Elbow & Wrist
advertisement

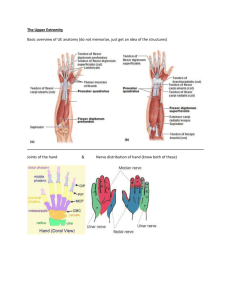
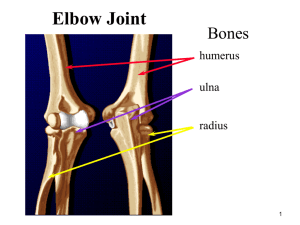
ESS 303 – Biomechanics Elbow & Wrist Anterior View 3 2 Middle phalanx 1 Posterior View 4 5 The Elbow Joint Articulation between humerus and ulna Flexion: limited by coronoid fossa and coronoid process contact Extension: limited by olecranon fossa and olecranon process contact Stable compared to shoulder – bony structure Head of radius moves along capitulum Radioulnar Joint 3 articulations Proximal or superior (by the elbow joint) Middle Distal or inferior (by the wrist joint) Bony arrangements give virtually no stability – ligament support Movements: pronation and supination The Wrist Joint Technically 2 joints Proximal or radiocarpal Ellipsoidal Flexion Extension Abduction (radial flexion or radial deviation) Adduction (ulnar flexion or ulnar deviation) Circumduction Distal radiocarpal or midcarpal joint The Wrist Joint The primary function of the wrist muscles is to provide a stable base for the hand, while permitting postural adjustments that provide optimal length-tension in the long finger muscles Tennis Elbow and Carpal Tunnel Syndrome (CTS) Tennis Elbow Tennis Elbow Lateral epicondylitis Wrist extensors attach to a single tendon at the lateral epicondyle of the humerus May be caused by any activity in which you grasp an object while your wrist is extended or by lifting heavy objects with your elbow locked and your arm extended Common in people over 30. Most common in Caucasian men 30 to 60 years old who work with their hands Tennis Elbow – RX Rest (or stop) until the pain disappears Massage Exercise to strengthen and prevent reinjury Warm up & stretching before activity Take frequent breaks Medical: Anti-inflammatory drugs and surgery CTS Median Nerve Transverse Carpal Ligament CTS Basics The carpal tunnel is a bony canal within the palm side aspect of the wrist that allows for the passage of the median nerve to the hand Pinching or compression of the median nerve (compression neuropathy) by the transverse carpal ligament sets into motion a progressively crippling disorder which eventually results in wrist pain, numbness and tingling in the hand, pain consisting of a “pins and needles” feeling at night, weakness in grip and loss of coordination Who Gets CTS? Women more than men – ratio of 3 to 1 Usually between the ages of 30 and 50 Seen more frequently in people who tend to do forceful repetitive types of work, such as grocery store checkers, assembly line workers, meat packers, typist, accountants, writers, etc. CTS - RX Early stage: modification in activities, a removable wrist brace, and anti-inflammatory medicines Moderate stages, especially if numbness and pain continues: cortisone injection into the carpal tunnel or surgery (if other treatments have failed) Advanced stages, especially with profound weakness or muscle atrophy: surgery Untreated can cause permanent nerve damage Movements and Major Muscles Elbow Flexion: biceps brachii, brachialis & brachioradialis Extension: triceps brachii & anoneus Radioulnar Pronation: pronator quadratus Supination: supinator Movements and Major Muscles Wrist Flexion: flexor carpi radialis, flexor carpi unlaris, pulmaris longus, flexor digitorum superficialis & flexor digitorum profundus Extension: extensor carpi radialis longus, extensor carpi radialis brevis & extensor carpi unlaris Abduction (also called radial deviation or radial flexion): flexor carpi radialis Adduction (also called ulnar deviation or ulnar flexion): flexor carpi unlaris Circumduction: combination of above