Sympathetic nerve blocks
advertisement

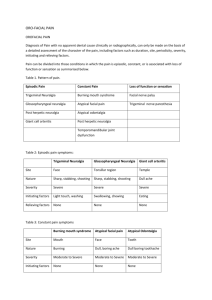
Sympathetic nerve blocks are not commonly performed. They are useful for Complex Regional Pain Syndrome (formerly known as RSD) as diagnostic and potentially therapeutic. Most sympathetic nerve blocks performed at Medical Associates are for tailbone pain or trigeminal neuralgia. Sympathetic nerves that can be targeted include: Sphenopalatine- for atypical facial pain. Similar to trigeminal neuralgia, this stabbing, burning pain in the face can be intermittent or constant with a prolonged course. The procedure uses a sterile cotton tipped applicator (Q-Tip) and a catheter to anesthetize a nerve behind the throat. The Q-Tip goes into a nostril and touches the back of the throat. If it sounds uncomfortable it is, but it is not painful and I have done it on myself. Go watch the video to see how it is done. I have several patients trained to do the procedure at home. Gasserian- for trigeminal neuralgia or atypical facial pain. This is a procedure done under light sedation. A needle is placed an inch to the side of the mouth and advanced to behind the eye into the edge of the brain. It has been performed for over 100 years using various techniques. Stellate- for arm pain related to CRPS. A needle is guided from the front of the neck to touch down on the spine at C6-7. Local anesthetic turns off the sympathetic nerves to the arm. The procedure is felt useful only if a patient has acute or subacute CRPS and is not tolerating PT. Celiac- for chronic abdominal pain. The needle starts in the back next to the spine and is placed in front of the large vessels in front of the spine. The needle starts off like an epidural and misses the spine to turn off the sympathetic nerves in front of the spine. Lumbar plexus- for leg pain related to CRPS. Same as above but instead of going at the level just under the ribs, it is performed at L2-3. GRC- for chronic lumbar disk pain. The sympathetic nerves next to L2 are turned off. 60-78% of patients get good short term relief. If effective and pain returns, RF ablation can be performed to reduce disk pain long term. http://www.ncbi.nlm.nih.gov/pubmed/14668658 http://www.ncbi.nlm.nih.gov/pubmed/16850044 Superior hypogastric plexus- for chronic pelvic pain. Typically done if there are adhesions from prior pelvic surgeries. Ask your Gynecologist or Urologist for a referral. Impar- for tailbone pain- chronic pain of the tailbone after a fracture or torn sacrococcygeal ligament. Removing the tailbone surgically is not usually effective, but turning off the nerve to the tailbone is a simple, easy, and reliable way to make this pain better.