialized countries. More recently Ford and Labbock(55) have reported breast feeding as providing some protection for pneumonia after adjusting for several potentially confounding variables in a large national sample of US children 1-2 years of age at the time of the survey in 1981. The protective effects of breast feeding is probably mediated through specific immune mechanisms particular humoral immunity (36, 56), by its being an important alternative to potentially contaminated fluids and reduction of contacts during early months of life(57). Its being an alternative to potentially contaminated fluids is probably more relevant to diarrheal diseases than ALRI, although repeated diarrheal attacks can predispose children to PEM and thus to ALRI. Similarly, repeated upper ARI as a result of early contact with others can predispose children to PEM. In conclusion, our study shows protein energy malnutrition, breast feeding, and probably and to a lesser extent dietary vitamin A, as independent risk factors of ALRI occurrence in children. This findings indicate the importance of continuation of current interventions in the control of PEM and promotion of breast feeding in developing countries. Further larger scale research to quantify the association of vitamin A and other substances in vegetables with ALRI is required. Acknowledgement This study was done as a doctoral thesis work by Dr. Derege Kebede at the Department of Epidemiology, Harvard School of Public Health. His training at Harvard was supported by a fellowship grant from the World Health Organization. The study was supported by a grant from the Rockefeller Foundation African Dissertation Internship Awards Program. Additional support was also obtained from the Departments of Epidemiology and Nutrition at Harvard and the Department of Community Health, Addis Ababa University and the Ethiopian Nutrition Institute. We thank Dr. Hana Neka-Tibeb and W. Elizabeth Wubeneh for expert assistance in the nutritional and dietary assessment of children; Drs. Lulu Muhe, Damte Shimelis, Ferehiwot Kebede, Hana Afeworki and Tsege Y/Amlak, from the Ethio-Swedish Children's Hospital in Addis Ababa, for their assistance in the Nutritional and dietary risk factors of ALRI 35 ──────────────────────────────────────────────────────────── evaluation of children for ALRI; the directors and physicians of the Tekle-Haimanot Health Center, Beletshachew MCH Clinic, and Berla Clinic, for their collaborations in making available clinical data of study children seen at these facilities. We would also like to acknowledge the mothers and other caretakers of study children, field workers, supervisors, clerical workers who have made the conduct and reporting of the study possible. We are grateful to Dr. Tigest Ketsela for her expert assistance during data collection, processing and analysis, and for reviewing an earlier draft of this manuscript. References 1. Bulla A and Hitze KL, Acute Respiratory Infections: a review Bull. WHO 1978;56(3):481-498. 2. Leowsky J. Mortality from acute respiratory infections in children under 5 years of age global estimates. World Health Stat. Q. 1986;39:138-44 3. IUATLD Working Group on ARI Acute respiratory infections: a high priority. Tubercle and Lung Disease. 1993;74:1. 4. Stansfield SK and Shepard DS Acute respiratory infection. In: Jamison DT, Mosley WH, Measham AR and Bobadilla JL eds, Disease control priorities in developing countries. New York: Oxford university Press 1993:67-90. 5. Graham NM. The epidemiology of acute respiratory infections in children and adults: a global perspective. Epidemiol. Rev. 1990;12:149-78. 6. Garenne M, Ronsmans C and Campbell H. The magnitude of mortality from acute respiratory infections in children under 5 years in developing countries. World Health Stat Q. 1992;45(2-3):18091. 7. Rothman KJ. Modern epidemiology. Boston: Little, Brown and Company 1986. 8. Wafula EM, Muruka J. Chest X-rays in children with Acute Respiratory Infections or Bronchospasm at Kenyatta National Hospital. East. Afr. Med. J1984;61(12):900-6. 9. Campbell H. Byass P. Lamont AC, Forqie IM, O'Neill KP, Lloyd-Evans N. Greenwood BM. Assessment of clinical criteria for identification of severe acute lower respiratory tract infections in children. Lancet 1989 Feb. 11;1(8633):297-9. 10. Cherian T. John TJ, Simoes E. Steinhoff MC, and John M. Evaluation of simple clinical signs for the diagnosis of acute lower respiratory tract infection. Lancet 1988;2:125-128. 11. Redd SC, Vreuls R, Metsing M, Mohobane PH, Patrick E. and Moteetee M. Clinical signs of pneumonia in children attending a hospital outpatient department in Lesotho. Bull. WHO. 1994;72(1):113-18. 12. Fawzi WW, Chalmers TC, Herrera MG and Mosteller F. Vitamin A supplementation and child mortality: a meta analysis. JAMA 1993;269:898-903. 13. Glaziou PP and Mackerras DEM. Vitamin A supplementation and child mortality: a meta-analysis British Medical J. 1993;306:366-70. 14. Fawzi WW, Herrera MG, Willett WW, Nestel P. Amin AE, Lipsity S and Mohamed KA. Dietary vitamin A intake and the risk of mortality among children Am. J. Clin. Nutr. 1994;59:401-8. 15. Population & Housing Census Commission. Population and Housing Census of Ethiopia, 1984: Analytical report on results for Addis Ababa. Addis Ababa, January 1987; 1(1). 16. Frisancho AR Anthropometric standards for the assessment of growth and nutritional status. Ann Arbor: The University of Michigan Press 1990. 17. Ågren G and Gibson R. Food composition table for use in Ethiopia I. Addis Ababa: Ethiopian Nutrition Institute 1968. 18. Ethiopian Nutrition Institute. Ethiopian Traditional Recipes Addis Ababa: Ethiopia Nutrition Institute 1980. 19. Gobezie A. Manual for hospital diets for use in Ethiopia Addis Ababa: Ethiopian Nutrition Institute c1970. 20. West CE, Pepping F and Temalilwa eds. The composition of foods commonly eaten in east Africa. 36 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Wageningen: Wageningen Agricultural University 1988. 21. Food and Agricultural Organization Food composition table for use in Africa Rome: Food and Agricultural Organization 1968. 22. Willett WC. Nutritional epidemiology. Oxford University Press, New York, 1990. 23. Berman S. McIntosh K. Selective Primary Health Care: Strategies for control of diseases in the developing world XXI. Acute respiratory infections. Rev. Infect. Dis. 1981;3:246-53. 24. UNICEF. Children and women in Ethiopia. UNICEF, Addis Ababa 1993. 25. James JW. Longitudinal Study of the morbidity of diarrheal and respiratory infections in malnourished children. Am. J. Clin. Nutr. 1972;25:690-94. 26. Berman S. Duenas A. Bedoya A. Constain V. Leon S. Borrero I and Murphy J. Acute lower respiratory tract illnesses in Cali, Columbia: A two- year Ambulatory Study Paediatrics. 1983;71:210218. 27. Tupasi TE, Velmonte MA, Sanvictores MEG. Determinants of morbidity and mortality due to acute respiratory infections: Implications for Infection. J. Infect Dis. 1988;157:615-23. 28. Tupasi TE, Mangubat NV, Sunico MES, Magdangal DM, Navarro EE, Leonor ZA, Lupisan S, Medalla F and Lucero MG. malnutrition and acute respiratory tract infections in filipino children. Rev. Infect. Dis. 1990;12: S1047-1054. 29. Victora CG, Barros FC, Kirkwood Br, Vaughan JP. Pneumonia, Diarrhoea and Growth in the First 4 year of Life: A longitudinal Study of 5914 Urban Brazilian Children. Am. J. Clin. Nutr. 1990;52(2):391-6. 30. Spooner V, Barker J, Tulloch S, Lehmann D, Marshall TF, Kajoi M and Alpers MP. Clinical signs and risk factors associated with pneumonia in children admitted T. Goroka Hospital, Papua New Guinea. J. Trop. Pediatr. Dec. 1989;35(6);295-300. 31. Selwyn BJ, et. al. The epidemiology of acute respiratory tract infection in young children: Comparison of findings from several developing countries. Rev. Infect. Dis. 1990;12:5870-5888. 32. Kirkwood BR Acute respiratory infections. In: Feachem RG and Jamison DT eds, Disease and mortality in sub-Saharan Africa. New York: Oxford University Press 1991:158-72. 33. Francisco ADE, Morris J, Hall AJ, Armstrong Schellenberg JRM and Greenwood BM. Risk Factors for mortality from acute lower respiratory tract infections in young Gambian Children. Int. J.Epidemiology 1993;22:1174-82. 34. WHO Working Group. Use and interpretation of anthropometric indicators of nutritional status. Bull. WHO 1986;64(6):929-41. 35. Cunningham-Rundles S. Nutritional factors in immune response in Malnutrition:Determinants and consequences. 1984 Alan R. Liss, Inc., New York. PP. 233-244. 36. Bor DH, and Epstein PR, Pathogenesis of respiratory infections in the disadvantaged. Semin Respir. Infect. 1991;6:194-203. 37. Rahmathullah L, Underwood BA, Thulasira ED and Milton RC. Diarrhoea, respiratory infections, and growth are not affected by the weekly low-dose vitamin A supplement: A masked, controlled field trial in children in Southern India. Am. J. Clin. Nutr. 1991;54:568-77. 38. Vijayaraghavan K. Radhaiah G. Prakasam B. Sarma KVR, Reddy V, Effect of massive dose of vitamin A on morbidity and mortality in indian children. Lancet 1990;336:1342-1345. 39. Abdeljaber MH, Monto As, Tilden RL, Schork A. Tarwotjo I. The impact of vitamin A supplementation on morbidity: A randomized community intervention trial. Am. J. Public Health 1991;81:1654-1656. 40. West KP, Pokiel RP, Katy J, et al. Efficacy of vitamin A in reducing preschool child mortality in Nepal. Lancet 1991;338:67-71. 41. Ghana VAST study Team. Vitamin A supplementation in northern Ghana; effects on clinic attendances, hospital admissions, and child mortality. Lancet 1993;342:7-12. Nutritional and dietary risk factors of ALRI 37 ──────────────────────────────────────────────────────────── 42. Stansfield SK, Pierre-Louis M, Lerebours G, Augustin A. Vitamin A supplementation and increased prevalence of childhood diarrhea and acute respiratory infections. Lancet 1993; 341:578-82. 43. Bloem MW, Wedel M. Egger RJ, et al. Mild vitamin A deficiency and risk of respiratory tract diseases and diarrhoea in pre school and school children in north eastern Thailand. Am. J. Epidemiol. 1990;131:332-9. 44. Pinnock CB, Douglas RM and Badcock NR. Vitamins A status in children who are prone to respiratory tract infections. Aust. Paediatr. J. 1986;22:95-99. 45. Fawzi WW, Herrera MG, Willett WC, El Amin A. Nestel P. Lipsitz S. Spiegelman D and Mohamed KA, vitamin A supplementation and dietary vitamin A in relation to the risk of xerophthalmia. Am. J. Clin. Nutr. 1993;58:385-391. 46. West KP, Djundaedi E, Paudji A et. al. Vitamin A supplementation and growth: a randomized community trial. Am. J. Nutr. 1988;48: 157-64. 47. Muhilal PD, Idjradinata YR and Muherdiyantiningsih KD. Vitamins A- fortified monosodium glutamate and health, growth and survival of children: a controlled field trial. Am. J. Clin. Nutr. 1988:48:1271-76. 48. Scrimshaw NS. Ecological factors in nutritional disease. Am. J. Clin. Nutr. 1964;14:112-122. 49. LeRiche H, Kinnear AA and Smit RJ. The Diepkroof nutrition and health study on Bantu Boys, South Africa. Canad. Med. Ass. J. 1956;74:130-138. 50. Chandra RK Increased bacterial binding to respiratory epithelial cells in vitamin A deficiency. Br. Med.J 1988;297:834-35. 51. Lepage P, Munyakazi C and Hennart P. Breast-Feeding and hospital mortality in children in Rwanda. Lancet. August 22, 1981;II:409-411. 52. Victora CG, Barros FC, Vaughan JP and Reixeira AMB. Birthweight and infant mortality: a longitudinal study of 5914 Brazilian children. Int. J. Epidemiol. 1987;16:239-245. 53. Sauls HS. Potential effect of demographic and other variables in studies comparing morbidity of breast-fed and bottle-fed. Infants. Pediatrics 1979;64:523-527. 54. Bauchner H. Leventhal JR, Shapiro E. Studies of breast feeding and infection:how good is the evidence? J.A.M.A. 1986;256:887-92. 55. Ford K and Labbok M. Breast Feeding and child health in the United States. J. Biosoc. Sci 1993;25(2):187-94. 56. Hansen LÅ, Ashraf R, Zaman S, Karlberg J, Lindblad BS and Jalil F. Breast feeding is a natural contraceptive and prevents disease and death in infants, linking infant mortality and birth rates. Acta Paediatr. 1994;83:3-6. 57. Glazen WP. Epidemiological perspective of breast-feeding and acute respiratory illnesses in infants. Adv. Exp. Med. Biol. 1991;310:235-40. Original article The validity and reproducibility of a semiquantitative food frequency questionnaire used for measuring dietary vitamin A intake in under-five children in Addis Ababa, Ethiopia. Derege Kebede1, Melaku Umeta2, Elizabeth Wuhib2, Kelbessa Urga2 and Walter C Willett3 Summary: A valid assessment of diet is crucial both for understanding disease causation and for launching control programs. Although there have been a number of studies that have evaluated and demonstrated the reproducibility and validity of food frequency questionnaires (FFQs) in the developed world, to our knowledge there have not been published reports of such studies from Africa. The purpose of the present study was to assess the validity and reproducibility of a 98-item FFQ used in a cohort study to evaluate dietary vitamin A intake as a risk factor for acute lower respiratory infections in children under five years of age in Addis Ababa, Ethiopia. Serum retinol determinations and seven days of 24-hour diet recall were compared with data from the FFQ completed three times at six month intervals in a randomly chosen sub-sample of 100 children from the larger cohort. Reproducibility was high for all nutrients between the second and third FFQ. The correlations ranged from 0.36 for folic acid to 0.63 for preformed vitamin A. The correlations between FFQ1 and FFQ2 ranged from 0.23 for total vitamin A to 0.39 for preformed vitamin A. Correlations between the mean of the three questionnaires and serum retinol were 0.22 for intake of total vitamin A, 0.25 for preformed vitamin A and 0.15 for provitamin A. All nutrient estimations from the multiple recalls were not appreciably correlated with serum retinol levels. Correlations between the multiple 24-hour recalls were 0.21 for total vitamin A, 0.11 for preformed vitamin A, 0.16 for provitamin A, 0.12 for folic acid and 0.27 for total caloric intake. Our results suggest that 98-item FFQ performs reasonably well for categorizing children by levels of vitamin A intake in Addis Ababa. The results also indicate that the seven-day multiple 24-hour recalls were inferior to the questionnaires in estimating long-term vitamin A intake in children and are probably best avoided as gold standard measure in this setting.[Ethiop. J. Health Dev. 1997;0(0):39-46] Introduction Acute and chronic under nutrition and communicable diseases are major problems of developing countries(1). The interactions between nutrition and health have been recognized for some time(2). A reasonably valid assessment of diet is crucial both for understanding disease causation and for launching control programs(3). In the past decade, a large number of epidemiologic studies in the industrial world have used the semi-quantitative food frequency questionnaire (FFQ) for dietary assessment in their search for causes of diseases(4). The FFQ assesses the frequency of consumption during a specified time period with a list of foods using defined portions sizes. The strengths and ______________________________________ 1 From the Department of Community Health, Faculty of Medicine, P.O. Box 1176 Addis Ababa, Ethiopia, 2Ethiopian Health and Nutrition Research Institute, Addis Ababa Ethiopia and 3Departments of Nutritional and Epidemiology, Harvard School Public Health, 665 Huntington avenue, Boston, 02115, USA limitations of the FFQs have been reviewed(5,6). Short-term dietary assessment methods using the 39 ──────────────────────────────────────────────────────────── 24-hour recall or diet records, now less frequently used in the developed countries, are still widely used in developing countries including Ethiopia(7). Probably the two major advantages of use of the FFQs is that they measure the average long term diet (for example 6-12 months), which is more relevant for most disease causation than short term diet, and because they are relatively inexpensive and thus can be used for large scale epidemiologic studies6. Although there have been a number of studies which have evaluated and demonstrated the reproducibility and validity of FFQs in the developed world(8-11), to our knowledge there have not been published reports of such studies from Africa. Figure Time sequence of food frequency questionnaire (FFQ1-FFQ3) validation study using seven-day 24-hr recalls and serum retinol determination, conducted among 100 children under five years of age in Addis Ababa, Ethiopia 1993 1991 December FFQ1 1992 J F M A M June FFQ2 J A S ** (September) Sevenday multiple 24Recalls followed by Serum collection O November FFQ3 The purpose of the present study was to assess the validity and reproducibility of a 98-item FFQ used in a cohort study to evaluate dietary vitamin A intake as a risk factor for acute lower respiratory infections in children under five years of age in Addis Ababa, Ethiopia. Methods Population: Children in this study were a sample of a cohort of 1,992 children under five years of age participants of a cohort study, followed for one year, between November 1991 and December 1992, to study the risk factors for acute respiratory infections (Kebede and Willett. Submitted to Int.J.Epidemiol 1995). Dietary information was collected using food frequency questionnaires developed locally, three times during the year, at six-month intervals . The FFQ were administered by trained and supervised interviewers. Mothers or other caretakers were asked about their children's usual intake in the previous six months for each specific item and portion size, and were asked to respond in terms of frequency of intake per day, week, month, past 6 months or never. For the validation study we selected a random sample of 100 children from the cohort study and collected multiple 24-hour diet recalls for seven days followed by venous blood for serum retinol determinations. The blood collection and recall data were obtained close to the mid-interval (September) of time between the administration the second and third FFQs (Figure). After the conclusion of the recall interviews mothers were asked to bring their children to the clinical chemistry laboratory of a nearby referral and teaching hospital (Tikur Anbessa Hosptial) where an experienced laboratory technician drew their blood. Because of technical difficulties serum retinol determinations could be completed in only 80 of study children. Thus, comparisons between the dietary data and serum retinol levels were limited to the 80 study children who had both measurements. The semi-quantitative food frequency questionnaire: An experienced dietitian from the Ethiopian Nutrition Institute was invited to participate in the process of identifying the relevant food items to be included in the FFQ, with the aim of measuring intakes of total calories and vitamin A in Addis Ababa. Food composition tables for use in Ethiopia, East Africa and Africa(12-16) were consulted to work out an initial extensive food list of over 400 items. Of these 99 items deemed relevant and able to categorize children by past nutritional intake were selected. For each of the 99 food items listed, mothers were asked to estimate their children's use of that food in terms of a standard portion size. We have made this portion sizes to correspond to children's 'natural' units (for example, a quarter of Injera, the staple, but fairly large, flat bread). The list included mixed dishes as the number of such foods were not extensive in this population and food composition data on these foods were available. This FFQ was then pilot tested on 50 children under-five in a sub-district outside of the study area before it was 40 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── used in the cohort study. A computer program was developed to calculate nutrient values from the FFQ using Ethiopian and African food composition table data. Daily, weekly or monthly frequencies for each item in the FFQ were first converted into daily frequencies of consumption. These were multiplied by the specific food composition data base reflecting the nutrient content of one portion of each item in the questionnaire. The values were then summed up for all items in the FFQ giving total daily intake of the various nutrients for each child in the study. Multiple 24-hour recalls: Using a diet recall form developed for the purpose, trained and supervised field workers made visits to the selected households and interviewed caretakers on the child's diet intake during the previous 24-hours. This was repeated for seven consecutive days. For the 24-hour recalls, the dietitian from the Ethiopian Nutrition Institute calculated the nutrient values manually but following the same steps as described above for the FFQs. Serum retinol determination: Serum retinol determinations were conducted using high pressure liquid chromatography (HPLC) at the laboratory of the Ethiopian Nutrition Institute using the method described by Bieri et al(17). Blood was collected by venous puncture without anti coagulant and serum was separated and stored in the dark at -200C until analysis. Quantitation Retinol and retinyl acetate standards were prepared in absolute ethanol. Concentrations of the standard solutions were determined using a Beckman Du-60 (Irvine, CA, USA) spectrophotometer. The retinol concentration was computed from a standard curve of peak area ratios. To prepare a standard curve, we combined a constant amount of the internal standard with five different concentrations of retinol. These mixtures of retinol and retinyl acetate were chromatographed, and the peak area ratios (peak area retinol and retinyl acetate) and concentration ratios (concentration of retinol: concentration of retinyl acetate) were determined. The inter-assay coefficient of variation for retinol determination was 5.2%. Statistical analysis: Means and standard deviations were calculated on total nutrient intakes from the three FFQs and the recalls. Spearman's correlation coefficients were used in the statistical analysis. Correlations coefficients were computed before and after adjustment for total caloric intake: total caloric intake (loge transformed) was used as the independent variable in a regression model with the nutrient score (loge transformed) as the dependent variable. The rationale for energy-adjustment is given elsewhere(6), an additional reason was because we have used energy-adjusted nutrient estimates in evaluating dietary risk factors in the ALRI cohort study. Multivariate regression models were also fitted to evaluate the ability of the FFQs to predict serum retinol levels. Table 1: Age, sex and nutritional status of children under five years of age participating in the Addis Ababa validation sub-study and ALRI Study cohort, 1993 Variable Validation Study (n=100) % Total Cohort (n=1,992) % Age Under 6 months 5.0 5.5 6-12 months 8.0 9.0 13-24 months 9.0 19.0 >24 months 78.0 66.5 Sex Male Female Weight-for-height (wasting) 51.0 49.0 53.1 46.9 More than -2.0 Sda Between -2.0 and -3.0 Sd Less than -3.0 SD Height-for-age (stunting) 90.0 1.0 9.0 88.8 1.7 9.9 More than -2.0 SD Between -2.0 and -3.0 Sd Less than -3.0 SD 47.0 22.0 31.0 48.3 22.2 29.4 a Z scores were computed to categorize levels of weight-for-height, weight-for-age and height-for-age based on the NCHS standards. 41 ──────────────────────────────────────────────────────────── The ability of FFQs in discriminating children with serum retinol values of 10 mcg/dl or less was examined by dichotomizing serum retinol values into high and low (< 10 mcg/dl) and fitting a logistic regression model to the data, with serum retinol as the dependent variable. Odds ratios and 95% confidence intervals were then estimated. Test for trend was calculated by including the nutrient as continuous variables in the model. Table 2: Mean (+ standard deviation) absolute daily vitamin A intake estimated by three food frequency questionnaires (FFQ1-FFQ3), and seven days 24-hr recalls among 100 children under five of age in Addis Ababa, Ethiopia, 1993 Variable FFQ1 FFQ2 FFQ3 FFQ1-FFQ3a Recall ALRI Cohorta (n=1,992) Total vitamin A (RE/d) 409 + 285 556 + 259 556 + 259 469 + 204 389 + 203 444 + 238 Preformed vitamin A (RE/d) 27 + 47 28 + 40 28 + 49 28 + 36 6 + 24 33 + 43 Provitamin A (RE/d) 387 + 115 444 + 237 537 + 257 448 + 203 372 + 205 420 + 232 Folic acid (mcg/d) 191 + 111 188 + 92 212 + 140 191 + 82 176 + 167 173 + 90 Total caloric intake (kcal/d) 1495 + 667 1657 + 720 1720 + 844 1582 + 590 1096 + 274 1479 + 602 a Average intake estimated from all three FFQs Results for only the first FFQ and the mean of the first and second FFQs are presented because these were used in the ALRI cohort study. As the purpose of this report is to quantify measurement error rather than test hypothesis, p values for correlation coefficients are not presented. Data were entered onto a computer using the EPI-INFO program, version 5, CDC, Atlanta GA, and analyzed using the Statistical Analysis System program, version 6.04, SAS Institute, Cary NC. Scientific and ethical clearance for the study was given by the Research and Publication Committees of the Department of Community Health, the Faculty of Medicine, and the Research and Publication Office of Addis Ababa University. Results Age, sex, and the degrees of wasting and stunting among children participating in the validation study were comparable with these distributions in the overall cohort (Table 1). The proportion of children over 24 months of age was somewhat higher in the validation group than the larger cohort. We compared the means for average daily nutrient intakes from the seven days of multiple 24-hour recalls and from questionnaires 1 to 3 individually and in combination for the 100 children included in the validation study (Table 2). On the average, nutrient estimates from the three questionnaires were higher than those from recalls. This over estimation ranged between 4.8% for total vitamin A and 3.8% provitamin A for FFQ1 to 36% for total caloric intake with FFQ3. The mean intakes of all nutrients, except preformed vitamin A were slightly lower for the whole cohort (n = 1,992) compared with responses from questionnaire from the sample. This reduction varied between 2.3% for performed vitamin A and 8% for total caloric intake. The reproducibility of the FFQ was examined by calculating Spearman's correlations between the three FFQs completed at six-months intervals in one year (Table 3). Reproducibility was high for all nutrients when the second and third FFQ were compared. These ranged from 0.36 for folic acid to 0.63 for preformed vitamin A. Correlation coefficients, though, were lower with FFQ1. 42 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Table 3: Correlations (Spearman's coefficients) of food frequency questionnaires (FFQ1-FFQ3), completed three times at 6 months interval, among 1992 children under five years of age in Addis Ababa, Ethiopia, 1993 FFQ1 versus FFQ2 Variable Crude Adjusteda Total vitamin A 0.39 0.39 Provitamin A 0.29 0.14 Folic acid 0.30 0.17 Total caloric intake 0.29 a Intakes adjusted for total caloric intake using regression analysis Crude 0.39 0.22 0.20 0.18 FFQ1 versus FFQ3 Adjusted 0.38 0.04 0.16 - FFQ2 versus FFQ3 Crude 0.63 0.41 0.36 0.60 Adjusted 0.61 0.46 0.25 - The mean (+ SD) of serum retinol in the 80 children was 15.5 (+ 12.2) mcg/dl, and levels ranged between 6 and 64.1 with a median of 14.6 mcg/dl. Comparison of energy-adjusted nutrient intake measurements from the questionnaire with serum retinol values show the highest correlation for preformed vitamin A (r = 0.25) from the mean of all three questionnaires (Table 4). For preformed vitamin A correlations ranged between 0.09 for FFQ1 and 0.25 for the mean of all three questionnaires. For provitamin A these ranged between 0.06 for FFQ1 and 0.18 for the mean of FFQ2 and FFQ3. For total vitamin A the range was between 0.04 for FFQ1 and 0.22 for the mean of all three questionnaires. All nutrient estimations from the multiple recalls were not appreciably correlated with serum retinol levels. Table 4: Spearman correlation coefficients of vitamin A intake calculated from three food frequency questionnaires (FFQ1-FFQ3), and seven-day 24-hour recalls results with serum retinol determinations among 80 children under five years of age in Addis Ababa, Ethiopia, 1993 Total vitamin A Preformed vitamin A Pro vitamin A Crude Adjusteda Crude Adjusted Crude Adjusted FFQ1 0.11 0.04 0.10 0.09 0.13 0.06 FFQ2 0.07 0.12 0.16 0.20 0.09 0.12 FFQ3 0.07 0.12 0.17 0.10 0.05 0.11 Mean of FFQ1 & FFQ2 0.12 0.14 0.18 0.21 0.27 0.12 Mean of FFQ2 & FFQ3 0.09 0.19 0.25 0.22 0.09 0.18 Mean of FFQ1, FFQ2 & FFQ3 0.09 0.22 0.24 0.25 0.10 0.15 Seven 24-hr Recalls 0.05 0.04 0.08 0.03 0.02 0.02 a Intakes adjusted for total caloric intake using regression analysis The questionnaires were also compared with the multiple 24-recalls (Table 5). Correlation estimates were generally lower for total vitamin A. For preformed vitamin A the correlations ranged between 0.07 for FFQ2 to 0.27 for FFQ3, and for preformed vitamin A they ranged between 0.11 for FFQ2 and 0.22 for FFQ3. Adjustment for total energy intake decreased correlation coefficients. These were 0.21 for total, 0.11 for preformed, 0.16 for pro vitamin A, 0.12 for folic acid. The correlation was 0.27 for total caloric intake. The ability of the FFQs in discriminating children with low level of serum retinol (< 10 mcg/dl) was also examined (Table 6). There was a statistically significant association between dietary intake of preformed vitamin A levels and serum retinol levels. Children in the highest quintile of dietary preformed vitamin A intake had a 30% lower chance of having low levels of serum retinol compared to the children in the lowest quintile, FFQ1: (Adjusted RR: 0.70, 95% CI: 0.17, 2.84, P for trend:0.04); mean of FFQ1 and FFQ2: (Adjusted RR: 0.44, 95% CI: 0.11, 1.74, P for trend:0.003). Discussion We compared individual nutrient intakes estimated by a 98-item food frequency questionnaire completed three times in a year with serum retinol determinations and seven 24-hour diet recalls completed in the second half of the year. Correlations between serum retinol and the mean of the three questionnaire was 0.22 for total vitamin A, 0.25 for preformed vitamin A and 0.15 for provitamin A. Energy adjustment of nutrients improved correlations in the studies by Willett et al(8); the effect of adjustment by total caloric intake was minimal in the study by Pietinnen et al (1988). In our study such adjustment improved the correlation of nutrient estimates from the questionnaire with serum retinol value but attenuated those with multiple 24-hour recalls. The higher correlations with serum retinol after energy adjustment supports the biological rationale for this procedure(6), which is the primary reason for taking energy intake into account. 43 ──────────────────────────────────────────────────────────── Table 5: Spearman correlation coefficients for three food frequency questionnaires (FFQ1-FFQ3) and seven day 24-hr recalls among 100 children under-five years of age in Addis Ababa, Ethiopia, 1993. T otal vitamin A Preformed Vaitamin Provitamin A Folic acid Calories 24-Recalls Versus Crude Adj.a Crude Adj Crude Adj. Crude Adj Crude FFQ1 0.02 0.11 0.07 0.08 0.12 0.15 0.15 0.02 0.05 FFQ2 0.04 0.19 0.28 0.03 0.11 0.13 0.16 0.06 0.24 FFQ3 0.11 0.01 0.27 0.08 0.22 0.04 0.15 0.13 0.16 FFQ1&FFQ2 0.07 0.18 0.17 0.08 0.17 0.18 0.20 0.09 0.18 FFQ2 & FFQ3 0.11 0.18 0.26 0.08 0.17 0.08 0.25 0.13 0.27 FFQ1,FFQ2 & FFQ3 0.14 0.21 0.19 0.11 0.21 0.16 0.19 0.12 0.27 a Intakes adjusted for total caloric intake using regression analysis Table 6: Odds ratios (95% confidence interval) of low serum retinol level according to the distribution of nutrient intakes from food frequency questionnaires among 80 children under five years of age in Addis Ababa, Ethiopia. Dietary variable Quintile of intake P(trend)a FFQ1 1 2 3 4 5 Total vitamin A 1.00 0.73 (0.19, 2.77) 0.95 (0.25, 3.55) 1.14 (0.30, 4.33) 1.52 (0.40, 5.80) 0.6 Preformed vitamin A 1.00 0.46 (0.11, 1.81) 0.28 (0.07, 1.15) 0.38 (0.09, 1.49) 0.70 (0.17, 2.84) 0.04 Provitamin A 1.00 0.45 (0.11, 1.80) 0.93 (0.25, 3.51) 1.91 (0.47, 7.63) 1.56 (0.41, 5.96) 0.7 Mean of FFQ1 & FFQ2 Total vitamin A Preformed vitamin A Provitamin A 1.00 1.00 1.00 0.67 (0.22, 1.97) 0.73 (0.19, 2.81) 0.65 (0.18, 2.36) 0.35 (0.10, 1.17) 0.92 (0.23, 3.58) 0.71 (0.19, 2.57) 1.20 (0.36, 4.05) 0.64 (0.15, 2.65) 1.99 (0.52, 7.66) 1.02 (0.32, 3.22) 0.44 (0.11, 1.74) 1.26 (0.34, 4.59) 0.1 0.003 0.8 In well nourished populations the liver stores at least 90% of the total body reserve of vitamin A and buffers serum levels over a wide range of dietary vitamin A intake(9). On the other hand, serum retinol may be more sensitive indicator of vitamin A status in under nourished populations. Ethiopia is categorized globally among "category I" countries having physiologically significant vitamin A deficiency(19). Several surveys have also demonstrated this fact(7,20-22). The deficiency of the Ethiopian diet in protein, calorie and vitamin A was also shown by early studies(23-25). A survey of 31,876 children under six years of age in 1988 has shown a Bitot's spot rate of 0.6% in Addis Ababa(26). The present study was conducted in a population with low socio-economic status and poor nutritional status (Paper II). Thus, it is assumed that serum retinol values may be more sensitive indicator of prolonged low intake of vitamin A. Several studies from developing countries(27) and Ethiopia(28) have shown the association between intake of vitamin A and serum retinol levels. Our finding that nutrients estimated by questionnaire correlated with serum retinol levels, but not with multiple 24-hour recall, suggest that the questionnaire reflects vitamin A status of children than multiple 24-hour recalls. The availability and intake of food sources of vitamin A is affected by seasons in many countries particularly in Ethiopia due to agricultural practices(28) and the religious practice of fasting. Most of the 80% orthodox Christians fast between 150 and 200 days each year, and most of the Moslem population also fast for 30 days each year(29,30). Furthermore, unlike adults, as children grow, their dietary intake changes. This variation of intake of vitamin A will have impact on serum retinol levels. Also, the seasonal variation of dietary vitamin A intake is probably better measured by the three food frequency questionnaire which reflect longer period of intake (one to onehalf year), than the multiple 24-hour recalls which covered a period of only seven days. This is also indicated by the very low correlation between serum retinol levels and the multiple 24-hour recall in our study. The reproducibility of the FFQ was variable for total, preformed and provitamin A. This is probably due to the fact that the FFQs were reflecting in part a true variation in dietary intake among the study. For the orthodox christian population, fasting involves avoidance of meat and dairy products including eggs, and for the more conservative, fish. In this study fewer than 0.5 % of children were reported as having eaten fish during the study period. On the other hand, variations in the intake of vegetables, particularly food containing pepper (Capsicum anuum), which is widely and regularly eaten(28), may not be as marked as meat and dairy products. Our food frequency questionnaire was designed to be used in a cohort study of children under five years of age in Addis Ababa to evaluate the relationship of acute lower respiratory tract infections 44 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── (ALRI) and dietary vitamin A intake. Comparisons of children in extreme quintiles of distribution of dietary vitamin A intake were used to evaluate relative risks of ALRI (Paper II). Our data also provided the opportunity to compare the performances of both the food frequency questionnaire and diet recalls with serum retinol determinations. The results indicate that the seven day multiple 24-hour recalls were inferior to the questionnaires in estimating long-term vitamin A intake in children and probably best avoided as gold standard measures in this setting. The value of a greater number of 24-hour recalls or recalls more dispersed in time is unknown in the Ethiopian environment. In conclusion, we have found the 98-item food frequency questionnaire used in children under five years of age to be predictive of serum retinol levels among children in Addis Ababa. These result indicate that the food frequency questionnaire can be used to evaluate associations between dietary intake of vitamin A and risk of ALRI. Further research on the FFQs is required if they are to be use for estimation of other nutrients in children in Ethiopia. Acknowledgement This study was done as a doctoral thesis work by Dr. Derege Kebede at the Harvard School of Public Health. His training at Harvard was supported by a fellowship grant from the World Health Organization. The study was supported by a grant from the Rockefeller Foundation African Dissertation Internship Awards Program. Additional support was also obtained from the Departments of Epidemiology and Nutrition at Harvard and the Department of Community Health, Addis Ababa University. We thank the Ethiopian Nutrition Institute, particularly its Director: Dr. Zewdie WoldeGebriel for allowing use of the institute facilities for serum retinol determination. We would also like to acknowledge the mothers and other caretakers of study children, field workers, supervisors, clerical workers who have made the conduct and reporting of the study possible. We are grateful to Dr. Tigest Ketsela for her expert assistance during data collection, processing and analysis, and for reviewing an earlier draft of this manuscript. References 1. World Bank. World Development Report 1993: Investing in Health Oxford University Press, New York, 1993. 2. Scrimshaw NS. Ecological factors in nutritional disease. Am J Clin Nutr. 1964;14:112-122. 3. Stamler J. Assessing diets to improve world health: Nutritional research on disease causation in populations. Am J Clin Nutr: 1994;59(suppl):1465-565. 4. Willett WC, Future Directions in the Development of Food Frequency Questionnaires. Am. J. Clin. Nutr. 1994;59(supp):1715-45. 5. Block G. A Review of Validations of Dietary Assessment Methods Am J Epidemiol. 1982;115:492-505. 6. Willett WC. Nutritional Epidemiology. Oxford University Press, New York, 1990. 7. Bekele A. Wolde-Gebriel Z. and Kloos H. Food, diet, and nutrition. In:Kloos H and Zein ZA, eds. The ecology of health and disease in Ethiopia. Boulder: Westview press, Inc. 1993:85-102. 8. Willett WC, Sampson L, Stampfer MJ, Rosner B, Bain C, Witschi J, Hennekens CH. and Speizer FE. Reproducibility and Validity of a Semi-Quantitative Food Frequency Questionnaire. Am J Epidemiol. 1985;122:51-65. 9. Hunter DJ, Rimm EB and Sacks FM et al. Comparison of measures of fatty acid intake by subcutaneous fat aspirate, food frequency questionnaire, and diet records in a free-living population of US men. Am J Epidemiol. 1992;135:418-27. 10. Rimm EB, Giovannucci EL, Stampfer MJ, Colditz GA, Litin LB and Willett WC. Reproducibility and validity of an expanded self-administered semiquantitative food frequency questionnaire among male health professionals. Am J Epidemiol. 1992;135:1114-26. 11. Martin-Moreno JM, Boyle P, Gorgojo L, Malsonneuve P, Fernandez-Rodriguez JC, Salvini S and Willett WC. Development and validation of a food frequency questionnaire in Spain. Int J Epidemiol. 1993; 22(3): 512-519. 12. Ågren G and Gibson R. Food composition table for use in Ethiopia I. Addis Ababa: Ethiopian Nutrition Institute 1968. 13. Food and Agricultural Organization Food composition table for use in Africa Rome: Food and Agricultural Organization 1968. 14. Gobezie A. Manual for hospital diets for use in Ethiopia Addis Ababa: Ethiopian Nutrition Institute c1970. 15. Ethiopian Nutrition Institute Ethiopian Traditional Recipes Addis Ababa: Ethiopia Nutrition Institute 1980. 16. West CE, Pepping F and Temalilwa eds. The composition of foods commonly eaten in east Africa. Wageningen: Wageningen Agricultural University 1988. 17. Bieri JG, Tolliver TJ and Catignani GL. Simultaneous determination of alpha-tocopherol and retinol in plasma or red cells by high pressure liquid chromatography. Am J Clin Nutr. 1979;32:21439. 18. Pietinnen P, Harman AM, Haapa E et al. Reproducibility and validity of dietary assessment instruments. I. Self-administered food use questionnaire with a portion size picture booklet. Am J Epidemiol. 1988; 128:655-66. 19. Humphrey JH, KP West, Jr., & A Sommer. Vitamin A deficiency and attributable mortality among under 5 year olds. Bull WHO 1992;70(2):225-32. 20. Wolde Gebriel Z. Demeke T. and West CE. Xerophthalmia in Ethiopia: A nationwide ophthalmological, biochemical and anthropometric survey. European Journal of Clinical Nutrition 1991;45:469-78. 21. Lindtjorn B. Xerophthalmia in the Gardula area of South-West Ethiopia, Ethiop Med J. 1983;21:169-174. 22. DeSole G. Yigezu B. and Bekalu Z. Vitamin A deficiency in southern Ethiopia. Am J Clin Nutr. 1987;49:780-84. 23. Selinus R, Gobezie A, Knutsson E and Vahlquisr. Dietary studies in Ethiopia I. Dietary pattern among the rift valley Arsi Galla. Am J Clin Nut. 1971;a;24:365-77. 24. Selinus R, Awalom G And Gobezie A. Dietary studies in Ethiopia. II Dietary pattern in two rural communities N. Ethiopia. Act Soc Med Upsal 1971;b;76:17-38. 25. Selinus R, Gobezie A and Vahlquist. Dietary studies in Ethiopia 3 dietary pattern among the Sidamo ethnic group. A study of villages in the ensete mono culture area in Southern Ethiopia with special attention situation in young children. Act Soc Med Upsal. 1971;c;76:158-78. 26. Alemayehu W. and Cherinet A. Eye diseases and blindness In: Kloos H and Zein ZA, eds. The ecology of health and disease in Ethiopia Boulder: Westview press, Inc. 1993:237-50. 27. Patwardhan VN. Hypovitaminosis A and epidemiology of xerophthalmia. Am J Clin Nutr. 1969;1106-18. 28. Wolde-Gebriel Z. Micronutrient deficiencies in Ethiopia and their inter-relationships. [Dissertation]. Wageningen, the Netherlands: Wageningen University, 1992. 29. Knutsson KE, Selinus R. Fasting in Ethiopia. Am J Clin Nutr. 1970;23:956-9. 30. Pankhurst R. An Introduction to the medical history of Ethiopia. Trenton: Red Sea Press 1990. Review article Acute respiratory infections in rural Ethiopian children: Description of the study setting and review of the literature Lulu Muhe The study setting (Butajira district): Butajira is found in the southcentral part of the country on the western side of the Gurage chain of mountains. Two all-weather roads communicate Butajira with Addis Ababa, the shorter but rough road being 130 km away. The small town of Butajira used to act as a communication centre for traders coming from southern Ethiopia to the north, especially Addis Ababa and further to the Arab world and now it is the business centre and the seat of the district administration. It is famous for having a number of traders who have high business in the Markato area of Addis Ababa. In fact some farmers do half year trading in Addis Ababa and half year farming in their villages, thus the economic level of some farmers of this district is generally higher than most places in the country. The estimated population of the district was 250,000 and of Butajira town was 22,188. The Butajira district has altitude ranging from 1500 to 2300 metres above sea level. Traditional divisions of places according to altitude have implications in terms of life style, vegetation, crops, and disease pattern. They include "kola" meaning lowland and generally below 2000 metres, "Dega" or "woinadega" meaning highland or in between and generally above 2000 metres. People living in "kola" areas are said to have shorter life period, attacked by diseases especially malaria, tuberculosis and anaemia more commonly and eat food generally made of maize or sorghum. These divisions exist also in many parts of highland Ethiopia. _________________________________________ From the Ethio-Swedish Children's Hospital, Department of Paediatrics and Child Health, Addis Ababa, Ethiopia. Review of ARI Literature 47 ──────────────────────────────────────────────────────────── Figure 1: Map of Ethiopia and Butajira district indicating the ten selected areas The ethnic group in this region are the Gurages, who have further divisions into minor groups: Meskan, Marako, Silti, and sodo. The Gurages are said to have migrated from the north, a place called "Gura" in the region of Akale Guzai in Eritrea in the 12th century even though some said they came before the birth of Christ. The reason for this mass movement is said to be related to famine; some relate it to war. The language of the Gurages is semitic and is related to Tigrigna and Amharic. Further subdivisions into smaller groups gave different dialects as a result of much mixing. The Gurages are happy to live as Ethiopians, partly because they are successful business people even outside the Gurage areas. The main religion for the Gurages is Islam. But quite a high number also believe in Christianity. The names of the various subgroups and villages generally come from names of prominent people in the history of these people. Meskan tribe, the predominant subgroup in Butajira district, got its name because the people believe in "meskel yesus church", thus the name "Meskan" to the tribe. The People in Butajira district live by farming, trading and cattle grazing. Many people do both farming and petty trading. Farming is done based on the traditional ploughing system using oxen. The staple food for Gurages is "kocho" which is made from "ensete". Ensete is produced mainly in the highlands and it is a multi-purpose plant. They use the root to produce the food. The fibres from the leaves are used for producing containers, ropes and materials for building their houses etc. It may also be fed to their cattle. Kocho contains basically carbohydrates. It is usually eaten with butter and green leaves. Children who are marginally fed and put exclusively on kocho tend to develop kwashiorkor. Kocho, however, is popular because it is drought resistant and is not so much affected by lack of rain for one or two years because it normally is stored for several years. Rural houses are traditional round huts made of wood and plastered with clay, with thatched roofs, often with no windows or rather small windows. Only 4% of the houses were roofed with corrugated iron sheets in the rural areas. Most of the time there is only one room that is used for cooking food, sleeping of all household members, and keeping the cattle, sheep and goats at night. Water is generally obtained either from rivers or dug wells even though more recently some villages are getting their water from standpipes. The use of biomass fuel for cooking is universal. There is electricity in Butajira 48 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── town for lighting but few people use it for cooking. Illiterate mothers of Butajira, similar to other parts of the country, consider illness differently from the modern or western outlook. They are not familiar with the germ theory of causation of infectious diseases. They look at illnesses as results of evil spirits. The evil eye, the "bird of the sky" or Allah's will are common explanations for occurrence of disease in the child. Some common conditions like malnutrition may not be perceived as illnesses by mothers and who, therefore, do not seek care. Local terms of illness may not be congruent with terms for disease or symptoms as known by a health worker. Community's perception of illness can delay health care seeking for many diseases. For example, in measles, children suspected to have it will be kept at home, usually in the dark to protect them from "mich" (literally being hit) or "tilla" (literally shadow) or "buda" (evil eye) until the rash comes out. The child will be suffering from fever, dehydration and severe malnutrition including fatal complications. Many mothers may bring the child with measles to a health facility just to confirm the diagnosis. Despite different concepts of disease that we mentioned above, there are still good grounds in the culture of the Gurages that could be exploited and be used to increasing health awareness among the Butajira people and involving them into improvement of health facilities and health care development programmes. In the first place there are only one health centre (in Butajira town) and two health stations for a quarter of a million people. Even though more recently the staffing of the health centre has been improving, there are still resource constraints in terms of drug supply, reagents etc. There are two hospitals located 120 and 140 km south and west of the town respectively outside the district, to which patients could be referred. But obviously, many of the Butajira people cannot afford to pay the transport for such a long distance. Actually, for those living in remote areas, even the health centre is too far. With community involvement, a hospital is now being built in Butajira town now. Point of departure for the ARI studies in the area: Experience within the Butajira Rural Health Project proved that the Butajira people are unique in their friendly outlook, acceptance of new ideas and remarkable cooperation for health studies. Thus, once the surveillance system was established in 1987, studies were being done quite smoothly and results were coming. It was shown that the crude death rate was 16.4 per 1000 population. 26% of the deaths were infant deaths and 24 % were child deaths (10). The age-specific mortality pattern displayed the well-known U-shaped curve. The infant mortality rate was 109/1000 live-births (120 for boys and 98 for girls). The rate of dying between 1-4 years was 36.0/1000 children per year for the sexes combined. Cumulative under-five (0-4 years) mortality rate i.e. the probability of dying before the age of five years, was 210/1000 children (10). As the aims of the surveillance system was to prepare a framework for health related research, a number of health issues were planned. Because the underfive mortality accounted for more than half of all deaths in the community, but only 18% of the population being underfive, searching for determinants of mortality in this age group seemed mandatory. The research team both from hospital experiences and the increasing global awareness of ARI as a public health problem at that stage wanted to look at the role of ARI in this high underfive mortality. Review of the literature on epidemiology of ARI Impact of ARI in global mortality and morbidity in children: In developed countries, during the last hundred years, the decline of mortality due to acute respiratory infections (ARI) has been dramatic (1). At high levels of mortality, such as in XIXth century Europe, diseases due to ARI reduced life expectancy with 7.5 years, more than all other infectious diseases (4.8 years) including diarrhoeal diseases (2.9 years). Among infants and children, ARI was the first cause of death outside the neonatal period. When life expectancy was below 45 years, 25% of all deaths in the age group 0-4 years were due to ARI, compared to only 4% when life expectancy increased to 70 years. Thus, ARI mortality has been declining steadily with improving living conditions in developed countries, a decline that has been enhanced 1950 when antibiotics became available. Perhaps the best way to estimate the current Review of ARI Literature 49 ──────────────────────────────────────────────────────────── burden of ARI diseases in developing countries is to compare ARI mortality to the lowest values recorded in developed countries. This would indicate the number of deaths that could be averted if improvements could be made in living conditions, health service coverage including availability of antibiotics. Such a comparison and the high values of ARI mortality found in many developing countries indicate that more efforts should be made to control ARI (1). In developing countries every 7 seconds a child under five years of age dies because of acute respiratory infections, usually pneumonia (2). Of the 12.9 million deaths of children under five that occurred in 1990, some 4.3 million were attributed to ARI (3), accounting for 33% of all deaths in childhood and the overwhelming majority occurring in developing countries. Other data show that ARI is also the leading contributor to the loss of disability-adjusted life years (DALYs) in children under five years of age (4). The latter takes into account the serious chronic sequelae of pneumonia and otitis media, the leading preventable cause of deafness. However, recognition of pneumonia and other ARI as an important public health problem in developing countries is recent; the earliest documentations being in the early 1960s (5). Part of the high death toll seen in developed countries in the XIXth century could be accounted explained by the simple fact that antibiotics were not available. The large difference in the ARI-related mortality in children between developed and developing countries is progressively increasing mainly because the number of child deaths in the developed countries is being lowered faster than in the developing countries (6). The high ARI-related mortality in developing countries seen at a time when antibiotics are available should not wait until socio-economic development is achieved. The problem should be tackled by increasing understanding of the impact of environmental, social and health factors to ARI death in a community and instituting a locally effective, appropriate, community-specific control method(s). In addition to mortality studies, evaluations of magnitude and pattern of morbidity underlying mortality are necessary to assess the health needs of children in a social, economic, and health services context. Statistical information about the incidence of acute respiratory infections in the general population is scarce, since most respiratory infections are not listed among the diseases that must be notified to health statistics departments. The limited data from community-based longitudinal studies indicate that they are very common. On average, a child seen in urban areas has from five to eight episodes of respiratory disease annually during the first five years of life. It has been found that the same incidence range was observed in towns of Costa Rica (7), Ethiopia (8), Kenya (9) and India (10), as in towns of the United states (11,12). The available data suggest that even the mean duration varies little, amounting to seven to nine days with one or more respiratory symptoms per episode. The difference in disease experience seems to lie in the incidence and severity of acute lower respiratory infections, in particular pneumonia (6). Risk factors in ARI: Mortality from ARI declined in Europe and North America in the first half of the century before any specific preventive or therapeutic interventions were introduced. This is probably due to the gradual improvement in socio-economic conditions. Surveys in the industrialized countries have shown that exposure to adverse social conditions increases the probability of lower acute respiratory infections in early childhood. The standard of living in rural and periurban areas of developing countries is associated with host and environmental factors which increase the risks of severe respiratory infections in children (13). The birth weight of an infant is said to be the most important determinant of its chances of survival and healthy growth and development (14). It has, indeed, been used as an indicator of social development (15). Low birth weight (LBW) prevalence is high in developing countries, 20-40% versus 5-7% in developed countries and is frequently not due to prematurity but foetal growth retardation. LBW infants have higher IMR and pneumonia is the commonest cause of death from infection among LBW infants (16). Infection and disease impair the nutrition process. When food is scarce, malnutrition is aggravated 50 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── and the undernourished are more susceptible to infection. Thus a vicious circle is formed with infection affecting food intake and protein metabolism (17-21) and malnutrition acting as risk factor to infection (22-23). It has been estimated that some 40% of the total childhood population in the underdeveloped world is suffering from malnutrition, the major forms being protein-energy malnutrition, hypovitaminosis A, anemia and rickets (7). It has been suggested that malnourished children tend to have more frequent and prolonged episodes of ARI. Studies in developing countries indicate that breast feeding protects against severe respiratory infections (24-25). Studies in the developed world also showed the protective effect of human milk. In a suburban area of London, the annual incidence of bronchitis and pneumonia was significantly less common in infants who were breast-fed than in those who were formula-fed (26). In a case control study in Newcastle Upon Tyne, England, breast feeding appeared to halve the risk of admission to hospital with respiratory syncytial virus infection in children 0-5 months of age (27). Of nutrient deficiencies that may contribute to risk of infections in childhood, hypovitaminosis A is the most studied. Even though it has been reported that the intestinal absorption of vitamin A in children with ARI or diarrhoea was significantly lower than that of normal children (28), that vitamin A is important in maintaining the integrity of mucosal surfaces (29), as well as in ensuring competent cell-mediated immune responses (30) has suggested its potential protective effect against ARI. Vitamin A supplementation reduced measles morbidity, in particular pneumonia morbidity following measles by as much as 61-82% using the WHO-recommended dose (31). Others have shown that vitamin A deficiency is associated with a threefold increase in ARI morbidity (32-33). Vitamin A supplementation has been reported to reduce childhood ARI mortality (34) as well as ARI morbidity, even in well-nourished Australian children (35). A recently completed study in northern Ghana indicated no impact of vitamin A supplementation on the prevalence of childhood infections but showed a significant reduction in the "severity" of diarrhoea (36). Other studies suggested that vitamin A supplementation increased morbidity to a significant extent (37-40). A meta- analytical study showed an overall significant reduction in mortality based on 20 controlled studies but few data to conclude about morbidity (41). The role of vitamin A supplementation as a preventive measure to ARI morbidity awaits further studies. Vitamin D deficiency rickets is another still common condition that is reported to be associated with increased morbidity especially due to ARI (42-44). Large amounts of data have been collected on outdoor air pollution which is associated with urban combustion of fossil fuels. Conversely little attention have been given to indoor air pollution in rural communities of the developing world where biomass fuel is the principal source of energy. Young children often accompany their mothers during cooking, and important exposures to pollution from biomass fuels can occur at these times. Furthermore, at night, and during cold seasons in highland communities, families often spend many hours sleeping in heavily polluted rooms. In most countries using biomass fuels, the IMR and the incidence of pneumonia in young children is very high. The question has therefore arisen as to whether indoor air pollution is a major causal factor in childhood pneumonia. Four published studies have pointed to this association, even though none of them were conclusive because of the design used in data collection (45-50). An epidemiological survey conducted in Papua New Guinea showed there was no significant damaging effect of indoor air pollution on the respiratory tract of school children living in the highlands (51). This study did not include young infants and the sample size was small. More studies are required before the full implication of indoor exposure to smoke particles is known and its effect on children's health is more precisely determined. Microbiological Etiology of ARI: Viruses are the predominant etiological agents in ARI, especially URTI. The majority of these illnesses are benign and self-limiting. The most frequent non-bacterial agents of lower respiratory illnesses in infants and young children are respiratory syncytial virus (RSV), adenoviruses, parainfluenza and influenza A and B viruses. More frequently some agents are more associated with some clinical syndromes than others e.g. RSV with bronchiolitis. In a significant fraction of the cases, viral infection is the cause of a severe disease which can end in death (52) or is Review of ARI Literature 51 ──────────────────────────────────────────────────────────── complicated by bacterial superinfection. It is well known that secondary bacterial infection of the respiratory tract is the most frequent complication of influenza and measles infection, also recognized for rhinoviruses (53) and adenoviruses (54). The virus infections seem to act as suppressor of the normal respiratory antibacterial defence by impairing the muco-ciliary clearance and altering the functions of neutrophils, alveolar macrophages and T-lymphocytes. Among the bacteria, Streptococcus pneumoniae, Haemophilus influenzae are the two commonest organisms. Staphylococcal pneumonia also predominates in the 1-6 month old age group. Among neonates, gram negative enteric bacilli most notably E.coli and streptococcus group B are said to be dominant in the developed world. The few studies done in developing countries do not support streptococcus group B being an important pathogen in neonates (55-56). Since pneumonia can be caused by a variety of organisms, the ideal approach to its management would be to identify the causative agent(s) in each individual case so that an appropriate antibiotic can be prescribed. However, an etiological diagnosis of pneumonia is very difficult to establish in infants and young children because sputum is usually not available. A bacterial cause of pneumonia in young children can only be established by lung (or pleural fluid) aspiration or blood culture. Rapid immunological techniques such as an enzyme-linked immunosorbent assay (ELISA), latex particle agglutination, or coagglutination do not yet perform adequately for reliable bacteriological diagnosis in children. Blood cultures are positive in only a portion of children with bacterial pneumonia. In five recent hospital based studies in Bangladesh, Brazil, Pakistan, Papua New Guinea, and the Philippines, bacteria were isolated from the blood cultures of 17-27% of children with severe pneumonia (57-59). While cultures of lung aspirates yield a very low false-positive rate ( a positive result is strong evidence of bacterial infection), lung puncture is an invasive procedure and there is a small risk of serious complications associated with its use. During the last 20 years it has been used in 12 studies in developing countries in children with pneumonia who had not received previous antibiotic treatment(58-60). When the results of these studies were pooled, bacteria were isolated from 453 (56%) of the 808 children examined; they were found in at least 50% of the children in all but two small studies. In fact, a proportion of the negative results were probably false-negatives, because of factors that mask the presence of bacteria. For example, the appropriate lung lesion may not be reached with the needle, the material collected may be scanty, or the laboratory methods may be inadequate to isolate all bacterial pathogens. Thus, the actual proportion of positive cultures was probably higher than that reported. These studies also demonstrate that S. pneumoniae and H. influenzae were the most frequently isolated bacteria, being identified in 70 - 80% of the culture positive cases. Staphylococcus aureus causes a small proportion of pneumonia in untreated children, and a high proportion when the children studied have already had antibiotic treatment, or have hospital rather than communityacquired pneumonia. Clinical and radiological criteria are unreliable means of determining the etiology of childhood pneumonias. An etiological agent can be established in less than one-quarter of children hospitalized with pneumonia in developed countries, despite full diagnostic facilities, and in an even smaller proportion of ambulatory cases. As a result of these diagnostic limitations, the institution of empirical antibiotic therapy for pneumonia is the commonly accepted practice worldwide. In developing countries, and especially in those with high infant mortality rates (IMR), as many as half of the pneumonia cases in children attending health services may be of bacterial origin. Because of the higher probability of bacterial pneumonia, there is an even stronger justification for the empirical use of antibiotics than in developed countries. The prevalence of bacterial infections may be favoured by malnutrition, insufficient coverage of immunization, low level of education, poor hygienic habits, primitive sanitary conditions and lack of early health care or of any health care at all. Two kinds of data may be important in support of the high prevalence of bacterial respiratory infections in children of developing countries: etiological investigations of pneumonia and the pattern of colonization and 52 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── carriage of potentially pathogenic bacteria in the upper respiratory tract. Approaches to ARI management and control: Health-care workers treating children in developing countries often have to make treatment decisions without the aid of confirmatory laboratory tests. To help in such decisions the World Health organization has developed and promoted assessment and treatment algorithms based on clinical signs for several major childhood diseases (61), including ARI (62). The latter case management protocol aims at distinguishing cases of pneumonia from other cases of acute respiratory infection and providing appropriate treatment. For simplicity and ease of training, the smallest number of criteria that is adequate to diagnose cases of pneumonia is used. In addition to recognition and treatment of pneumonia, the case management addresses home management issues extensively and health education to promote vaccination and early seeking of health care. It is to be noted that four of the six Expanded Programme for Immunization (EPI) targets i.e. measles, pertussis, diphtheria and tuberculosis give ARI-related diseases. Almost all cases of pneumonia can be detected by simple clinical signs, without radiography or laboratory data. The pathognomonic value of a cluster of simple clinical signs for the diagnosis of pneumonia has been shown by studies in the Gambia (63), Lesotho (64), Papua New Guinea (65), and India (66). For example, fast breathing was found to be a better predictor of pneumonia than auscultatory findings (67). All these studies confirmed that fast breathing is a sensitive and specific indicator of the presence of pneumonia, and that observation of this sign can help to categorize children with cough into two groups with high and low probability of pneumonia. They have also provided detailed information on the sensitivities and specificities of different respiratory rate criteria in different age groups. The sensitivity of these clinical signs as observed by trained lay reporters in different settings versus clinical diagnosis by physicians may however need to be further evaluated. Community based focused ethnographic studies of ARI in particular pneumonia are needed to provide data on community beliefs about ARI in children, including their causes and treatment. There is a particular need for documentation of the terms, signs and symptoms by which families recognize illness that corresponds, in whole or in part, to clinically diagnosed pneumonia. Appropriate case management can avert most deaths from ARI, but only if families recognize signs of possible pneumonia and seek care promptly from a trained health worker. Identification of the factors that facilitate or constrain prompt seeking of care from a trained health worker is very much needed. In view of the cultural variability associated with maternal recognition and interpretation of signs and symptoms of pneumonia, a direct translation of these signs and symptoms into a local language may not always be appropriate. Thus, studies are needed to assess whether instructions given to mothers for careseeking are appropriate for mothers in a specific community. Other cultural characteristics and conditions that are likely to strongly influence community responses to ARI programme activities should also be identified. Modules have been prepared by WHO's ARI control programme to teach physicians, nurses and auxiliary health workers on the case management based on the above principles. Thus in a child aged 2 to 12 months with a respiratory rate more than 50 or age above one year and respiratory rate above 40 per minute and no chest indrawing presenting with cough or difficult breathing pneumonia is diagnosed and child is treated with antibiotics for 5 days. Reassessment is done in 2 days. Home care advice is given. ARI in the Ethiopian Perspective: Information on the contribution of ARI to the high IMR and preschool child mortality rate in Ethiopia is limited to hospital and a few community-based surveys. Diseases of the respiratory tract were the principal diagnoses in 11% of 3500 admissions to a children's hospital in Addis Ababa (68). Cases with pneumonia as the principal diagnosis constituted 6% of admissions and accounted for 7% of the deaths. Measles was the principal diagnosis in 3% of the admissions with a case fatality rate of 28%. Among 21,853 ambulatory patients in the same hospital over a year, ARI was the principal health problem in 20% (69). In a report from a clinic serving a deprived area of Addis Ababa, ARI accounted for 35% of the 25,000 annual child attendances (70). Review of ARI Literature 53 ──────────────────────────────────────────────────────────── The scarce data available have come from urban communities. In the face of the fact that 85% of the population of Ethiopia is rural (71), it can be concluded that the problem of ARI in terms of morbidity or even mortality has not been sufficiently described to health planners. In view of the large population and the large size of the country, the infrastructure for health services and health care is very much limited as well as underutilized. In a study conducted within the BRHP (72), it was shown that the prevalence of perceived illness was 15% during a recall period of 2 weeks and only one third of those who reported illness had visited a health unit. The study showed that people in Butajira town used the health service seven times as much as the peasant population emphasizing the inequities and discrepancy that exist also at district level for the limited services available. Similar results were reported in studies from the Rift valley (73), from the eastern (74) and northern (75) parts of the country. Obviously the poor health services and the low utilization by the more vulnerable groups increase the risk of death from ARI and other diseases. The magnitude of the potential impact of nutritional factors on ARI outcome in Ethiopia is underscored by the observation that up to 50% of rural children are undernourished (76). The decline in breast feeding in many communities (77) may have increased the seriousness of the ARI problem. Ethiopia was one of the nine countries which participated in the WHO collaborative breast-feeding survey conducted in 1976-77. This survey was undertaken on three different socio-economic groups of mothers and their children: the urban rich, the urban poor and the rural. The results show that 8.6% of the urban rich and 2.7% of the urban poor had not initiated breast feeding at all, whereas all mothers in the rural areas had initiated breast feeding (78). A more recent study from western Ethiopia reported that exclusive breast-feeding (without supplementation) declined from 86% for infants 2 months of age to 31% in infants 4-6 months (79), indicating that weaning takes place relatively early in some populations. A national breast feeding survey on knowledge, attitude and practices among mothers and health professionals concluded that health services frequently contribute to the decline of breast feeding either by failing to support and encourage mothers to breast feed or by introducing routines and procedures that may interfere with the normal initiation and establishment of breast feeding particularly in urban areas (80). Thus, with decline in breast feeding, increased ARI mortality and morbidity is likely, although it has not been addressed by special studies. The role of vitamin A deficiency states in childhood disease and mortality is increasingly being recognized in Ethiopia. Hospital based studies showed that 36% of outpatients of 2 hospitals in Addis Ababa from 1976 to 1980 were identified as having the deficiency state (81). Very high rates of clinical xerophthalmia (up to 7.2%) in monocrop agriculture areas were also reported (82) by Desole in 1987. Vitamin A deficiency attains public health importance also among pregnant women as shown by GebreMedhin et al comparing Ethiopian mothers with Swedish mothers (83). The 1979-81 national nutritional survey by ENI among 6,636 preschool children in the four major agricultural ecozones also found an association between avitaminosis and diet; the highest rates of vitamin A deficiency were again in the grain-growing areas (6.6%) and the lowest rates were in the ensete areas (1.0%)(84). Severe rickets , which is no longer seen in developed countries, is common in developing countries in the tropics and subtropics, in spite of abundant sunshine (85-87). In Ethiopia, severe rickets gives considerable morbidity and mortality from chronic pulmonary fibrosis and terminal cor pulmonale in the advanced disease (87). A case control study showed that rickets is associated with severe malnutrition (73%) and Pneumonia (62%) and mortality in these patients is 31% (88). A preliminary case-control study from the Ethio-Swedish Children's Hospital showed that mortality from pneumonia is 3 times more common when there is associated rickets in the child (89). Birth weight is recognized not only as a reliable index of intrauterine growth but also as a pertinent risk factor limiting the probability of infant survival and normal development (90). In Ethiopia, limited information on birth weight distribution is available mainly for the cities of Addis Ababa and Gonder (91-92). The mean birth weight for Addis hospitals were reported to be 3100 and the low birth weight 54 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── rate was 13%. The mean birth weight for Jimma was 3180 grams and the incidence of LBW was 12.3% (93). The source of these data are all from hospital records which tends to have a selection bias because only certain individuals may be using the hospitals and thus the results are not generalizable. Other limitations of such data are the lack of accuracy and completeness of the records. Cigarette smoking has been uncommon in Ethiopians until the present generation, but has lately become more widespread, for example, among medical students (94) and high school students (95). In contrast, indoor air pollution from biomass fuel has been a way of life for centuries. All households in rural Ethiopia and most households in urban areas still use biomass fuel for cooking food and lighting the house at night and possibly heating rooms at cold hours. As in many developing countries, guidelines on pneumonia case detection by clinical signs and symptoms are being adapted to local conditions within the Ministry of Health of Ethiopia. A draft policy on ARI National Programme has come out as recently as January 1993 (96). The programme has given a number of training workshops on the case management of ARI. Much is expected to see impact on the control of ARI in the country. However, such case management guidelines require field testing and adapting to the local circumstances. For example, the management module needed translation to the local languages. While the latter is already done for Amharic, it is awaiting evaluation of the performance in training as well as clinical management. As the infrastructure of health services is still low in many places, training of community health agents using a more simplified module is invisaged to be ideal. There are very few studies in Ethiopia that addresses communities beliefs and practices in the care of children with pneumonia. A small study on the northern periurban Oromo community of Addis showed that it is possible to change mothers attitude and practice by repeated general and ARI-specific health education (97). The health goals of the plan of action of the World Summit for Children, held in New York in 1990 included " a reduction by one-third in child deaths caused by acute respiratory infections" by 2000 (4). Is this goal likely to be realized in Ethiopia? Any such discussion of health actions, programmes or policies must start with a sense of the scale of health problems. It is conceivable that ARI contributes to much of the high IMR in this country. How much and what factors are responsible for ARI deaths? What amount of the disease burden and death can be averted by responding to these questions by appropriate interventions ? Such questions should guide future priority research areas in Ethiopia. References 1. Preston SH. Mortality patterns in national populations. ed.New York: Academic Press, 1976. 2. Gwatkin DR. How many die? A set of demographic estimates of the annual number of infant and child deaths in the world. Am J Public Health 1980;70:1286-9. 3. World Health Organization. Sixth Programme Report 1992-93. Programme for the control of Acute respiratory infections. Document WHO/ARI/94.33. Geneva: World Health Organization,1994. 4. World Development Report 1993. Investing in health. Published for the World Bank. Oxford: Oxford University Press, 1993. 5. Gordon JE. et al. Death rates and causes of death in eleven Punjab villages: an epidemiological study. Indian journal of medical research. 1961; 49:568-594. 6. Pio A, Leowski J, & Ten Dam HG. The magnitude of the problem of acute respiratory infections. ARI in Childhood. Proceedings of an international workshop, Sydney, August 1984: 3-16. 7. James JW. Longitudinal studyof the morbidity of diarrhoeal and respiratory infections in malnourished children. Am J. Clin nutr 1972;25:690-94. 8. Freij L, Wall S. Exploring child health and its ecology. The Kirkos study in Addis Ababa. Acta Paed Scand, 1977. Suppl.267. 9. Wafula EM, Onyango FE, Mirza,WM, Macharia,WM et al. Epidemiology of acute respiratory infections among young children in Kenya. Review of Infectious Diseases. 1990;12:S1035-S1038. 10. Kammath KR, Feldman RA, Sundar Rao, PSS, and Webb JKG. Infection and disease in a group of Review of ARI Literature 55 ──────────────────────────────────────────────────────────── south indian families and family members. Am J Epid 1969;89:375. 11. Monto AS, Ullman B. Acute respiratory illness in an American community: The Tucumsch study. JAMA 1974;227:164. 12. Fox JP, Cooney MK, Hall CE. The Seattle Virus Watch:V. Epidemiologic observations of rhinovirus infections, 1965-1969, in families with young children. Am J Epid 1975;101:122. 13. Parker RL. Acute respiratory illness in children: PHC responses. Health policy and planning 1987;2(4):279-88. 14. World Health Organization. Weekly Epidemiological Record,1984;59:205. 15. Sterky G, Mellander L. Birth weight distribution - an indicator of social development. Report from SAREC/WHO workshop. SAREC Report series No R:2,1978. 16. Crosse, VM. The Preterm Baby. ed. London:Churchill Livingstone, 1975. 17. Mata LJ, Kromal RA, Urrutia JJ, Garcia B. Effect of infection on food intake and the nutritional state:perspectives as viewed from the village. Am J Clin Nutr 1977;30:1215-27. 18. Martorell R, Yarbrough C, Yarbrough S, Klein RE. The impact of ordinary illnesses on the dietary intakes of malnourished children. Am J Clin Nutr 1980;33:345-50. 19. Brown KH, Black RE, Robertson AD, Becker S. Effects of season and illness on the dietary intake of weanlings during longitudinal studies in rural Bangladesh. Am J Clin Nutr 1985;41:343-55. 20. Tomkins AM, Garlick PJ, Schfield WN, Waterloo JC. The combined effects of infection and malnutrition on protein metabolism in children. Clin Sci 1983;65:313-24. 21. Briscoe J. The quantitative effect of infection on the use of food by young children in poor countries. Am J Clin Nutr 1979;32:648-73. 22. Brown KH, Gilman RH, Gaffar A, Alamgir SM, Strife J, Kapikian AZ, Sack RB. Infections associated with severe protein calorie malnutrition in hospitalized infants and children. Nutr Res 1981;1:33-46. 23. Graitcer Pl, Gentry EM, Nichaman MZ, Lane JM. Anthropometric indicators of nutrition status and morbidity. J Trop Paediatr 1981;27:292-298. 24. Jelliffe DB, Jelliffe EFP. Human milk in the modern world. ed. Oxford, Oxford University Press,1980. 25. Lepage P, Munyakazi C, Hennart P. Breastfeeding and hospital mortality in children in Rwanda. Lancet 1981; August 22:409-11. 26. Watkins CJ, Leeder SR, Corkhill RT. The relationship between breast and bottle feeding and respiratory illness in the first year of life. J epid comm Health, 1979;33:180-82. 27. Pullan CR, Toms Gl, Martin AJ, Gardner PS, Webb JKG, Appleton DR. Breast-feeding and respiratory syncitial virus infection. BMJ 1980;281:1034-36. 28. Siva Kumar B, Reddy V. Absorption of labelled vitamin A in children during infection. Br J Nutr 1972;27:299-304. 29. Bendich A. Physiological role of antioxidants in the immune system. J Diar Sci 1993 Sep;76(9):2789-94. 30. Chandra RK. Cell-mediated immunity in nutritional imbalance. Fed Proc.1980;39:3088-92. 31. Coutsoudis A, Broughton M, Coovadia HM. Vitamin A supplementation reduces measles morbidity in young African children: a randomized, placebo-controlled, double-blind trial. Am J Clin Nutr 1991 Nov;54(5):890-5. 32. Sommer A, Katz J, Tarwotjoi. Increased risk of respiratory disease and diarrhoea in children with preexisting mild vitamin A deficiency. Am J Clin Nutr 1984;40:1090-95. 33. Sommer A,Tarwotjoi, Djunaedi E, et al Impact of vitamin A supplementation on childhood mortality. Lancet 1986;1:1169-73. 34. Sommer A, Tarwotjoi, Hussaini,G, Susanto D. Increased mortality in children with mild vitamin A deficiency. Lancet 1983;ii:585-8. 35. Pinnock CB, Douglas RM, Badcock NR. Vitamin A status in children who are prone to respiratory 56 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── tract infections. Aust Paediatr J 1986;22:95-9. 36. Arthur P. Kirkwood B, Ross D, et al. Impact of vitamin A supplementation on childhood morbidity in northern Ghana. Lancet 1992;339:361-62. 37. Stansfield SK, Pierre-Louis M, Lerebours G, Augustin A. Vitamin A supplementation and increased prevalence of childhood diarrhoea and acute respiratory infections. Lancet 1993;341:578-82. 38. Rahmathullah L, Underwood BA, Thulasiraj RD, Milton RC. Diarrhoea, respiratory infections and growth are not affected by a weekly low-dose vitamin A supplement: a masked, controlled field trial in children in southern India. Am J Clin Nutr 1991;54:568-77. 39. Bandrinath P, Chaladar BK, Rao TSK. Effect of massive doses of vitamin A on morbidity and mortality in Indian children. Lanct 1991;29:849-50. 40. Kartasasmita CB, Rosmayndi O, Soemantri ES, Deville W, Demedts M. Vitamin A and acute respiratory infections. Paediatr Indones 1991;31:41-49. 41. Glasziou PP, Macherras DE. Vitamin A supplementation in infectious diseases: a meta analysis. BMJ 1993 Feb 6;306(6874):366-70. 42. Nagi NA. Vitamin D deficient rickets in malnourished children. J trop med hyg 1972;75:251-54. 43. Salimpour R. Rickets in Teheran. Arch Dis child 1975;50:63-5. 44. Zaman S, Jalil F, Karlberg J, Hanson A. Early child health in Lahore, Pakistan:VI. Morbidity. Acta Paedi%' (+ ( 1993 Aug;82 suppl 390:63-78. 45. Kossove D. Smoke-filled rooms and lower respiratory disease in infants. South Afr Med J 1982;24 April:622-24. 46. Armstrong JRM, Campbell H. Indoor air pollution exposure and lower respiratory infections in young Gambian children. Int J Epidemiol 1991;20:424-29. 47. Campbell H, Armstrong JRM, Byass P. Indoor air pollution in developing countries and acute respiratory infections in children. Lancet 1989;i:1012. 48. Collings DA, Sithole SD, Martin KS. Indoor woodsmoke pollution causing lower respiratory disease in children. Trop doct 1990;20:151-5. 49. Pandey MR, Neupane RP, Gautam A, Shrestha IB. Domestic smoke pollution and acute respiratory infections in a rural community in the hill region of Nepal. Env Internat 1989; 15:337-40. 50. Pandey MR, Boleij JSM, Smith KR, Wafula AM. Indoor air pollution in developing countries and acute respiratory infection in children. Lancet 1989;i:427-428. 51. Anderson HR. Chronic lung disease in the Papua New Guinea Highlands. Thorax 1979;34:647653.? Inter J Epidem,1978. 52. Downham MP, Gardner PS, McQuillin J, Ferris JAJ. Role of respiratory viruses in childhood mortality. BMJ 1975;1 February:235-39. 53. Cherry JD, Diddams JA, Dick EC. Rhinovirus infections in hospitalized children. Arch environm health, 1967;14:389-96. 54. Ellenbogen C, Graybill JR, Silva J, Homme PJ. Bacterial pneumonia complicating adenoviral pneumonia. A comparison of respiratory tract bacterial culture sources and effectiveness of chemoprophylaxis against bacterial pneumonia. Am J Med 1974;56:169-78. 55. Tafari N and Ljungh-Wadstrom A. Consquences of amniotic fluid infection: early neonatal septicaemia. Excerpta medica 1980, Perinatal infections ( Ciba foundation 77) 55-67. 56. Tafari N, Ferede A, Girmai M et al. Neonatal septicaemia. Ethiopian Medical Journal. 1976;14:169-77. 57. Ghafoor A, Nomini NK, Ishaq Z et al. Diagnosis of acute lower respiratory infections in children in Rawalpindi and Islamabad, Pakistan. Rev infect dis 1990;12(suppl.8):s907-s914. 58. Shann, F. Etiology of severe pneumonia in children in developing countries. Paediatric infectious diseases, 1986;5:247-52. 59. Wall RA, Corrah PT, Mabey DCW, Greenwood BM. The Etiology of lobar pneumonia in the Review of ARI Literature 57 ──────────────────────────────────────────────────────────── Gambia. Bulletin of the World Health Organization 1986;64:553-58. 60. Ikeogi, MO. Acute pneumonia in Zimbabawe: bacterial isolates by lung aspiration. Archives of disease in childhood 1988;63;1266-1267. 61. Walsh JA, Warren KS. Selective primary health care: an interim strategy for disease control in developing countries. N. Engl J Med 1979;301:967-74. 62. World Health Organization. Supervisory skills: management of the young child with an acute respiratory infection. WHO, Geneva, 1991. 63. Campbell H, Byass P, Lamont AC, et al. Assessment of clinical criteria for identification of severe acute lower respiratory tract infections in children. Lancet, 2:742-743. 1988. 64. Redd S, Vreuls R, Metsing M, Mohobane PH, Patrick E, Moteetee M. Clinical signs of pneumonia in children attending an outpatient department in Lesotho. WHO Bulletin. 1994,72(1):113-118. 65. Shann F, Hart K, Thomas D. Acute respiratory tract infections in children: possible criteria for selection of patients for antibiotic therapy and hospital admission. Bull WHO 1984, 62:749-753. 66. Cherian T, Jacob TJ, Simoes E, Steinhoff M, John M. Evaluation of simple clinical signs for the diagnosis of acute lower respiratory tract infection. Lancet,2:125-128. 1988. 67. Leventhal JM. Clinical predictors of pneumonia as a guide to ordering check roentgenograms. Clinical Pediatrics 1982;21:730-34. 68. Tafesse B. Analysis of admissions to the Ethio-Swedish Children's Hospital. Ethiop Med J 1973;11:3-12. 69. Ethio-Swedish Childrens'Hospital. Annual report to the Ministry of Health 1991-92. 1992. 70. Freij L, Sterky G. The components and economics of a small scale urban mother and child health clinic. Ethiop M J 1973;11:101-112. 71. Central Statistical Authority. Statistical Abstract 1990. Addis Ababa: CSA, 1993. 72. Shamebo D, Muhe, L, Freij L et al. The Butajira Rural Health Project in Ethiopia: Distribution of Health needs and care - a case for improved and equitable services. Social science and medicine. submitted for publication. 73. Kitaw Y. Self(lay) care in a developing country: a study of three communities in Ethiopia. Ethiopian Journal of Health development (special issue),1987;2. 74. Buschkens WFL and Slikkerveer LJ. Illness behaviour of the eastern Oromo in Harrarghie (Ethiopia). Health care in east Africa. Van Gorcum, 97-127, Assen, 1982. 75. Dagnew M. Pattern of health care utilization in a small rural Ethiopian town. Ethiop M J 1984;22:173-7. 76. Sector Review Ethiopia. Population, Health and Nutrition (1985 Report No 5299-et, p35 Document of the World bank. 77. World Health Orgnization. Report of the WHO collaborative study on breast feeding,1981, WHO, Geneva. 78. World Health Organization. Contemporary patterns of Breast-feeding. Geneva: WHO, 1980. 79. Ketsela T, Asfaw M, Kebede D. Patterns of breast feeding in western Ethiopia and their relationship to acute diarrhoea in infants. J Trop Med. Hyg. 1990;36:180-183. 80. Tadesse, E. National Breast Feeding Survey in Ethiopia: knowledge, attitude and practices among mothers and health professionals. MOH and UNICEF. 1993. Addis Ababa. 81. Teshome D, Gebru H. Xerophathalmia: a review of hospital outpatient records. Ethiop. Med. J. 1982;20:15-20. 82. Desole G, Yigezu B, Bekalu Z. Vitamin A deficiency in Southern Ethiopia. Am. J. Clin Nutr. 1987;49:780-784. 83. Gebre Medhin M, Vahlquist A, Hofyander Y, Uppsall L, Vahlquist B. Breast milk composition in Ethiopian and Swedish mothers. Am J Clin Nutr 1976;29:441-451. 84. Teshome D, Wolde Gebriel Z. Vitamin A status of preschool children in Ethiopia. ENI, Addis Ababa, 1985. 58 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── 85. World Health Organization. Joint FAO/WHO Expert Committee on nutrition, WHO Technical report series.1976; 377, 31-34 86. Hojer B, Gebremedhin, M. Sterky, G et al. Rickets and exposure to sunshine. J Trop Pediatr envir child health 1975;21:88-90. 87. Woldemariam T, Sterky G. Severe rickets in infancy and childhood in Ethiopia. J pediatr.1973;82:876-78. 88. Lulseged S. Severe rickets in a children's hospital in Addis Ababa. Ethiop M J 1990;28:175-181. 89. Muhe L. Review on potential interventions for the prevention of pneumonia in children: vitamin D deficiency. World Health Organization meeting. June 7-8, 1994. Geneva. 90. Tafari N. Low birth weight: an overview in advances in international maternal and child health (eds DB Jelliffe and EFP Jelliffe) Vol 1, chap 6, New York, Toronto.1974. 91. Zein A, Gebrekidan K, Eshete M, Haile M, Hunduma N, Makonnen T, & Sahlu T. Birth weight of hospital delivered neonates in Gondar, Northwestern Ethiopia. Ethiop med J. 1985;23:59-63. 92. Hojer B. Low birth weight infants in Ethiopia, results of hospital care. J trop pediatr environ child health 1972;18:192-195. 93. Shiferaw T. Some factors associated with birth weight in Jima, Southwestern Ethiopia. Eth. Med J. 1990;28:183-190. 94. Ahmed Zein, Z. Cigarette smoking among Ethiopian health professionals and students. N.Y. state J Med 1987;87:433-435. 95. Ahmed Zein Z, Abuhay M. The prevalence of cigarette smoking among secondary school children in Gonder city, Ethiopia. Ethiop Med J 1989:17:41-46. 96. Ministry of Health. Draft policy on national programme for the control of ARI. Sept, 1993. MOH Addis Ababa. 97. Wolde Michael Saba, Carlson DG, Kebede D. Caregivers’ knowledge, beliefs, attitudes, and Nactices on case management of ARI In a rural district in Ethiopia. EJHD 1994;8:103-103. Original article A one-year community study of under-fives in rural Ethiopia: Patterns of morbidity Lulu Muhe1, Lennart Freij2, Peter Byass3, Anita Sandström2 and Stig Wall2 Summry: A prospective weekly home surveillance study was undertaken to determine morbidity patterns within the Butajira Rural Health project in central Ethiopia. Overall, illness was reported in 5.8% of 1,216 person-years observed among rural Ethiopian children aged under 5 years. Acute respiratory infections (ARI) (prevalence 2.8%) and acute diarrhoea (2.4%) were the commonest conditions. Episodes of illness were distributed unequally among children, with a mean of 2.34 episodes per child. These included an average of 1.13 episodes of ARI (of which 0.16 had lower respiratory symptoms (ALRI)) and 1.17 episodes of acute diarrhoea. Children between 1 and 6 months old had the highest incidences of ARI, ALRI and acute diarrhoea. There were no sex differences in morbidity. However, it was found that children living in the lowlands experienced more illness.[Ethiop. J. Health Dev. 1997;0(0)61-67] Introduction Health service providers need to have adequate information about the nature, quantity, distribution and determinants of illness in populations. Such information should form the basis of effective planning, development, delivery and evaluation of services. Unfortunately, this information is either unavailable or inadequate in many developing countries, often comprising fragments of isolated data from different sources. In the absence of national data, well designed epidemiological surveys in defined populations may give clues as to the status of health in the community (1). The Butajira Rural Health Project (BRHP) is one such attempt (2). It was initiated in 1986 in the district of Butajira, about 130 km south of Addis Ababa, to establish a system for continuous demographic surveillance. Since its establishment, data on causes and determinants of mortality have been collected (3,4,5). The study base was used to carry out focused studies on specific health problems including acute respiratory infections (ARI). In addition to mortality studies, evaluations of morbidity patterns underlying mortality were envisaged to assess health needs of children in a social, economic, and health services context. In Ethiopia the information on morbidity is limited mainly to hospital data. Diseases of the respiratory tract (11% of 3500 admissions), malnutrition and deficiency states (18.5%) , neonatal disorders (16.8%) and gastroenteritis and intestinal parasitic diseases (9.8%) were the major causes of admission to a children's hospital in Addis Ababa (6). Cases with pneumonia as the principal diagnosis constituted 6% of the admissions. Outpatient attendance reports from a clinic serving a deprived area of Addis Ababa showed that ARI accounted for 35% of the 25,000 annual attendances (7). Almost all studies in Ethiopia have been done in urban populations. Since 89.7% of the country's population is rural (8), community-based epidemiological studies in rural areas are essential prerequisites for the design and implementation of effective and efficient primary health care. ______________________________________ 1 From the Ethio-Swedish Children's Hospital, Department of Paediatrics and Child Health, Addis Ababa University, P.O. Box 1768, Addis Ababa, Ethiopia, 2Department of Epidemiology and Public Health, University of Umeå, S-901 85 Umeå, Sweden and 3Nottingham School of Public Health, Queen's Medical Centre, Nottingham NG7 2UH, United Kingdom. Table 1: Prevalences of symptoms and illness entities in 1,216 person-years of observation in rural Ethiopian children aged under 5 years. Dirama Dobena Butajira Total LOCATION 60 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── characteristic rural highland rural lowland number of children person-years observed Prevalence of reported simptoms any illness diarrhoea vomiting cough fever ear discharge Prevalence of derived disease entities acute respiratory infections (ARI) acute lower respiratory infections (ALRI) gastroenteritis (GE) non-ARI/GE febrile illness 306 278 256 239 753 698 1315 1216 7.9% 2.5% 1.2% 3.6% 3.2% 0.3% 9.2% 3.3% 1.1% 3.6% 3.7% 0.7% 3.7% 1.6% 0.4% 1.5% 1.3% 0.1% 5.8% 2.1% 0.7% 2.4% 2.2% 0.3% 4.3% 0.2% 3.8% 0.6% 1.8% 0.1% 1.7% 0.1% 2.8% 0.2% 2.4% 0.3% 4.1% 0.3% 3.0% 0.4% semi-urban This study was prompted by a special interest in childhood ARI for which an intervention study was being developed within BRHP. This paper addresses approaches and methodologies in the estimation of morbidity and presents the basic morbidity data. The assessment of risk factors will be considered subsequently. Methods The study was carried out in 1991 in the Butajira district in southern central Ethiopia, 130 km south of Addis Ababa. The district has a population of 250,000 with several ethnic groups (Gurage, Amhara, Oromo). Most people live by subsistence farming, grow false banana (Ensete ventricosum), tef (Eragrosis tef), maize and wheat and graze cattle. The district can be divided into lowland (altitude less than 1,500 metres) and highland. The adult literacy rate is 22%. Most of the houses are traditional huts made of wood and clay with thatched roofs. Water is mainly drawn from rivers and wells. The district is served by one health centre, situated in the small town of Butajira, and 5 health stations. The BRHP demographic database covers 9 Peasant Associations (PA) in the district and one Urban Dwellers' Association (UDA) in Butajira town, a sample previously selected using probabilities proportional to size (2). The possibility of identifying a sufficient number of cases of acute lower respiratory infections (ALRI) for studies of risk factors and outcome was one of the considerations in determining the sample size for the morbidity study. As the mortality pattern showed considerable variations between the urban, lowland and highland rural areas (2,3) it was of interest to include communities from these three areas. Thus, one UDA from Butajira town (600 children), the rural lowland PA of Dobena (300 children) and rural highland PA of Dirama (200 children) were chosen. Field workers visited every household once per week. A nurse-supervisor was responsible for managing data collection, passing completed forms, after careful scrutiny, to the investigators who also actively participated in supervision during fortnightly field visits. Figure 1: Incidence rates for episodes of reported symptoms during 1,216 person-years of observation among under-fives in a rural Ethiopian community, divided into rural highland (white bars), rural lowland (shaded Morbidity pattern 61 ──────────────────────────────────────────────────────────── bars) and semi-urban areas (black bars). Field workers were trained in interview techniques and in the few clinical assessments which they were instructed to carry out on children with reported illness (respiratory rate, chest indrawing, grunting). They were also instructed to measure children's weight and height at 4-monthly intervals. An initial feasibility study was conducted over a period of 3 months on 30 children. The questionnaire covered common symptoms such as diarrhoea, vomiting, running or blocked nose, cough, fever, fast breathing, difficult breathing, reduced intake of food and fluids, and ear discharge. Children commonly had skin infections such as scabies, pyoderma, tinea corporis and tinea capitis as well as conjuctivitis, but these were recorded under other complaints and are not reported here. In addition to the interview, mothers were given simple calendars (recall cards) for daily recording of perceived illness. The latter comprised a photograph of the child and weekly slips of paper with seven spaces to be filled in by the mother on any day child was ill. All children under five were included in the study. Field workers studied the recall cards before starting the interview every week. They then asked about the presence of all symptoms for each day of the week. Children with reported illness and/or symptoms were clinically assessed. After the first three months, due to a shortage of forms, the weekly illness registration forms were filled in only for children who reported some illness. Supervision was tightened to make sure that no illness reports were missed. Table 2: Distribution of episodes of symptoms and illness entities among 1,315 rural Ethiopian children aged under 5 years. Episodes per child 0 1 2 3 4 5+ Total episodes Reported symptoms any illness 319 299 249 152 122 174 2839 diarrhoea 622 332 168 101 42 50 1440 vomiting 918 251 101 30 11 4 601 cough 674 316 164 82 43 36 1269 fever 574 342 204 89 57 49 1533 ear discharge 1249 46 11 4 1 4 105 Disease entities acute respiratory infections (ARI) acute lower respiratory infections (ALRI) gastroenteritis (GE) non-ARI/GE febrile illness 622 115 7 340 132 181 20 89 46 1 37 1 1368 193 622 1150 333 340 171 20 98 5 43 3 48 1 1427 209 Children reporting ill or having ALRI symptoms with a respiratory rate higher than 40/min were referred to a physician based in Butajira health centre. Chest x-rays were taken whenever possible. Outcome measures definition: The daily data on symptoms were used to compute individual prevalences for each symptom and individuals' episodes of illness. Episodes of individual symptoms were taken to have minimum durations of 1 day, with an interval of at least 3 days between adjacent episodes. The following definitions of derived entities were developed: ARI: Any day with one or more of runny nose, cough, fast breathing, difficult breathing is an ARI day. Additionally, any day not meeting the above definition, but which has one or more of fever, vomiting, feeding difficulty, and which lies within 3 days of an ARI day is also an ARI day. An ARI episode has a minimum length of 1 ARI day, with a minimum gap of 3 days between episodes. 62 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Figure 2: Incidence rates for episodes of derived disease entities (acute respiratory infections, acute lower respiratory infections, gastroenteritis and non-ARI/GE febrile illness) during 1,216 person-years of observation among under-fives in a rural Ethiopian community, divided into rural highland (white bars), rural lowland (shaded bars) and semi-urban areas (black bars). ALRI: Among ARI episodes, any occurrence of fast breathing or difficult breathing characterised that episode as ALRI. Gastroenteritis [GE]: Any day with diarrhoea is a GE day. Additionally, any day not meeting the above definition, but which has one or more of fever, vomiting, feeding difficulty, and which lies within 3 days of a GE day is itself a GE day. A GE episode has a minimum length of 1 GE day, with a minimum gap of 3 days between episodes. Non-ARI/GE Febrile illness [FE]: Any day with fever, which is not already either an ARI or a GE day, is an FE day. Additionally, any day not meeting the above definition, but which has one or both of vomiting, feeding difficulty, and which lies within 3 days of a FE day is itself an FE day. An FE episode has a minimum length of 1 day, with a minimum gap of 3 days between episodes. Using the above definitions, disease incidence rates and illness loads as a proportion of time were analysed by age, sex, and area of residence. Data entry and analysis: Each child was identified using a PA number, household number, and individual number. From these, a unique 6-digit identifier was derived. A database (dBase IV) consisting of one record per subject per week was created. Subjects' unique identifiers were included along with date and week of interview in these records. For each symptom, a 7-character string corresponding to the 7 day period was used. Each of these fields were filled "Y" or "N". Data were then converted into a one-year diary format in a separate database by fitting individual weeks of symptoms in chronological order into character strings representing occurrences of each symptom. Because of software constraints on field width (255 characters) a 2:1 compression algorithm was used to represent a year's data in 183 characters. Programs were developed to apply the above definitions to the daily data, producing counts of days and episodes for each child, for each symptom and derived entity. Initially this approach was tested and evaluated on a random 10% sample of children, allowing consideration of episode definitions on a strictly a priori basis; in fact the definitions remained unchanged after considering the sample results, and were subsequently applied to the complete data. Results There were 1,315 children involved in the study over the one year period (52.7% males). 128 births were recorded and 117 children moved into the study area. 67 children died during the study and 30 out-migrated from the area. A total of 1,216 person-years (p-y) were observed, among which symptoms and derived entities were recorded as shown in Table 1. The overall illness load was Morbidity pattern 63 ──────────────────────────────────────────────────────────── markedly lower in Butajira UDA compared with the rural areas. Diarrhoea and fever were reported most commonly in the lowland area. Ear discharge was relatively rare in all study areas. Figure 3: Age-specific incidence rates for episodes of reported symptoms during 1,216 person-years of observation among under-fives in a rural Ethiopian community. Age groups, from left to right, are under 1 month, 1-2 months, 3-5 months, 6-11 months, 12-23 months and 2 years & over. Incidence rates for episodes of symptoms and of derived entities are shown in Figures 1 and 2 respectively, divided geographically. Overall illness occurred at 2.34 episodes/p-y. Individual symptoms showed rates of 1.18 episodes/p-y for diarrhoea, 0.49 for vomiting, 1.04 for cough, 1.26 for fever and 0.09 for ear discharge. Derived entities occurred at 1.13 episodes/p-y for ARI, 0.16 for ALRI, 1.17 for GE and 0.17 for FE. The incidence of reported symptoms and derived entities varied very little by sex. The M:F ratio for overall illness was 1:1.05. Episodes were distributed among children as shown in Table 2. 319 children (24.2%) were reported to have no illness, while 174 (13.2%) had more than 5 episodes. Only 50 children (4%) had chronic respiratory illness as defined by an ARI episode lasting more than 4 weks, and 21 (1.6%) had an episode of GE of more than 2 weeks. The distributions of all reported symptoms and derived entities differed significantly from Poisson distributions, indicating clustering of morbidity episodes among some children. 22% of the children accounted for more than 50% of the reported illness episodes. A breakdown by age depicts the sharp drop in the incidence of both reported illness and derived entities after the age of 12 months, as shown in Figures 3 and 4. The peak incidence of ARI was in the age group between 3 and 6 months and for ALRI between 1 and 6 months. For GE, the peak incidence is between 1 and 6 months. Ear discharge occurred most commonly in the first month. 64 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Figure 4: Age-specific incidence rates for episodes of derived disease entities (acute respiratory infections, acute lower respiratory infections, gastroenteritis and non-ARI/GE febrile illness) during 1,216 person-years of observation among under-fives in a rural Ethiopian community. Age groups, from left to right, are under 1 month, 1-2 months, 3-5 months, 6-11 months, 12-23 months and 2 years & over Discussion Any consideration of morbidity data, particularly in developing countries, has to look carefully at methodological issues. Our study used a feasibility study period of 3 months before the main study was launched to improve the skill of our interviewers. The additional recall calendar was designed to improve the recall problem of mothers. Despite strict supervision, underreporting cannot be totally excluded because healthy children were not registered for part of the study period due to a shortage of forms. Without considering the latter possibility, the rates that were found in this study for ARI, ALRI, and diarrhoea in rural under-five children in Ethiopia are quite high. Conversely, we may have slightly overestimated incidence by not making special allowance for episodes occurring on the first day of the study, rather assuming them to start on that day. In view of the overall pattern of frequent, short episodes this is unlikely to be a significant effect. We have not separately addressed questions of malnutrition, although the 1.6% of children with chronic GE episodes may be relevant here. Many rural studies of morbidity have used weekly home surveillance studies with questionnaires administered by non-medical personnel. Others have used biweekly visits or fortnightly visits, with different implications for recall bias. Some have used clinic or even hospital patients as the basis of observations. Case definitions have also varied between studies. These design differences have implications both for the validity and the reliability of morbidity data. Overall however we consider that our approach has resulted in a fair picture of morbidity in our communities. Morbidity rates were highest in the lowland area (Dobena), and lowest in the semi-urban area of Butajira. This follows the same pattern as the mortality data collected two years earlier in the same project (2,3). Other community based studies have indicated that ARI, diarrhoea and malnutrition are the principal diseases among under-fives in developing countries (9,10,11). The median diarrhoeal morbidity rate in under-fives (episodes/p-y) has been quoted as 1.6 for Africa, 2.6 for Asia and 1.8 for Latin America (12). The incidence of ARI ranges from 5 to 9 /p-y in urban areas both in developed and developing countries (13-19). The same range was found in an urban slum area in Addis Ababa (20). In rural areas lower incidence rates have been reported, ranging from 1 to 3 /p-y, similar to the results in this study. This is conceivably explained by problems associated with overcrowding, inadequate housing conditions, malnutrition and poor sanitation that are worse in shanty cities than in rural communities. Studies in rural communities in Bangladesh (21), China (22), Indonesia (23), and Papua New Guinea (24) showed incidence rates similar to ours for ARI. A prospective weekly home surveillance study in rural Kenya also gave an ARI incidence of 3.4 /p-y (25). A study in a northern rural community in Ethiopia showed a rate of 2.8 /p-y in infants and 3.1 /p-y in children (26). Even Morbidity pattern 65 ──────────────────────────────────────────────────────────── though our rates of ARI episodes were similar to other rural studies, the rate of ALRI (0.2 /p-y) in this population was much higher than those shown in rural studies from China (0.07 /p-y)(22), Kenya (0.09 /p-y)(25) and Thailand (0.07 /p-y)(18). Although wide differences in incidence rates between urban and rural communities have been quoted in various studies, the methodologies used in the two groups have not always been comparable. One study in Trinidad which used the same methods in both rural and urban areas gave a reported incidence of respiratory illness of 7.7 /p-y in urban Port of Spain, against 4.4 /p-y in rural Sangre Grande (27). The age and gender-specific incidence of episodes of illness and derived entities in this study is generally similar to previous knowledge (13,20). The greater vulnerability of weanling infants to ARI and GE has been widely observed in various settings in developing countries. In our case the peak incidence occurred between 2-6 months. In a study from Manila, the peak age group for ARI was 6-12 months (13). Similarly, the highest ARI incidence was in infants below 1 year in a Kenyan study (25). The longitudinal follow-up in this study has shown that there are certain children who seem to have a tendency to get repeated episodes of illness. The distribution of episodes of reported symptoms and derived entities among individuals was far from random. It may be that first episodes of infection beget other infections so that the more episodes a child has had, the more predisposed he is to further illness. Alternatively other local or environmental factors may put certain children at much higher risk of these common infections. Further analysis of factors associated with frequent episodes of illness in a child is planned, since there are important health service implications in these cases. In conclusion, this study has identified levels of morbidity that are obviously of public health importance, reminding the health authorities of the urgent need to reduce the burden of illness in these communities. The study has demonstrated that a prospective weekly home surveillance method combined with a recall calendar can give useful information on the nature, magnitude, and distribution of illnesses. Further work on these data are required to identify specific risk factors. The results of such morbidity studies are a prerequisite to the planning of locally adapted and affordable disease-specific interventions, and the methodologies used can become important tools in the evaluation of such initiatives. Acknowledgements We acknowledge the financial support of the Swedish Agency for Research in Developing Countries (SAREC). This study would not have been possible without the hard work put by the field supervisor, Mr Yemiru Teka and all the field workers, and the massive data entry would not have been possible without the help of Mr Kidanemariam Woldeyesus. We also acknowledge the participation in planning the study of Mr Göran Lönnberg and Dr Ingela Krantz. We would also like to thank Dr Sandy Gove of the WHO CDR/ARI programme for her help and advice. References 1. Ekanem E. Field epidemiology: methodological constraints and limitations in developing countries. Public Health, 1985;99:33-36. 2. Shamebo D, Sandström A and Wall S. Epidemiological surveillance for health research and intervention in primary health care. Scandinavian Journal of Primary Health Care, 1992;10:198-205. 3. Shamebo D, Muhe L, Sandström A and Wall S. (1991). Mortality pattern of the underfives. Journal of Tropical Paediatrics, 1991;37:254-261. 4. Shamebo D, Sandström A, Muhe L, Freij L, Krantz I, Lönnberg G, and Wall S. A nested casereferent study of underfive mortality and its public health determinants. Bulletin of the World Health Organization, 1993;71:389-396. 5. Shamebo D, Muhe L, Sandström A, Freij L, Krantz I and Wall S. (in press). A nested case-referent study of underfive mortality and its health and behavioural determinants. 6. Tafesse, B. Admission patterns to the Ethio-Swedish Children's Hospital, Addis Ababa. Ethiopian Medical Journal 1973;11:3-12. 7. Freij L, Sterky G. The components and economics of a small scale urban mother and child health 66 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── clinic. Ethiopian Medical Journal, 1973;11:101-112. 8. Ethiopian Statistical Abstract. Central Statistics Office, Addis Ababa, 1984;23-24. 9. Lindtjorn B, Alemu T, Bjorvatn B. Child health in arid areas of Ethiopia: longitudinal study of the morbidity in infectious diseases. Scandinavian Journal of Infectious Disease, 1992;24:369-377. 10. Tumwine JK, Mackenzie S. Child survival in a rural area in Zimbabwe: are we winning? Central African Journal of Medicine, 1992;38:30-36. 11. Biddulph J. Child health in the third world. Medical Journal of Australia, 1993;159:41-45. 12. Rohde JE, Northrop RS. Taking science where diarrhoea is. In: CIBA Foundation Symposia, vol. 42 (new series), Elsevier/North-Holland, Amesterdam, 1976; pp.339-358. 13. Tupasi TE, De Leon LE, Lupissan Socorro et al******. Patterns of ARI in children: a longitudunal study in a depressed community in Metro Manila. Reviews of Infectious Disease, 1990;12:S940-S949. 14. Monto AS, Ullman B. Acute respiratory illness in an American community: the Tecumseh study. Journal of the American Medical Association, 1974;227:164-169. 15. Fox JP, Cooney MK, Hall CE. The Seattle Virus Watch: V. Epidemiologic observations of rhinovirus infections, 1965-1969, in families with young children. American Journal of Epidemiology, 1995;101:122-143. 16. Kamath KR, Feldman RA, Sundar Rao PSS, Webb JKG. Infection and disease in a group of south Indian families. II. General morbidity patterns in families and family members. American Journal of Epidemiology, 1969;89:375-****. 17. Hortal M, Benetez A, Contera M, Etorena P, Montano A, Meny M. A community based study of acute respiratory tract infections in children in Uruguay. Review of Infectious Disease, 1990;12:S966S973. 18. Vathanophas K, Sangchai R, Raktham S. et al****. A community based study of acute respiratory tract infection in Thai children. Reviews of Infectious Disease, 1990;12:S957-S965. 19. Borrero I, Fajardo L, Bedoya A., et al****. Acute respiratory tract infections among a birth cohort of children from Cali, Colombia, who were studied through 17 months of age. Reviews of Infectious Disease, 1990;12:S950-S956. 20. Freij L, Wall S. Exploring child health and its ecology. The Kirkos study in Addis Ababa. Acta Paediatrica Scandinavica, 1977;267:Suppl. 20-31. 21. Black RE, Brown KH, Becker S, Yunus M. Longitudinal studies of infectious diseases and physical growth of children in rural Bangladesh. American Journal of Epidemiology, 1982;115:305315. 22. Lei-Mei Gao. A primary report of acute respiratory infections surveillance in Dong Guan Brigade, document WHO/WPR/ARI/82.13,2, WHO, Geneva 1982. 23. Karyadi A. Acute viral respiratory infections: their public health importance in Indonesia, document WHO/VIR/SG/79, WHO, Geneva 1979. 24. Smith D. Patterns of ARI morbidity, mortality and health service utilization in the Asaro valley, Papua New Guinea, 1980 - 1981, document WHO/WPR/ARI/82.7, WHO, Geneva 1982. 25. Wafula EM, Onyango FE, Mirza WM, Macharia WM. et al*****. Epidemiology of acute respiratory tract infections among young children in Kenya. Reviews of Infectious Disease, 1990;12:S1035-S1038. 26. Dodge RE, Demeke T. The epidemiology of infant malnutrition in Dabat. Ethiopian Medical Journal, 1970;8:53-66. 27. Sutton RNP. Minor illness in Trinidad: a longitudinal study. Transactions of the Royal Society of Tropical Medicine and Hygiene, 1965;59:212-220. Original article A one-year community study of under-fives in rural Ethiopia: public health determinants of morbidity Lulu Muhe1, Lennart Freij2, Peter Byass3, Anita Sandström4, Stig Wall4 Summary: Based on a weekly home surveillance study, morbidity of underfives in a rural Ethiopian community and possible public health determinants of morbidity were measured. Using poisson regression models, the study showed that there is a significant impact on underfive morbidity from few sanitational, parental and housing factors. Gastroenteritis was particularly associated with sanitational factors, and acute respiratory infections were particularly associated with parental factors. Underfive morbidity was increased 1.20 times in highland rural and 1.44 times in lowland rural areas compared to urban areas. Among sanitational factors, the absence of piped water for a household was an important determinant of underfive morbidity. Among Housing factors, the type of roof and lighting of the house and among parental factors illiteracy of either parents and occupation of the father as farmer were found to be independently associated with increased morbidity. The study concludes by discussing possible applications of the results in health planning and intervention programmes. [Ethiop. J. Health Dev. 1997;0(0):69-76] Introduction Both hospital-based and community-based studies confirm that diarrhoeal diseases and acute respiratory infections (ARI) are the leading causes of morbidity among underfive children in developing countries (1-5). While low socio-economic status is associated with increased morbidity from ARI and diarrhoea (5), it is important to understand the relative contributions of specific factors such as household size, parental literacy, occupation, place of residence, household income, low birth weight, source of water etc which may determine the magnitude and severity of disease (6). Such specific possible risk factors could be averted by affordable specific programmes of prevention and management to reduce morbidity and mortality from ARI and diarrhoea. Mother's education, for example, has been shown to have beneficial effects on the survival of under-five children (7-9). Improvements in access to water and sanitation have also been shown to contribute to improved personal hygiene and thus reduced child mortality (10). There is also evidence that the attack rate of ARI is increased among the nutritionally compromised (11-13). Large family size, increasing birth order, overcrowding households and high sleeping density are environmental factors that may be expected to promote the transmission of respiratory pathogens and increase the size of the infecting inoculum, thus, increasing the risk to ARI morbidity (14). This paper assesses the association of public health factors and common childhood illnesses especially ARI and diarrhoea among under-five children. Identification of specific public health determinants of ARI and diarrhoea in childhood was considered an essential prerequisite in the design of an appropriate intervention package which was planned and is now being launched in the study communities. Nutritional and behavioural determinants of morbidity are also identified but will be reported in a separate paper. ______________________________________ 1 From the Ethio-Swedish Children's Hospital, Department of Paediatrics and Child Health, Addis Ababa University, P.O. Box 1768, Addis Ababa, Ethiopia, 2Department of Medical Microbiology & Immunology, University of Göteborg, Guldhedsgatan 10, 41346 Göteborg, Sweden, 3Nottingham School of Public Health, Queen's Medical Centre, Nottingham NG7 2UH, United Kingdom and 4 Department of Epidemiology and Public Health, University of Umeå, S-901 85 Umeå, Sweden Methods The study was performed within the Butajira Rural Health project (BRHP), in Butajira district in southern central Ethiopia, 130 km from Addis Ababa (15-18). The BRHP demographic database 68 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── covers 9 Peasant Associations (PA) in the district and one Urban Dwellers' Association (UDA) in Butajira town, a sample previously selected using probabilities proportional to size (15). The possibility of identifying a sufficient number of cases of acute lower respiratory infections (ALRI) for studies of risk factors and outcome was one of the considerations in determining the sample size for the morbidity study. As the mortality pattern showed considerable variations between the urban, lowland and highland rural areas (16) it was of interest to include communities from these three areas. The details of the study background and methods were described in a morbidity pattern paper among under-five children in a previous report (19). A cohort of 1315 under-five children were followed by a weekly home surveillance method plus use of a recall card over a period of one year. The recall card is a simple calendar with a photograph of the child for daily recording of perceived illness by the mother. The weekly interviews consisted of symptoms and signs as perceived by mothers and few clinical observations made by the field workers who had meticulous training and practice for 3 months. The results were used to define derived disease entities like diarrhoea and acute respiratory illnesses. Data on household, parental and childhood factors were collected at the beginning of the study for most children and at the time of enrollment for inmigrants and newbirths during the study period. A postulated conceptual model of public health factors leading to increased morbidity is shown in Figure 1. Based on the model, data on Figure 1: Conceptual model of morbidity determinants in rural Ethiopia parental and child factors included questions on age of mother and father, marital status of mother and father, ethnicity, religion, literacy, present occupation, position in mass organizations, position in religious organizations, and number of siblings alive and dead. The data on housing included number of household members, number below 5 years, size of house, shape of house, number of windows, number of windows that are open during visit, type of roofing of the house, type of floor, place of fireplace in the house, type of fuel used mostly, source of light, sleeping room alone or together, presence of a compound, main source of water, distance to fetch water, daily amount of water, type of latrine, ownership of latrine, and presence of livestock in the household. The majority of the collected variables were not expected to change over the study period and therefore data collected at the beginning of the study was considered sufficient. However, for variables like breast feeding status, supplementary feeding and immunization status which are not analysed in this paper, data was collected both at the beginning and at the end of the study. Episodes of illness were defined as previously described (19) and calculated for each child under surveillance. Individual Table 1: Illness rate ratios for various risk factors in a prospective study of morbidity among 1,304 rural Ethiopian children aged under 5. Group Parameter Levels n@ bivariate rate ratio* group rate ratio+ Publich health determinants of morbidity 69 ──────────────────────────────────────────────────────────── Age age at mid point of servillance Sex housing member number below 5 years shape of house size of hou (m2) number of rooms number of windows type of roof fireplace lighting compound situation main water xource Time taken to fetch wat latrine livestock in household maternal age marital status ethnicity religion literacy number of children died Paternal age marital status ethnicity religion literacy occupation under 12 m 12 to 23 m 24 m & over 10 & over 7 to 9 4 to 6 Under 4 2 & over 1 None circular Rectangula 40 & over 30 to 39 20 to 29 Under 20 4 & over 3 2 1 3 & over 2 1 none corrugate Thatch elsewhere Sleeping area electric none electic no Yes piped not piped under 5 min 5 to 9 min 10 to 19 min 20 min & over yes no no yes 35 & over 25 to 34 under 25 married Others 128 289 887 104 417 617 127 625 543 136 487 774 310 212 495 240 85 213 359 579 205 225 394 480 751 513 641 615 681 573 854 384 649 611 172 233 374 525 656 600 584 605 448 625 212 822 112 1.000 1.433 0.846 1.000 1.323 1.533 1.710 1.000 1.134 1.058 1.000 0.620 1.000 0.915 1.208 0.332 1.000 1.085 1.005 1.691 1.000 1.187 1.149 1.735 1.000 1.738 1.000 1.668 1.000 1.777 1.000 0.757 1.000 1.827 1.000 0.846 0.904 1.307 1.000 1.498 1.000 1.571 1.000 1.045 1.073 1.000 1.324 miscellaneous Dobi Meskan Silti Sodo & Marako christian/ot her Moslem literate Illiterate none 1 or more 35 & over Under 35 married Other miscellaneous Dobi Meskan Silti Sodo & Marako christian/ot her Moslem literate Illiterate non-farmer Farmer no yes 230 144 635 127 149 437 903 437 844 677 627 713 260 783 200 217 97 507 99 60 276 700 604 374 433 543 290 889 1.000 0.902 0.931 1.137 1.187 1.000 1.234 1.000 1.470 1.000 1.571 1.000 1.009 1.000 1.123 1.000 0.801 0.891 0.963 0.821 1.000 1.163 1.000 1.494 1.000 1.783 1.000 0.916 membership of mass oranisation Note: @where the total n for a parameter is less than 1,304, the remaining cases are missing for that parameter *bivariate illness rate ratios calculated for each parameter separately, using poisson regression +multivariate illness rate ratios calculated by poisson regression, modelling all parameters within the group 1.000 1.090 1.000 1.034 1.000 1.257 1.000 1.012 1.000 1.077 1.000 1.000 1.1.4 1.000 1.457 1.000 1.123 1.000 1.334 1.000 1.114 1.000 1.693 1.000 1.119 1.000 1.044 1.000 1.024 1.000 1.101 1.000 1.225 1.000 1.181 1.000 1.226 1.000 1.317 1.000 1.170 1.000 1.070 1.000 1.114 1.000 0.987 1.000 1.090 1.000 1.203 1.000 1.623 1.000 1.022 episode counts together with durations of surveillance were used as outcome variables and rate multipliers respectively in a Poisson regression model using EGRET software (20), in order to assess the impact of various risk factors on morbidity. Initial models were constructed for rates of overall illness against conceptual groups of risk factors. The within-group adjusted rate ratios from these 70 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── models were then used as a basis for the calculation of an individual multiplicative risk index for each group. Using these indices, multivariate Poisson regression models of various morbidity rate ratios were developed, including age, sex and, optionally, geographical area. Similar within-area models were also studied for overall illness. Results Risk factor and morbidity data were available for 1,304 children, the majority of whom were under surveillance for a complete year. Table 1 shows bivariate morbidity rate ratios for overall illness for each of the risk factors assessed. Apart from age and sex, these are grouped into housing, sanitation, maternal and paternal factors respectively. On the basis of the bivariate ratios, each factor was dichotomised, and a within-group rate ratio for each factor, adjusted for all other factors in the group, is also shown in Table 1. Some factors, particularly where fathers were unavailable for interview, unavoidably have a number of missing data points, as can be seen from the total number of responses to each factor in Table 1. Individual risk indices for housing, sanitation, maternal and paternal factors were calculated using the group rate ratios from Table 1. In general missing data were taken to have no effect on an individual index. However, for 316 cases in which no paternal factors were recorded, a paternal index value equal to the mean of that for the remaining 988 cases was arbitrarily assigned in order to prevent the missing data from distorting the overall distribution of this index. All these indices were then grouped by quartile, and Table 2 shows Poisson regression models of adjusted rate ratios for illness, gastroenteritis and acute respiratory infections (ARI) against these indices, together with age and sex. Gastroenteritis was particularly associated with sanitation factors, and ARI was particularly associated with parental factors. Housing factors contributed relatively little to the overall multivariate models of morbidity. Publich health determinants of morbidity 71 ──────────────────────────────────────────────────────────── Figure 2: Adjusted illness rate ratios for household, sanitation and parental risk indices, by urban, rural lowland and rural highland areas. Vertical bars represent 95% confidence intervals. 72 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Table 2: Adusted rate ratios for episodes of illness, gastroenteritis and acute respiratory infedctions (ARI) by age, sex, and risk indices for housing sanitation, maternal and paternal factors, based on community morbidity surveillance for a one-year period among 1,304 rural Ethiop[ian children aged under 5. Rate ratios are calculated by poisson regression, with all factors in the model. Risk indices have been divided into quartiles, as indicated by the mid-quartile values for each index. 95% confidence intervals for rate ratios are shown in brackets. risk factor age category under 12 m 12 to 23 m illness 1.000 1.508 (1.279-1.777) gastro-enteritis 1.000 1.598 (1.281-1.991) ARI 1.000 1.562 1.240-1.968) 24 m & over 0.896 (0.764-1.051) 0.746 (0.601-0.925) 0.861 (0.688-1.078) Sex male female 1.000 1.074 (0.998-1.157) 1.000 1.041 (0.937-1.155) 1.000 1.013 (0.911-1.128) Housing index 1.000 1.000 1.000 2 (MQV 1.579) 3 (MQV 2.393) 4 (MQV 2.924) 1 (MQV 1.000) 1.046 (0.924-1.183) 1.070 (1.243-1.241) 1.241 (1.058-1.457) 1.000 1.102 (0.927-1.310) 1.122 (0.911-1.382) 1.223 (0.997-1.532) 1.000 1.098 (0.915-1.317) 1.140 (0.917-1.419) 1.221 (0.966-1.543) 1.000 2 (MQV 1.044) 3 (MQV 1.809) 4 (MQV 2.024) 1 (MQV 1.350) 2 (MQV 1.774) 3 (MQV 1.774) 4 (MQV 2.548) 1 (MQV 1.214) 1.222 (1.075-1.389) 1.441 (1.223-1.697) 1.383 (1.164-1.642) 1.000 1.348 (1.127-1.612) 1.574 (1.250-1.981) 1.495 (1.174-1.905) 1.000 1.348 (1.116-1.629) 1.474 (1.157-1.878) 1.472 (1.143-1.895) 1.000 1.006 (0.893-1.132) 1.196 (1.065-1.345) 1.231 (1.094-1.384) 1.000 1.055 (0.894-1.244) 1.156 (0.979-1.365) 1.275 (1.081-1.504) 1.000 1.030 (0.864-1.228) 1.215 (1.022-1.444) 1.415 (1.193-1.678) 1.000 2 (MQV 1.755) 3 (MQV 1.848) 4 (MQV 2.391) 1.080 (0.955-1.221) 1.237 (1.082-1.414) 1.338 (1.164-1.538) 1.042 (0.880-1.235) 1.102 (0.914-1.328) 1.225 (1.009-1.486) 1.048 (0.874-1.256) 1.256 (1.033-1.527) 1.463 (1.196-1.788) (MQV 1.370) Situation index Maternal The same model with the addition of an urban/lowland/highland variable was also investigated for overall illness. This reduced the effect of all the other indices, and, taking the urban rate ratio as 1.000, highland and lowland areas were associated with adjusted rate ratios of 1.20 and 1.44 respectively (95% confidence intervals 1.03 to 1.39 and 1.23 to 1.67). The complete data for overall illness were then divided into three separate models for the urban, highland and lowland areas. These were each analysed in a similar manner to the overall model, and the relationships between risk indices and illness rate ratios are shown in Figure 2. The rate ratios shown are adjusted for age and sex, with the first quartile rate ratios set at 1.00, 1.20 and 1.44 for the urban, highland and lowland models respectively, in accordance with the area adjusted rate ratios from the overall model described above. Discussion In this study of public health determinants of morbidity among underfive children in rural Ethiopia, sanitational factors came out having the higher impact on general illness load as well as on the incidence of ARI and diarrhoea compared to housing and parental factors. In conformity to other studies (10), underfive morbidity was significantly and independently associated with the presence of Publich health determinants of morbidity 73 ──────────────────────────────────────────────────────────── piped water. The availability of latrine or the presence of livestock in the house did not come out as significant on multivariate analysis even though the rate ratios were high on bivariate analysis. Among housing factors, type of roof i.e. thatched roofing versus corrugated iron as well as use of fireplace versus electricity for lighting were associated with increased morbidity among the underfives. Among parental factors, illiterate mothers and illiterate and farming fathers predisposed the under-five to a higher illness rate. Maternal education was found to be a significant risk factor for morbidity even when controlling for other variables in our study as well as other studies from Guatemala and Uruguay (21, 22). Maternal education was not important factor in ARI morbidity in a study from Thailand (23). Unmarried mothers and mothers having more than one child dead have also significantly high risk ratio to morbidity. The above factors i.e. young age of mothers, illiteracy and being unmarried could be addressed by increasing individual and public awareness to the problems by giving specifc health education and mass education. Among variables related to fathers, a similar conclusion could be made on paternal age, marital status, and literacy. A striking finding among paternal variables is that being a farmer was a significant risk to morbidity among the under-fives. The latter may be explained on the basis of the low socio-economic status that farmers generally face in the study area. Low socioeconomic status can be improved only on a long term programme of the country. In the bivariate analysis of housing variables, number of household members, size of the house, number of rooms, presence of windows, type of roof, presence of fireplace in the sleeping area of the house, source of light gave a significantly high bivariate rate ratio. However, on multivariate analysis, all except type of roofing, source of light and shape of house disappeared. The latter three factors came out as important household determinants of morbidity independently of other variables. Unlike common beliefs and results of some studies (24), number of household members did not affect underfive illness rate. It should be noted that in the case of the two housing variables, shape of house and presence of a compound, the rate ratio which was higher for circular houses and for no compound on the bivariate analysis, reversed on multivariate analysis. The latter phenomenon emphasizes the complexity of the interaction of such factors and points to the necessity of multivariate analysis in studying multiple variables with possible confounding effects. The type of fuel used for cooking being predominantly biomass for all households has prevented us from anlysing its effect on underfive morbidity. In conformity to other studies, the number of children below 5 years in the household was not significant even on bivariate analysis (25). Because of the small number of children present in the study in the age group below 12 months, the differential effects within infancy could not be studied. The bivariate analysis proved that children between one and 2 years are at more risk of illness than infants below 1 year and those above 24 months are protected from illness. The latter is significant particularly for gastroenteritis. Other studies agreed that the age group above 24 months is at less risk to ARI morbidity than those below 24 months (25, 26). Unlike results of other studies (22,25,26), sex does not seem to influence the incidence of gastroenteritis or ARI. When risk ratios are computed for risk indices after dividing them into quartiles, it was shown that sanitation index is significantly affecting both gastroenteritis and ARI but more particularly gastroenteritis; maternal index and paternal index are affecting both of them but more particularly ARI. The housing index is not affecting gastroenteritis or ARI. A study of these indices on acute lower respiratory infections and acute febrile illness was not possible because of the small number of these cases. In contrast to our findings, Cruz et al showed that parental education did not influence the incidence of ARI (22). However, they also showed that the number of household members did not influence the incidence of ARI (22). A study of morbidity by study areas showed that the rural lowlands had a significantly higher rate of illness than the rural highlands. Similarly the rural highlands had more illness rate than the semi-urban Butajira town. It is shown in the figures that in the lowlands the adjusted illness rate ratio increases 74 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── with increase in the sanitation index and the household index but decreases or remains the same with increase in parental indices. Conversely, in the highlands, the adjusted illness rate ratio increases with increase in household index, and parental indices while it even decreases with increase in the sanitation index. This implies a greater impact on illness rate is obtained by improvement in sanitation and household factors rather than parental factors in the lowlands compared to the highlands. In the semiurban Butajira town, the adjusted illness rate ratio is increased by increase in the maternal and paternal risk indices. Thus, efforts put to improve paternal factors rather than sanitational or household factors in Butajira town will reduce the illness rate which is already much better than that of the rural areas. These differences between the study areas underline the need to address local problems in order to design specific recommendations for interventions. In conclusion, this study proved the presence of a significant impact on under five morbidity in rural central Ethiopia from few sanitational, parental and housing factors. Among parental variables studied, illiteracy of either parents and occupation of father as farmer and among housing variables studied, type of roof and lighting of the house were shown to determine morbidity independently. It is conceivable that some of the parental factors like illiteracy can be improved by a short-term, affordable national programmes and raising general education and public awareness while other factors like occupation and housing may require decades to change. Our study identified the absence of piped water as an important underfive morbidity determinant. Such a study could be used to convince politicians of developing countries often armed with meagre resources and to support health planners in the prioritization of specific programmes like provision of clean and safe water to the rural lowland communities or education of parents in the rural highland communities. Further research is required to understand the differences between the study areas in more detail and apply them for priority setting. Acknowledgements We acknowledge the financial support of the Swedish Agency for Research in Developing Countries (SAREC). We also acknowledge the hard work put by the field supervisor, Mr Yemiru Teka and the field workers. The massive data entry required in this study would not have been possible without the help of Mr Kidanemariam Woldeyesus. We also acknowledge the participation in planning the study of Dr Ingela Krantz and Mr Göran Lönnberg. We would also like to thank Dr Sandy Gove of the WHO CDR/ARI programme for her help and advice. References 1. Parker RL. Acute respiratory illness in children: PHC responses. Health policy and planning. 1987;2(4):279-88. 2. Wafula AM, Onyango FE, Mirza WM. et al. Epidemiology of acute respiratory tract infections among young children in Kenya. Review of Infectious diseases. 1990;12 suppl8:S1035-S1038. 3. Tafesse B. Admission patterns to the Ethio-Swedish Children's Hospital, Addis Ababa. Ethiop Med J, 1973;11:3-12. 4. Taha TE AbdelWahab MM, & Wallace HM. Morbidity patterns in a new paediatric hospital in Juba, Sudan. Child:care, health and development, 1986;12:111-120 5. Tupasi TE, Velmonte MA, Sanvictores MEG et al. Determinants of morbidity and mortality due to acute respiratory infections: implications for intervention. The Journal of infectious diseases,1988;157(4):615-23. 6. Adedoyin MA & Watts SJ. Child health and child care in Okelele: an indigenous area of the city of Ilorin, Nigeria. Social science and medicine, 1989;29:1333-41. 7. Majumder AK. Maternal factors and infant and child mortality in Bangladesh. Journal of Biosocial science,1988;20:89-98. 8. Chen LC. Primary health care in developing countries: overcoming operational, technical and social barriers. Lancet,1986;2:1260-65. 9. Cleland JG & Van Ginneken JK. Maternal education and child survival in developing countries: the search for pathways of influence, social science and medicine,1988;27:1357-68. 10. Merrick TW. The effect of piped water on early childhood mortality in urban Brazil, 1970 to 1976. Demography,1985;22:1-24. 11. Mata LJ. The children of St. Maria Canque. The MIT Press. Cambridge, Mass, and London, England. 12. Scrimshaw NS. Synergistic and antagonistic interactions of nutrition and infection. Fed Proc. 1966;25:1679-81. 13. Suskind RM. (ed) Malnutrition and the immune response. Raven press, NewYork. 1977. 14. Stansfeld SK. Acute respiratory infections in the developing world: strategies for prevention, treatment and control. Pediatr Infect Dis J. 1987;6:622-9. 15. Shamebo D, Sandström A, Wall S. Epidemiological surveillance for health research and intervention in primary health care. Scandinavian Journal of Primary Health Care, 1992;10:198-205. 16. Shamebo D, Muhe L, Sandström A, Wall S. Mortality pattern of the underfives. Journal of Tropical Paediatrics, 1991;37:254-261. 17. Shamebo D, Sandström A, Muhe L, Freij L, Krantz I, Lönnberg G, Wall S. A nested case-referent study of underfive mortality and its public health determinants. Bulletin of the World Health Organization, 1993;71:389-396. 18. Shamebo D, Muhe L, Sandström A, Freij L, Krantz I, Wall S. (in press). A nested case-referent study of under-five mortality and its health and behavioural determinants. Annals of Tropical Paediatrics. 19. Muhe L, Freij L, Byass P, Wall S. A one -year community study on under-fives in rural Ethiopia: morbidity patterns. Submitted for publication. 20. EGRET -Epidemiological Graphics, Estimation, and Testing package. Data file definition. version 0.19.2(c) copyright 1985-1990, SERC. 21. Hortal M, Benetez A, Contera M, Etorena P, Montano A, Meny M. 1990. A community based study of acute respiratory tract infections in children in Uruguay. Review of Infectious Disease. 1990;12:S966-S973. 22. Cruz JR, Pareja G, Fernandez AD, Peralta F, Caceres P, & Cano F. Epidemiology of acute respiratory tract infections among Guatemalan ambulatory preschool children. Rteview of Infectious Diseases. 1990;12:S1029-S1034. 23. Vathanophas K, Sangchai R, Raktham S. et al. A community based study of acute respiratory tract infection in Thai children. Reviews of Infectious Disease, 1990;12:S957-S965. 24. Borrero I, Fajardo L, Bedoya A, et al. Acute respiratory tract infections among a birth cohort of children from Cali, Colombia, who were studied through 17 months of age. Reviews of Infectious Disease, 1990;12:S950-S956. 25. Tupasi TE, De Leon LE, Lupissan Socorro et al. Patterns of ARI in children: a longitudunal study in a depressed community in Metro Manila. Reviews of Infectious Disease,1990;12:S940-S949. 26. Selwyn BJ. The Epidemiology of acute respiratory tract infection in young children: comparison of findings from several developing countries.1990. Reviews of Infectious Diseases, 1990;12:S870-S888. Original article A one year community study of under-fives in rural Ethiopia: Health and behavioural determinants of morbidity Lulu Muhe1, Peter Byass2, Lennart Freij3, Anita Sandström4, Stig Wall4 Abstract: Based on a one-year weekly home surveillance study, morbidity patterns of 1,304 children under five years of age in a rural Ethiopian community were measured, together with nutritional and health behavioural determinants. Using poisson regression models, the study showed that nutritional and health care factors make a significant impact on under-five morbidity. Gastroenteritis was particularly associated with child care factors, while acute respiratory infections were particularly associated with nutritional factors. Lack of immunization, low birth weight and pre-term delivery(more than one month early) were not found to have any independent effect on morbidity. Breast feeding was universal, but the introduction of supplementary foods was found to protect from excess morbidity. The study concludes by discussing possible applications of the results in intervention programmes. [Ethiop. J. Health Dev. 199-;0(0):0-00] Introduction A proper understanding of infant and child health requires consideration of socio-economic, nutritional and behavioural factors that might modify it (1,2). Even though low socio-economic status has been shown to be associated with increased morbidity(2), it is important to understand the relative contributions of specific factors such as feeding patterns, nutritional status, birth order and birth weight, which might influence the magnitude and severity of disease (3). In order to develop and implement educational, health system and health policy elements of interventions aimed at reducing excess morbidity as well as mortality, in developing countries, such factors need to be identified and addressed by affordable programmes suitable for specific cultural settings. Acute respiratory infections (ARI) and diarrhoeal diseases are still the major causes of morbidity and mortality among children under- five in developing countries(4). Identifying determinants of increased under-five morbidity due to ARI and diarrhoea is, therefore, likely to explain much of the overall morbidity in this age group. The present study was designed in preparation for an intervention study on ARI, which is on-going. This paper presents an analysis of child health, nutritional and obstetric determinants of under-five morbidity, controlling for public health determinants as previously described (5). Methods The study was conducted within the Butajira Rural Health project (BRHP), in southern central Ethiopia, 130 km from Addis Ababa. The BRHP demographic database covers nine Peasant ______________________________________ 1 From the Ethio-Swedish Children's Hospital, Dept. of Paediatrics and Child Health, Addis Ababa University, P.O. Box 1768, Addis Ababa, Ethiopia, 2Nottingham School of Public Health, Queen's Medical Centre, Nottingham NG7 2UH, United Kingdom, 3Department of Medical Microbiology & Immunology, University of Göteborg, Guldhedsgatan 10, 41346 Göteborg, Sweden, 4Department of Epidemiology and Public Health, University of Umeå, S-901 85 Umeå, Sweden Behavioural determinants of morbidity 77 ──────────────────────────────────────────────────────────── Associations (PA) in the Butajira District and one Urban Dwellers' Association (UDA) in Butajira town, a sample previously selected using probabilities proportional to size (6). The possibility of identifying a sufficient number of cases of acute lower respiratory infections (ALRI) for studies of risk factors and outcome was one of the considerations in determining the sample size for the morbidity study. The details of the study setting and methods were described in a previous report (5). A cohort of 1,315 under-five children were followed by a means of weekly home visits, together with the use of a recall card, over a period of one year. The recall card was a simple calendar with a photograph of the child, on which mothers recording perceived illness day by day. The weekly interviews covered symptoms and signs as perceived by mothers, together with a few clinical observations made by the field workers, who had had meticulous training and practice for 3 months. The results were used to define derived disease entities like diarrhoea and ARI. Data on birth weight, gestational age and other reproductive variables, immunization breast supplementary feeding and parental health care seeking behaviour were collected at the beginning of the study for most children, and at the time of enrollment for in-migrants and newbirths during the course of the study. A postulated conceptual model of health and behavioural factors leading to increased morbidity is shown in Figure 1. Episodes of illness were defined as previously described (5) and calculated for each child under surveillance. Individual episode counts and durations of surveillance were used as outcome variables. Results Risk factor and morbidity data were available for 1,304 children, the majority of whom were under surveillance for a complete year. Table 1 shows bivariate morbidity rate ratios for overall illness for each of the risk factors assessed. These are grouped into child health, obstetric and nutritional factors respectively. On the basis of the bivariate ratios, each factor was dichotomised, and a within-group rate ratio for each factor, adjusted for all other factors in the group, is also shown in Table 1. Figure 1: Conceptual model of health and behavioural factors contributing to childhood morbidity Individual risk indices for child health, obstetric and nutritional factors were calculated using the group rate ratios from Table 1. In general missing data were taken to have no effect on an individual index. All the individual indices were then grouped into quartiles. Table 2 shows Poisson regression 78 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── models of adjusted rate ratios for illness, gastroenteritis and ARI against these indices, after adjusting for age and sex, and for the area, environmental and parental factors previously established (5). It was shown that child care factors were significantly related to diarrhoea while nutritional factors were related to ARI. Nearly all the children in the study (99.4%) were given breast milk from birth (Figure 2). At four months of age, only 0.8% of these had stopped breast feeding. The median age at which breast feeding stopped was 27 months. A rigorous assessment of the impact of breast feeding on morbidity could not therefore be made. The possibly deleterious effect on morbidity in the period immediately following weaning was however investigated. Children who had stopped breast feeding in the 6-month period before the study started were not, however, found to be at higher risk of illness (Table 2). Figure 2: Practice of breast feeding in Butajira, Ethiopia, by age Discussion Nutrition has been shown to be a critical determinant of immunocompetence and risk of illness (7). Breast feeding has been shown to have protective, and the prevalence of breast feeding remains high in many communities in developing countries (8-10). We found that nearly all infants here were breast fed for at least 12 months. In western Ethiopia, Ketsela showed a significant reduction in diarrhoea prevalence among exclusively breast fed infants (11). Brown and Black have shown that diarrhoea and ARI prevalence rates were twice as high among infants on breast milk plus other fluids, as compared with exclusive breast feeding (12). In this study, various supplementary foods tended to reduce morbidity, particularly for children who were given meat, protein, fruit and vegetables. In a community such as this, where breast feeding is almost universal, appropriate health education messages should perhaps concentrate on the timely introduction of supplementary foods together with continued breast feeding. Children taken to a public health service facility showed slightly lower morbidity rates compared with those who used a local pharmacy, community health agent (CHA) or a traditional herbalist. Too few children claimed to have consulted CHAs or traditional practitioner for detailed analysis. Less than half of the respondents had sought medical help from the local health facilities, perhaps a reflection on the poor standards of service available there. Mothers were asked to assess the birth weight of their children as small, big or normal. Although this is a rather crude and unvalidated assessment of low birth weight, those children said to have been small at birth showed higher morbidity rates. A similar division into babies born at full term and those said by the mother to be at least 4 weeks early showed that these ‘premature’ babies were at a higher risk of morbidity compared to the full term births. However, when all these obstetric factors were assessed on a multivariate basis, the effects were not significant. Other studies have shown that low Behavioural determinants of morbidity 79 ──────────────────────────────────────────────────────────── birth weight children have more chronic conditions, more hospitalizations for repeated illnesses, more limitations on activity, poorer health status as perceived by parents and more school days lost (13-16). Premature and low birth weight infants have also been shown to a greater relative risk of lethal and potentially lethal illnesses compared to full term and normal birth weight babies (7) (relative risk 11.1 and 3.2, respectively). Hakulinen found intrauterine growth retardation rather than low birth weight to be associated with increased hospitalization (18). Birth order and variables associated with antenatal care and delivery did not influence subsequent morbidity independently of other variables in this study. However, a number of studies have suggested an increased subsequent morbidity among firstborn babies (19). The 6.7% of children born in the Health centre showed higher subsequent morbidity, but the very low number of Health Centre deliveries suggests that this group may be highly self-selected for complications and difficulties. The increased morbidity is thus likely to be a reflection of delivery complications. When both parents are present and involved in caring for their child, this study shows a beneficial effect on morbidity as compared to 80 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── Table 1: Illness rate for child health care, obstetric and nutritional factors in a one-year prospective study of morbidity among 1,304 rural Ethiopian children aged under 5 Child Health care factors Health care source n Bivariate risk Group risk Health unit Health agent 581 22 1.000 1.218 1.000 Pharmacy 534 1.218 1.135 Traditional 20 1.166 Parents Both presen One or neither 1102 162 1.000 0.905 Sleeping With adults 126 1.000 Alone 1.000 1.065 51 1.050 1.000 With family 1002 1.327 1.252 Immunization Full Partial None 347 298 620 1.000 1.891 1.734 1.000 Sunshine Exposed Not exposed 818 456 1.000 1.071 1.000 1.120 1 2-5 6+ 130 672 502 1.000 1.124 1.082 1.000 Ante-natal care Yes No 536 758 1.000 1.373 1.000 1.369 Place of delivery Health Center Home 87 1204 1.000 1.130 1.000 1.119 Delivery problem Yes No 271 1015 1.000 0.977 1.000 1.042 Birth weight Normal Lareg 900 133 1.000 1.070 1.000 Small 214 1.237 1.153 Full >1 month early 1223 68 1.000 1.622 1.000 1.625 No Yes No Yes 1150 154 497 716 1.000 0.748 1.000 0.804 1.000 0.854 1.000 0.805 Formula milk No Yes 931 61 1.000 0.612 1.000 0.726 ‘Faffa’* No Yes 924 112 1.000 0.751 1.000 0.906 Cereal No Yes 472 680 1.000 0.802 1.000 0.913 Meat No Yes 746 319 1.000 0.643 1.000 0.883 Vegetable protein No Yes 614 459 1.000 0.648 1.000 0.964 Obstetric factors Birth order Gestation Nutritional factors Breast feeding Stopped <6 months Cows’ milk 1.864 1.122 Behavioural determinants of morbidity 81 ──────────────────────────────────────────────────────────── Fruit and vegetables No Yes * Local porridge given to young children. 711 351 1.000 0.608 1.000 0.709 Table 2: Adjusted rate ratios for episodes of illness, acute respiratory infections (ARI) and gastroenteritis, based on individual risk factors from Table 1 and adusted for age, sex, area, environmental and parental factors (Ref. 5), among 1,304 rural Ethiopian Children aged under 5. Interquartile ranges (IQR) of index values and 95% confidence intervals of adusted rate ratios are shown in parentheses Index Child health factors Obstetric factors Nutritional factor Quartile 0 (1.0-1.5) (IQR) Illness 1.000 ARI 1.000 Gastroenteritis 1 (1.5-2.4) 1.121 (0.989-1.271) 0.950 (0.795-1.135) 1.000 2 (2.4-2.8) 3 (2.8-3.2) 0 (1.0-1-3) 1.066 (0.936-1.215) 1.204 1.049-1.381) 1.000 0.840 (0.698-1.011) 0.937 (0.772-1.138) 1.000 1.261 (1.054-1.509) 1.208 1.004-1.454) 1.284 (1.053-1.566) 1 (1.3-1.7) 0.988 (0.887-1.113) 0.965 (0.808-1.1154) 1.000 2 (1.7-1.7) 3 (1.7-3.4) 0 (0.2-0.6) 0.878 (0.772-0.997) 1.068 (0.948-1.204) 1.000 0.869 (0.720-1.049) 1.207 (1.015-1.434) 1.000 0.922 (0.782-1.088) 0.854 (0.714-1.022) 0.965 (0.817-1.140) 1 (0.6-0.7) 1.034 (0.912-1.171) 1.421 (1.176-1.761) 1.000 2 (0.7-0.9) 3 (0.9-1.0) 1.157 (1.023-1.308) 1.341 (1.180-1.523) 1.398 (1.155-1.693) 1.768 (1.456-2.147) 1.018 (0.849-1.220) 1.166 (0.976-1.393) children missing one or both parents, emphasising the necessity of care in protecting children from illness. Children sleeping with adults rather than with the wider family also seemed to be protected from illness. As expected, fully immunized children were at lower risk, though it is possible this may reflect the caring characteristics of parents who take their children for regular immunization, rather than being a direct effect of the immunizations. Conclusion We have shown that increased morbidity in young children in this community is significantly related to a selection of child care and nutritional factors. Improving understanding of patterns of morbidity, the extent of individual variation, and associated risk factors is crucially important for the effective planning and delivery of appropriate health services. Our previous paper showed that parental, hygiene and environmental factors were very important determinants of morbidity(5), but these factors are difficult to intervene against except on a long term and intensive basis, with full community involvement. However, this paper shows that even after controlling for those factors, a considerable part of variation in morbidity can still be explained by various factors relating to care of the individual child. The fact that 27% of the children had been fully immunized suggests a lack of impact of the preventive and health education services in the area, something which could be immediately acted upon. These results therefore emphasize the urgent need for improved outreach, both in curative and 82 Ethiop.J.Health Dev. ──────────────────────────────────────────────────────────── preventive programmes, in the health service provision for rural Ethiopia. Acknowledgements We acknowledge the financial support of the Swedish Agency for Research in Developing Countries (SAREC) and the Ethiopain Science and Technology Commission (ESTC). We also acknowledge the hard work put by the Field Supervisor of BRHP, Mr Yemiru Teka and the field workers. The massive data entry required for this study would not have been possible without the help of Mr Kidanemariam Woldeyesus. The participation in planning the study of Dr Ingela Krantz and Mr Göran Lönnberg and help and advice received from Dr Sandy Gove of the WHO CDR/ARI programme were also invaluable. References 1. The Cebu Study Team. Underlyimg and proximate determinants of child care: the Cebu longitudinal health and nutrition study. Am J Epidemiol 1991;133:185-201. 2. Tupasi, TE, Velmonte MA, Sanvictores MEG et al. Determinants of morbidity and mortality due to acute respiratory infections: implications for intervention. The Journal of infectious diseases,1988;157(4):615-23. 3. Adedoyin, MA, Watts, SJ. Child health and child care in Okelele: an indigenous area of the city of Ilorin, Nigeria. Social science and medicine, 1989;29:1333-41. 4. World Health Organization. Sixth programme report 1992-93. Programme for the control of acute respiratory infections. WHO/ARI/94.33, WHO, Geneva, 1994. 5. Muhe L, Byass, P, Freij, L, Wall S. A one -year community study on under-fives in rural Ethiopia: Patterns of morbidity and public health risk factors. Public Health 1995;109:99-109. 6. Shamebo, D., Sandström, A., Wall, S. Epidemiological surveillance for health research and intervention in primary health care. Scandinavian Journal of Primary Health Care, 1992;10, 198-205. 7. Chandra RK. Nutrition regulation of immunity and risk of illness. Indian J Paediatr 1989;56:60711. 8. World Health Organization. Report of the WHO collaborative study on breast feeding. WHO, Geneva, 1981. 9. Victora CG et al. Evidence for protection by breast feeding against infant deaths from infectious diseases in Brazil. Lancet 1987;II:319-322. 10. Tadesse E. National breast feeding Survey in Ethiopia:knowledge, attitudes and practices among mothers and health professionals. Ministry of Health and UNICEF. Addis Ababa, 1993. 11. Ketsela T, Asfaw M, Kebede D. Patterns of breast feeding in western Ethiopia and their relationship in acute diarrhoea in infants. J Trop Med Hyg 1990;36:180-3. 12. Brown KH. Infant feeding practices and their relationship with diarrhoeal and other diseases in Iluascar(Lima). Paediatrics 1989;83:31-40. 13. Overpeck MO, Moss AJ, Hoffman HJ, Heidershot GE. A comparison of the childhood health status of normal birth weight and low birth weight infants. Public Health Reports 1989;104:8-70. 14. McCormick MC. The contribution of low birth weight to infant mortality and childhood morbidity. N Eng J Med 1985;312:82-90. 15. Tammela OK. First year infections after initial hospitalization in low birth weight infants with or without bronchopulmonary dysplasia. Scand J Infect Dis 1992;24:515-24. 16. Tafari N. Low birth weight: an overview in advances in international maternal and child health. In An Overview in Advances in International Maternal and Child Health, DB Jelliffe and EEP Jelliffe, Eds. New York 1974. 17. Bartellett AV, Paz-de-Bocaletti ME. Neonatal and early post-neonatal morbidity and mortality in a rural Guatemalan community: the importance of infectious diseases and their management. Paediatr Infect Dis J 1991;10:752-57. Behavioural determinants of morbidity 83 ──────────────────────────────────────────────────────────── 18. Hakulinen A, Heinonen K, Jokela V, Launiala K. Prematurity associated morbidity during the first two years of life. A population-based study. Acta Paediatr Scand 1988;77:340-48. 19. Van Den Bosch WJ, Huygen FJ, Van den hoogen HJ, Van Weel C. Morbidity in early childhood, sex differences, birth order and social class. Scand J Prim Health Care 1992;10:118-23.
 0
0
advertisement


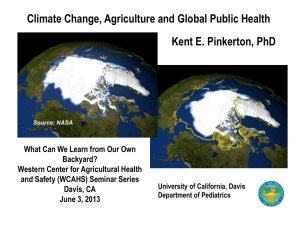




Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users