Sample
advertisement

Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 1 of 14, 3 Figure(s), 4 Table(s)
ESSENTIAL MATHEMATICS FOR GAMES
Core Mathematics
Paul Robertson
4
Section A
1 Blood disorders
2 Dermatology
3 The eye and external adenexa
4 The head and neck
Section B
5 The respiratory system
6 The cardiovascular system
7 The gastrointestinal system
000
000
000
000
000
000
000
PART OUTLINE HEAD
Sect title
Sect Subtitle
Sect Author
4
1 Blood disorders
2 Dermatology
3 The eye and external adenexa
4 The head and neck
5 The respiratory system
6 The cardiovascular system
7 The gastrointestinal system
8 The respiratory system
000
000
000
000
000
000
000
000
SECT OUTLINE HEAD
CHAPTER 214
Management of the Spastic Hand
ANN VAN HEEST, MD JAMES HOUSE, MD
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 2 of 14, 3 Figure(s), 4 Table(s)
OVERVIEW OF HAND SPASTICITY
ANALYSIS OF SPASTICITY IN THE HAND
TREATMENT GOALS
SURGICAL PRINCIPLES
Wrist Flexion Deformity
Thumb-in-Palm Deformity
Finger Swan-Neck Deformity
Authors' Preferred Method
COMPLICATIONS AND THEIR MANAGEMENT
OUTCOMES OF TREATMENT
OVERVIEW OF HAND SPASTICITY
Chapter Heading – Management of Spastic Hand
Molecules can be categorised as inorganic or organic based on their elemental
composition. Carbon-hydrogen bonds define molecules as organic.
Hand spasticity is a disorder most commonly seen in association with traumatic
brain injury, cerebral vascular injury, cervical spine injury, and cerebral palsy.
Glossary or Keywords
Europe the model is a coherent view of capital markets data that allows users to interact with the
content in a consistent manner.
Primates regardless of the source. Essentially, of sources. Properly deployed.
Europe model is a coherent view of capital markets data that allows users to interact with the
content in a consistent manner.
Relative size
Acquirer’s valuation
Primates regardless of the source. Essentially, it of sources. Properly deployed, such a framework can be used to remove, conceptually consistent view.
Heading within Glossary
Europe model is a coherent view of capital markets data that allows users to interact with the
content in a consistent manner.
Primates regardless of the source. Essentially, it of sources. Properly deployed.
Key points
Molecules can be categorised as inorganic or organic based on their elemental composition.
Carbon-hydrogen bonds define molecules as organic.
The simplest organic molecules are hydrocarbons which contain only carbon and hydrogen
atoms.
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 3 of 14, 3 Figure(s), 4 Table(s)
Alkanes are saturated hydrocarbons, alkenes have one or more double bonds and alkynes have
one or more triple bonds.
Alicyclic compounds have carbon atoms linked in cyclic structures.
Aromatic compounds contain one or more benzene rings.
Functional groups are added to hydrocarbon skeletons to give biologically functional molecules.
Many hydrocarbons have multiple isomeric forms.
Elements cannot be broken down into other substances by chemical reactions.
A compound is made from two or more elements which are combined in a fixed ratio.
ABSTRACT
This chapter explores some of the theories on the mechanism of action of reflexology,
particularly relating them to physiological actions and effects, and considering currently
available research that may support these theories.
Hand spasticity is a disorder most commonly seen in association with traumatic brain injury,
cerebral vascular injury, cervical spine injury, and cerebral palsy. All of these disorders have in
common a central nervous system injury causing an upper motor neuron paresis or palsy. In an
upper motor neuron disorder, the normal inhibitory control of tone is lost, and the resultant
peripheral manifestation is spasticity. Muscle spasticity causes imbalance across joints with
resultant loss of function. Cerebral palsy has the added complexity that the central nervous
system injury occurs in the perinatal period, so that the effect of spasticity on the immature
skeleton must be considered as well.
In the upper extremity, the typical pattern of spastic joint posturing includes shoulder internal
rotation, elbow flexion, forearm pronation, wrist flexion and ulnar deviation, thumb-in-palm, and
finger swan-neck or clenched fist deformities (Fig. 214-1). Although this pattern of deformity is
the most common, the particular pattern and severity are individual to each patient on the basis
of the extent and area of the underlying central nervous system disorder.
Spasticity in the hand does not occur as an isolated problem. Motor involvement can take the
form of spasticity (increased tone), flaccidity (decreased tone), or athetosis (lack of or poor
control of tone). The interplay of these various types of motor involvement is an important part
of defining the problem. In evaluating a particular joint deformity, several forces often work
together to exacerbate the joint deformity (Fig. 214-2). For example, in a wrist flexion/ulnar
deviation deformity, the deformity can be due primarily to spasticity of the flexor carpi ulnaris
muscle. However, weakness or flaccidity of the extensor carpi radialis longus and brevis muscles
can exacerbate the wrist flexion/ulnar deviation deformity because there is no active antagonist
(extension/radial deviation) to the spastic flexor carpi ulnaris (flexor/ulnar deviation). The
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 4 of 14, 3 Figure(s), 4 Table(s)
spasticity of the agonist (in this example, the flexor carpi ulnaris) as well as the strength and
control of the antagonist (in this example, the extensor carpi radialis longus and brevis) must be
assessed to evaluate the problem accurately.
Several disease processes that involve upper motor neuron lesions due to brain dysfunction are
considered together because they have a single final common pathway: spasticity in the hand
(Fig. 214-3). Traumatic brain injury is the most commonly seen in patients younger than 40
years and is typically secondary to motor vehicle accidents. Major return of function can occur
up to 18 months after traumatic brain injury with cognitive improvements during many years
after the injury.1 Cerebral vascular accidents affect 1 in 1000 individuals per year; spastic
hemiplegia is the most common sequela for the surviving patients. This is because the middle
cerebral artery is the most commonly involved vessel, with resultant sensory and motor system
dysfunction. Cerebral palsy is most commonly secondary to ischemic central nervous system
injuries occurring in the perinatal period. This is most commonly associated with low birth
weight with prematurity, anoxic events, or cerebral vascular bleeds or emboli. The incidence is
0.2% (2 children per 1000 live births), increasing to 10% in the premature, low-birth-weight
child.
Spasticity of the hand is not the only manifestation of these central nervous system disorders.
The pattern of musculoskeletal spasticity is classified by the limb or limbs involved: monoplegia
(one limb), hemiplegia (one arm and one leg), diplegia (two legs), triplegia (one arm and two
legs), and quadriplegia (all four extremities).
All individuals who present with spasticity in the hand need a further evaluation of their
central nervous system. If a child first presents to the hand surgeon, identification is most
commonly around 1 year of age because of delayed development of normal pinch and grasp
function. In this scenario, a complete neurologic evaluation is necessary, including evaluation of
the lower extremities, before a diagnosis of cerebral palsy can be made. In most other scenarios,
the hand surgeon is consulted for management of hand spasticity after the initial central nervous
system lesion has been diagnosed. The hand surgeon must continue to work with the
rehabilitation physicians and neurologists, as well as with any physicians who may be involved
in lower extremity care, to maintain a multispecialty approach that appropriately coordinates
services for the patient. Associated issues can include mental retardation, seizures, and speech
disorders as well as lower extremity involvement that affects mobility.
In this chapter, the focus is on spastic hemiplegia secondary to cerebral palsy as the most
common form of spasticity of the hand. Similar principles can be applied to other causes of hand
spasticity as well.
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 5 of 14, 3 Figure(s), 4 Table(s)
ANALYSIS OF SPASTICITY IN THE HAND
Assessment of the patient with spastic cerebral palsy starts with the history and physical
examination. Because cerebral palsy is associated with low birth weight and prematurity,
associated medical problems should be noted, particularly seizures and mental retardation as
indicators of more global central nervous system involvement. Developmental motor delays
should be assessed. Children with spastic hemiplegia most commonly will show premature hand
dominance, favoring the unaffected side even as young as 6 months. Delay of normal pinch and
grasp function patterning at 1 year of age is evident. Overall use of the upper extremity should be
characterized both from the history obtained from the parents and by the physician's direct
observation. Overall upper extremity function in cerebral palsy is most commonly classified by a
nine-level grading system (Table 214-1). General categories include the following: does not use;
passive assist (poor, fair, or good); active assist (poor, fair, or good); and spontaneous use
(partial or complete). Agreement with the parents on the child's present overall level of limb
function lays the groundwork against which outcome of subsequent treatments can be compared.
TREATMENT GOALS
Treatment of the hand dysfunction centers on improving muscle balance to maximize hand
function consistent with the quality of voluntary control retained. The primary lesion in the brain
is not treated and remains the limiting factor to the success of the surgery.
SURGICAL PRINCIPLES
Surgical procedures to satisfy these treatment goals follow specific surgical principles (Table
214-3) to be described as they apply to wrist flexion deformity, thumb-in-palm deformity, and
finger swan-neck deformity. A vast array of options exist for the surgeon treating the wrist,
thumb, and fingers and a constellation of associated deformities (Table 214-4).
MUSCLE CONTRACTURE
Muscle tone is noted through the passive evaluation of joint mobility. Passive range of motion
needs to be done slowly to overcome muscle spasticity with gentle sustained resistance.
Assessment for muscle and joint contracture is performed by passive mobility of the joint and
passive stretch of the muscle. If there is a loss of range of motion at both the finger and wrist
joints unaffected by change in position of the wrist, both muscle and joint contractures are
present. If there is full passive mobility of the joints and muscle, no contracture exists. If there is
muscle contracture without joint contracture, this can be elicited by testing the effect of joint
motion on a biarticular muscle such as the finger flexors. The finger flexor muscles are
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 6 of 14, 3 Figure(s), 4 Table(s)
biarticular muscles, meaning they cross over more than one joint (the wrist joint and the finger
joints). Thus, positioning of the wrist joint in flexion allows full finger extension if there is no
finger joint contracture; but positioning of the wrist joint in extension will not allow full finger
extension if there is finger flexor muscle contracture. This is analogous to the intrinsic tightness
test. This is commonly graded as described by Zancolli (Table 214-2).2
EVALUATION OF PATIENTS
Appropriate consultation or multispecialty approach to care should be instituted before
surgical intervention is considered. Several alternatives to surgical intervention exist.
Consideration of the treatment pros and cons may require discussions that include the
rehabilitation physicians, neurologists, and neurosurgeons to adequately explore the options of
tone-reducing medications (diazepam, baclofen), tone-reducing injections (botulinum toxin,
phenol), tone-reducing neurosurgery interventions (selective dorsal rhizotomy), and therapy
interventions (splinting, stretching programs).
PHYSICAL EXAMINATION
If physical examination reveals a joint or muscle contracture, particularly in a hemiplegic
patient or in a patient with isolated problems to the upper extremity, initial treatment includes
splinting, stretching, and therapy interventions. Electrical stimulation of the antagonist muscles
has been advocated in the upper extremity of patients with cerebral palsy, but lasting outcomes
and improved function have not been reported.4
What muscles are spastic and causing joint imbalance leading to limb dysfunction?
What muscles are under good voluntary control and are available for tendon transfer?
How old is the patient?
What is this patient's overall limb function as classified by House? (see Table 214-1)
The muscles with good voluntary control are best for good results with tendon transfer.
Is there significant athetosis or incoordination?
Wrist Flexion Deformity
1. Release or lengthen the spastic muscle or muscles:
Fractional lengthening of the flexor carpi ulnaris or flexor carpi radialis
Flexor pronator slide
2. Augment the weak or flaccid muscle (tendon transfers):
Brachioradialis to extensor carpi radialis brevis
Extensor carpi ulnaris to extensor carpi radialis brevis
Flexor carpi ulnaris to extensor carpi radialis brevis
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 7 of 14, 3 Figure(s), 4 Table(s)
Flexor carpi ulnaris to extensor digitorum communis (if finger extension is inadequate)
In some cases, the wrist flexion deformity is more severe, and the principal wrist extensor
muscles are not functional. This may be evident on physical examination, or it may require use
of a diagnostic motor nerve block or a diagnostic botulinum toxin injection to temporarily
weaken the spastic wrist flexor, most commonly the flexor carpi ulnaris, to assess the patient's
cortical control for wrist extension.
3. Stabilize the joint for severe instability or contracture:
Proximal row carpectomy
Wrist fusion
1. Release or lengthen the spastic muscle or muscles:
Adductor pollicis
Flexor pollicis brevis
Flexor pollicis longus
If the primary deformity is adduction of the first metacarpal, without significant
metacarpophalangeal or interphalangeal joint deformity, the primary deforming force is the
adductor pollicis. Treatment includes a partial tenotomy or myotomy near its insertion (often in
conjunction with a first web Z-plasty for individuals with concomitant skin contracture) or a
release of its origin off the third metacarpal as described by Matev.18
<Begin Equation>
{concentration}hexane
= constant
{concentration}water
</End Equation>
The constant is usually called P and is known as the partition coefficient. It is usual to divide
the concentration in the organic solvent by the concentration in the water, so that if P>1 the
solute favours the organic solvent. Since P varies for common compounds over at least 10 orders
of magnitude it is normal to use log P, which thus can range from +5 to 5 and occasionally
more. The value of log P, which is an equilibrium constant, gives valuable insight into the
properties of the molecule and has been used in drug design for many years as a descriptive
parameter.
<Author text type A>
if(Read_buffer[0] == ‘P’ && Read_
buffer[1] == ‘=’ &&
Read_buffer[2] == ‘?’ &&
Read_Buffer[3] == ‘?’)
{
TRISB = 0xFF;
Write_buffer[0] = ‘P’;
Write_buffer[1] = ‘=’;
Write_buffer[2] = PORTB;
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 8 of 14, 3 Figure(s), 4 Table(s)
Write_buffer[3] = ‘T’;
Hid_Write(&Write_buffer,4);
</Author text type A>
Authors' Preferred Method
This example describes the authors' preferred methods of evaluation, treatment, surgical
technique, and postoperative care. Note that the joints can be evaluated separately for treatment
options, with a final reconstructive treatment plan synthesizing the complexities of the entire
upper limb deformity.
COMPLICATIONS AND THEIR MANAGEMENT
Balance is the key, and it can be difficult to obtain. Overcorrection is due to excessively tight
tendon transfers or excessive release (instead of lengthening) of spastic muscles and should be
avoided through careful preoperative planning and attention to surgical technique. A key surgical
principle is to leave an option to reverse the surgical correction if this is possible.
Undercorrection occurs in the circumstances of release without concomitant tendon transfer,
insufficient release, and undertensioned tendon transfers. If the initial procedure has resulted in
undercorrection of the deformity, undercorrection is easier to manage with a subsequent
additional procedure to obtain balance.
CONCLUSION
In the above worked example, we can see that an understanding of pregnancy physiology, an
awareness of potential pathology and knowledge of the research on the effects of reflexology can
be applied to the treatment of a pregnant client with backache, offering safe, appropriate and
evidence-based therapy. If the practitioner wished to consider treatment of a woman with nausea
associated with medical interventions for breast cancer, it would be necessary to be cognisant of
the pathology of tumours developing in the breast, possible complications and routes by which
the disease could spread and conventional medical treatments and their effects. This knowledge
would then need to be applied to the reflexology treatment of the client, taking into account our
contemporary understanding of reflexology and its mechanism of action. Similar exercises could
be undertaken for treating other clients, both those seeking treatment for general health and wellbeing, and those with more specific pathological conditions.
Acknowledgments
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 9 of 14, 3 Figure(s), 4 Table(s)
The result of this approach is to produce a top-down view of tIt is a framework that
standardizes the manner in which organizations can refer to complex data content, thereby
reducing the efficiency. It can be applied as and when needed so that new systems take on a
standard.
REFERENCES
1. Teasdale G, Skene A, Parker L, Jennett B: Age and outcome of severe head injury. Acta
Neurochir Suppl Wien 1979;28:140-143.
2. Zancolli EA, Zancolli ERJ: Surgical management of the hemiplegic spastic hand in cerebral
palsy. Surg Clin North Am 1981;61:395.
3. Loewen P, Steinbok P, Holsti L, MacKay M: Upper extremity performance and self-care skill
changes in children with spastic cerebral palsy following selective posterior rhizotomy.
Pediatr Neurosurg 1998;29:191-198.
4. Carmick J: Clinical use of neuromuscular electrical stimulation for children with cerebral
palsy. Part II: upper extremity. Phys Ther 1993;73:514-527.
5. Hines AE, Crago PE, Villian C: Functional electrical stimulation for reduction of spasticity in
the hemiplegic hand. Biomed Sci Instrum 1993;29:259-266.
6. Keenan MAE, Thomas E, Stone L: Percutaneous phenol block of musculocutaneous deformity
in cerebral palsy. J Bone Joint Surg Am 1990;15:236.
7. Braun RM, Hoffer MM, Mooney V, et al: Phenol nerve block in the treatment of acquired
spastic hemiplegia in the upper limb. J Bone Joint Surg Am 1973;55:580-585.
8. Wall SA, Chait LA, Temlett JA, et al: Botulinum A chemodenervation: a new modality in
cerebral palsied hands. Br J Plast Surg 1993;46:703.
9. Van Heest AE: Applications of botulinum toxin in orthopaedics and upper extremity surgery.
Techniques Hand Upper Extremity Surg 1997;1:27-34.
10. Goldner JL, Koman LA, Gelberman R, et al: Arthrodesis of the metacarpophalangeal joint of
the thumb in children and adults: adjunctive treatment of thumb-in-palm deformity in cerebral
palsy. Clin Orthop 1990;253:75-89.
11. Manske PR, Strecker WB: Cerebral palsy, stroke, brain injury. In Peimer CA, ed. Surgery of
the Hand and Upper Extremity. New York, McGraw-Hill, 1995:1517.
12. Waters PM, Van Heest A: Spastic hemiplegia of the upper extremity in children. Hand Clin
1998;14:119-134.
13. Inglis AE, Cooper W: Release of the flexor-pronator origin for flexion deformities of the
hand and wrist in spastic paralysis. J Bone Joint Surg Am 1966;48:847-857.
14. White WF: Flexor muscle slide in the spastic hand: the Max Page operation. J Bone Joint
Surg Br 1972;54:453-459.
15. House JH, Gwathmey FW: Flexor carpi ulnaris and the brachioradialis as a wrist extension
transfer in cerebral palsy. Minn Med 1978;61:481-484.
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 10 of 14, 3 Figure(s), 4 Table(s)
16. McCue FC, Honner R, Chapman WC: Transfer of the brachioradialis for hands deformed by
cerebral palsy. J Bone Joint Surg Am 1970;52:1171-1180.
17. Green WT: Tendon transplantation of the flexor carpi ulnaris for pronation-flexion deformity
of the wrist. Surg Gynecol Obstet 1942;75:337-342.
18. Matev I: Surgical treatment of spastic "thumb-in-palm" deformity. J Bone Joint Surg Br
1963;45:703-708.
19. Manske PR: Redirection of extensor pollicis longus in the treatment of spastic thumb-in-palm
deformity. J Hand Surg Am 1985;10:553.
20. Filler BC, Stark HH, Boyes JH: Capsulodesis of the metacarpophalangeal joint of the thumb
in children with cerebral palsy. J Bone Joint Surg Am 1976;58:667-670.
21. Smith RJ: Flexor pollicis longus abductor-platy for spastic thumb-in-palm deformity. J Hand
Surg Am 1982;7:327.
22. Littler JW: The finger extensor mechanism. Surg Clin North Am 1967;47:415-432.
23. Van Heest A: Lateral band re-routing in the treatment of swan-neck deformities due to
cerebral palsy. Techniques Hand Upper Extremity Surg 1997;1:***
24. Tonkin MA, Hughes J, Smith KL: Lateral band translocation for swan-neck deformity. J
Hand Surg Am 1992;17:260-267.
25. Swanson AB: Surgery of the hand in cerebral palsy and the swan neck deformity. J Bone
Joint Surg Am 1960;42:951-964.
26. Thometz JG, Tachdjian MO: Long-term follow-up of the flexor carpi ulnaris transfer in
spastic hemiplegic children. J Pediatr Orthop 1988;8:407.
27. House J, Gwathmey F, Fidler M: A dynamic approach to the thumb-in-palm deformity in
cerebral palsy. J Bone Joint Surg Am 1981;63:216-225.
28. Van Heest AE, House JH, Cariello C: Upper extremity surgical treatment of cerebral palsy. J
Hand Surgery Am 1999;24:323-330.
29. Mital MA: Lengthening of the elbow flexors in cerebral palsy. J Bone Joint Surg Am
1979;61:515-522.
30. Strecker WB, Emanuel JP, Dailey L, Manske PR: Comparison of pronator tenotomy and
pronator rerouting in children with spastic cerebral palsy. J Hand Surg Am 1988;13:540-543.
31. Zancolli EA: Structural and Dynamic Bases of Hand Surgery, 2nd ed. Philadelphia, JB
Lippincott, 1968.
32. Sakellarides HT, Mital MA, Lenzi WD: Treatment of pronation contractures of the forearm
in cerebral palsy by changing the insertion of the pronator radii teres. J Bone Joint Surg Am
1981;63:645-652.
33. Green WT, Banks HH: Flexor carpi ulnaris transplant and its use in cerebral palsy. J Bone
Joint Surg Am 1962;44:1343-4352.
34. Omer GE, Capen DA: Proximal row carpectomy with muscle transfers for spastic paralysis. J
Hand Surg Am 1976;1:197-204.
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 11 of 14, 3 Figure(s), 4 Table(s)
FURTHER READING
Cohen M, Kemper K 2005 Complementary therapies in pediatrics: a legal perspective. Pediatrics
115(3): 774–780 (doi:10.1542/peds.2004–1093).
http://pediatrics.aappublications.org/cgi/content/full/115/3/774 accessed 19 September 2009.
Heller T, Lee-Treweek G, Katz J, Stone J, Spurr S (eds) 2005 Perspectives on complementary
and alternative medicine. London: Open University Press and Routledge.
Lee-Treweek G, Heller T, MacQueen H, Stone J, Spurr S (eds) 2005 Complementary and
alternative medicine: structures and safeguards. London: Open University Press and
Routledge.
Hope T, Savalescu J, Hendrick J 2008 Medical ethics and the law. The core curriculum. 2nd edn.
London: Churchill Livingstone.
<B type A>
Box 5.1
The Model for Structured Reflection (Edition 15a)
Reflective cue
Bring the mind home
Focus on a description of an experience that seems significant in some way (story/video etc)
What particular issues seem significant to pay attention to?
How were others feeling and why did they feel that way? (empathy)
How was I feeling and what made me feel that way? (sympathy)
What was I trying to achieve and did I respond effectively?
What were the consequences of my actions on the patient, others and myself?
What factors influence the way I was/am feeling, thinking and responding to this situation?
What knowledge did or might have informed me?
To what extent did I act for the best and in tune with my values?
How does this situation connect with previous experiences?
How might I reframe the situation and respond more effectively given this situation again?
What would be the consequences of alternative actions for the patient, others and myself?
What factors might constrain me responding in new ways?
How do I NOW feel about this experience?
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 12 of 14, 3 Figure(s), 4 Table(s)
Am I more able to support myself and others better as a consequence?
What insights do I draw from this experience?
Am I more able to realise desirable practice? (framing perspectives)
3.1 Authors' Preferred Method
Author Insight
This example describes the authors' preferred methods of evaluation, treatment, surgical
technique, and postoperative care. Note that the joints can be evaluated separately for treatment
options, with a final reconstructive treatment plan synthesizing the complexities of the entire
upper limb deformity.
At her thumb, the adductor is spastic, the extensor pollicis brevis and abductor pollicis longus
are poorly controlled, and the metacarpophalangeal joint is unstable. By application of the
surgical principles outlined before, we recommended
a partial adductor pollicis tenotomy (to weaken the spastic muscle);
a volar metacarpophalangeal joint capsulodesis (to stabilize the severely unstable joint).
Similarly at her wrist, the flexor carpi ulnaris is spastic, the extensor carpi radialis brevis/longus is poorly
controlled, and the wrist joint is subtle. Diagnostic testing would be performed by injection of botulinum toxin into
the flexor carpi ulnaris to better test voluntary control of the extensor carpi radialis brevis/longus as an antagonist to
the flexor carpi ulnaris muscle when it is less spastic. If findings indicate that the patient has no extensor carpi
radialis brevis/longus control despite diminished flexor carpi ulnaris spasticity, on application of the surgical
principles outlined before we would recommend
fractional lengthening of the flexor carpi ulnaris (to weaken the spastic muscle);
a tendon transfer into the extensor carpi radialis brevis; and
no joint stabilizations necessary.
Finger Swan-Neck Deformity
1. Release or lengthen the spastic muscle or muscles:
Intrinsic slide
Ulnar motor neurectomy
For patients with mild swan-neck deformity secondary to intrinsic spasticity, an intrinsic slide
procedure has been described to lengthen these muscles by use of two dorsal incisions to elevate
and slide the interossei origins.
2. Augment the weak or flaccid muscle (tendon transfers):
Lateral band rerouting
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 213 Tables (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 13 of 14, 3 Figure(s), 4 Table(s)
Rerouting
<T type A>
TABLE 214-1
UPPER EXTREMITY FUNCTIONAL USE CLASSIFICATION
0
1
2
3
Class
Designation
Does not use
Poor passive assist
Fair passive assist
Good passive assist
4
5
6
Poor active assist
Fair active assist
Good active assist
7
Spontaneous use, partial
8
Spontaneous use, complete
Activity Level
Does not use
Uses as stabilizing weight only
Can hold onto object placed in hand
Can hold onto object and stabilize it for use by other
hand
Can actively grasp object and hold it weakly
Can actively grasp object and stabilize it well
Can actively grasp object and then manipulate it
against other hand
Can perform bimanual activities easily and
occasionally uses the hand spontaneously
Uses hand completely independently without reference
to the other hand
<T type A>
TABLE 214-2
ZANCOLLLI ASSESSMENT OF WRIST FUNCTION
Group 1
Complete extension of the fingers with neutral extension of the wrist
Group 2
Finger extension with wrist flexion
Subgroup a: Active extension of the wrist with the fingers flexed
Subgroup b: No active extension of the wrist with the fingers flexed
Group 3
No active extension of the fingers even with maximal wrist flexion
<T type A>
TABLE 214-3
SURGICAL TREATMENT PRINCIPLES
1. Release or lengthen the spastic or contracted muscles.
2. Augment the weak or flaccid muscles.
3. Stabilize the joint for severe joint instability or severe joint contractures.
Mathes & Hentz, 2/e, ISBN 0-7216-8811-X
Chapter 214 (edited file)—"Management of the Spastic Hand"
2/5/2016, Page 14 of 14, 3 Figure(s), 4 Table(s), 0 Box(es)
FIGURE 214-1.
Typical spastic hemiplegic posturing in the upper extremity includes shoulder internal rotation,
elbow flexion, forearm pronation, wrist flexion and ulnar deviation, thumb-in-palm, and
clenched fist deformities.
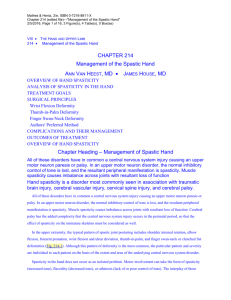
FIGURE 214-2.
A, Normal anatomy of proximal interphalangeal joint extensors in the dorsal and lateral view.
The extrinsic finger extensors (EDC, EDQ, EIP) divide over the proximal phalanx to form the
central slip and two lateral bands. The finger intrinsics are the interossei and the lumbricals. The
intrinsics join the extrinsic lateral band to form the conjoined lateral band, commonly referred to
as the lateral band. In the normal state, dorsal subluxation of the lateral band is prevented by the
volar tethering effect of the transverse retinacular ligament. B, Muscle imbalance causing joint
deformity. Joint deformity occurs secondary to muscle imbalance. In the wrist joint, the wrist
extensors are often flaccid with poor rotational control, whereas the wrist flexors are often
spastic, causing wrist flexion deformity.
FIGURE 214-3.
Sequence of events leading to limb dysfunction. Surgical treatment can address joint deformity
and dysfunction at the shoulder, elbow, forearm, wrist, thumb, and fingers.