CRPS Images - CatsTCMNotes
advertisement

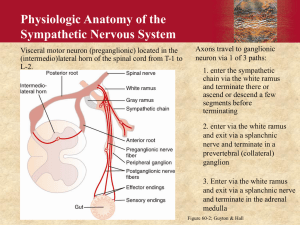
CRPS Images Complex Regional Pain Syndromes (CRPS) Definition of CRPS Type I a syndrome initiating noxious event not limited to the distribution of a single peripheral nerve disproportionate to the inciting event associated with edema, vasomotor, sudomotor, allodynia, and hyperalgesia in the region of pain 2 Causes Trauma sprain, strain, dislocation, fracture, laceration, contusion, crush injury, surgery, manipulation, tight cast, occupational repetitive trauma Disease intracerebral, intraspinal, nerve roots, ami, infection( joint, skin, periarticular), peripheral vascular Idiopathic ( about 1/3rd of all the cases) 3 Epidemiology Onset 9 – 85 years of age Median 42 years Women 3x > men Veldman PH, Reynen HM, Arntz IE: Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet 1993 Oct 23; 342(8878): 1012-6 4 Modified from Blumberg, J. Auton. Nerv. Sys. 1983 5 Pathophysiology Sympathetically maintained pain sympatholytic therapy abolishes pain and hyperalgesia sympatholytic blockade followed by administration of adrenoceptor agonists, rekindles pain distal electrical stimulation of a freshly cut sympathetic nerve induced pain in a patient with sympathetically maintained pain 6 Pathophysiology(continued) Ghostine et al - ephaptic transmission erosion of nerve insulation -> abnormal internerve communication short circuiting between somatic afferents and sympathetic efferents Bennett (NIH) - sprouting of damaged nerves sensitive to norepinephrine will discharge upon exposure to norepinephrine sympathetic fibers as a source of norepinephrine produce norepinephrine receptors at damaged ends nociceptors in intact nerves fire more in response to norepinephrine 7 Pathophysiology(continued) Schwartzman et al. - autoimmune etiology tissue injury -> nerve growth factor release -> activation of sympathetic neurons -> recruitment of neutrophils/monocytes -> complement activation -> interleukin 2 Roberts - sensitization of intraspinal wide dynamic range (WDR) neurons C fiber nociception A fiber mechanoreceptor sympathetic efferents C fiber blockade fails alleviation of SMP mechanoreceptor response to sympathetic activity 8 Thalamus Sympathetics WDR Neurons A Fiber Receptor C Fiber Receptor 9 Pathophysiology(continued) Sympathetic postganglionic neuron/afferent neuron coupling direct noradrenergic coupling within traumatized nerve within dorsal root ganglion via microvascular bed indirect noradrenergic coupling ephaptic coupling ? Abnormal inflammatory response 10 CLINICAL HISTORY ANTECEDENT TRAUMA WHEN WHERE TYPE SEVERITY NERVE INVOLVEMENT 11 CLINICAL HISTORY (CONTINUED) PAIN BURNING, ACHING, THROBBING, STINGING, CONTINUOS WITH EXACERBATIONS, “EXCRUTIATING”, “UNBEARABLE” SYMPATHETIC PAIN: CONSTANT, SPONTANEOUS, WORSE AT NIGHT, WORSE WITH MOVEMENT, TACTILE AND THERMAL STIMULI IMMEDIATE OR DELAYED ONSET(WEEKS), GRADUAL INCREASE IN INTENSITY PROPENSITY TO DIFFUSE, IPSILATERAL/CONTRALATERAL LIMB INVOLVEMENT 12 CLINICAL HISTORY (CONTINUED) INITIAL DESCRIPTION OF PAIN ADEQUACY OF TREATMENT CHANGE IN CHARACTER/INTENSITY IMMOBILIZATION HOW LONG, TO WHAT EXTENT HAS THE PRECIPITATING FACTOR RESOLVED? VASOMOTOR CHANGES? SUDOMOTOR CHANGES? 13 CLINICAL HISTORY(CONTINUED) TROPHIC CHANGES? PSYCHOLOGICAL COMPONENT? LITIGATION? PAST MEDICAL HISTORY SYMPATHOLYTC MEDICATIONS FACTORS LIMITING PHYSICAL ACTIVITY NICOTINE, CAFFEINE 14 PHYSICAL EXAMINATION COMPLETE GENERAL EXAM CARDIOPULMONARY VASCULAR NEUROLOGIC MUSCULOSKELETAL GENERAL APPEARANCE AFFECT, MOOD APPREHENSION, PROTECTIVE AND PAIN BEHAVIORS 15 PHYSICAL EXAMINATION AFFECTED LIMB SYMMETRICAL VISUAL INSPECTION PALPATION MOTOR/SENSORY EXAM 16 PHYSICAL EXAMINATION OF THE AFFECTED LIMB VISUAL INSPECTION SWELLING DISCOLORATION (ERYTHEMA, PALLOR, BLUISH MOTTLING, BRAWNY EDEMA) HYPERHIDROSIS MUSCLE WASTING POSTURING JOINT ABNORMALITY EVIDENCE OF TRAUMA 17 PHYSICAL EXAMINATION OF THE AFFECTED LIMB skin thickening, wrinkling, flaking skin thinning, smoothing, tightening, shining hair coarsening, lengthening, increase in distribution nail thickening, ridging, weakening with accelerated growth, growth asymmetry arthritic appearing joints 18 Physical Examination: Palpation Affected Limb allodynia hyperesthesia hyperalgesia warmth coolness sweaty coarse skin 19 Physical Examination: Motor & Sensory Exam Affected Limb weakness tremor fine motor movement decreased AROM/PROM allodynia hyperesthesia hyperalgesia Unaffected Areas neck/shoulder stiffness trapezial spasm with shoulder elevation and loss of motion altered gait with subsequent hip and back pain 20 Diagnostic Tests Sensory Von Frey hairs, brush hairs, feather Sudomotor ninhydrine sweat test, skin conductance response, cobalt blue test Swelling tape measure water displacement Joint mobility goniometer 21 Diagnostic Tests Psychological External Motor Behavior (ADL, disability) Visual Analogue Scale McGill pain questionnaire Minnesota Multiphasic Personality Inventory (MMPI) chronic pain profile organic vs. nonorganic patient 22 Diagnostic Tests Psychological Illness Behavior Questionnaire general hypochondria illness conviction psychological/somatic perception emotional inhibition dysphoria rejection irritability Depression and Anxiety Tests 23 Treatment Overview Prevention Early Diagnosis Physical Therapeutics Pharmacological Therapeutics Psychological Therapy Prevention of Late Complications Outcome Measurement 24 Treatment: Prevention high risk patient trauma cva nerve injury early mobilization AROM/PROM Braus patents with stroke and hemiplegia early PT 27% to 8% incidence of CRPS Type I 25 Treatment: Early Diagnosis improved outcome high degree of suspicion early treatment 26 Treatment: Physical Therapeutics elevation compression heat/cold tens/ultrasound stretching/AROM/PROM stress loading exercise(active/passive) 27 Treatment: Pharmacological Therapeutics Components of Pain inflammatory neuropathic sympathetic central nervous system 28 Treatment: Pharmacological Therapeutics Inflammatory Component NSAIDS central effect of prostaglandins IM/IV RB toradol - one study with good effect early phase intervention Prednisone - early phase intervention efficacy comparable to sympatholytics 1 mg/kg (up to 100 mg/day), 2 week taper membrane stabilizing effects binding to lamina III and VII 29 Treatment: Pharmacological Therapeutics Neuropathic Component anticonconvulsants - disappointing tricyclics - paucity of trials gabapentin - at least one study: highly effective CNS Component opioids TCAs anticonvulsants NSAIDs, steroids 30 Treatment: Pharmacological Therapeutics Calcitonin ? mechanism of action in CRPS I moderate efficacy in some studies 31 Treatment: Surgical Intervention Chemical Sympathectomy phenol, alcohol longer than sympathetic blockade pain recurs Radiofrequency Sympathectomy Endoscopic-guided Sympathectomy Open Surgical Sympathectomy Results: 12-90% efficacy 30% recurrence Complications: sympathalgia in 7-44% of patients 32 Treatment: Prevention of Late Complications muscle atrophy/weakness osteoporosis contractures pain 33 A 29-year-old woman with reflex sympathetic dystrophy in the right foot demonstrates discoloration of the skin and marked allodynia. 34 This photo shows the same patient as in the above image, following a right lumbar sympathetic block. Marked increase in the temperature of the right foot is noted, with more than 50% pain relief. 35 A 68-year-old woman with complex regional pain syndrome type II (causalgia). 36 A 36-year-old woman with right arm reflex sympathetic dystrophy and dystonic posture (movement disorder). 37 Normal laser Doppler study of the upper extremities. When the patient performs inspiratory gasp repeatedly during laser Doppler image acquisition, the transient capillary flow decreases are displayed easily and dramatically (as dark bands) in the pseudocolor image. 38 Laser Doppler study of the upper extremities in a patient with right hand reflex sympathetic dystrophy. 39 Laser Doppler study of the lower extremities in a 25year-old woman with reflex sympathetic dystrophy in the right foot. 40