ppt - Stewart Morrison
advertisement

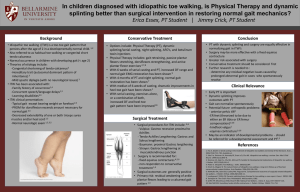
Orthopaedic Considerations in Cerebral Palsy Stewart Morrison Western Health Friday Presentation 20th January 2012 Definition + Aetiology “a disorder of movement and posture due to a defect or lesion in the developing brain” Not a diagnosis, but a heterogenous collection of clinical syndromes Cerebral lesion is static, musculoskeletal pathology is progressive Prenatal Perinatal Postnatal placenta insufficiency, toxins, genetic factors, TORCH premature delivery, hypoxia, infection, kernicterus, haemolytic disease infection, trauma Classification Type of Motor Disorder Limbs Involved Spastic Athetoid Ataxis Rigid + Mixed Monoplegia Hemiplegia Diplegia Triplegia Quadriplegia pyramidal system (motor cortex) extrapyramidal (basal ganglia) cerebellum + brainstem basal ganglia + motor cortex one limb (rare) one side lower limbs, assymetrically three limbs (rare) four limbs Demographics Two per 1000 live births 50% have normal intelligence, 25% able to self-support as adult Incidence remains static +/- increasing Clinical Features I Dependent on: I.Severity of neurological lesion II.Location of neurological lesion III.Age of child ✚Absence of normal reflexes (blinking, sucking) ✚Persistence of abnormal reflexes (Moro’s reflex) ✚Delayed motor milestones (head control 3 months, sitting 6 months, walking 12 months) ✚Gait disturbance ✚Epilepsy, speech and hearing difficulties, visual defects, feeding difficulties, drooling, learning, behavioural problems Clinical Features II Posturing Gait Neuromuscular Deformities sitting (hypotonic slump) standing (crouchposture, spastic posture, pelvic obliquity, loss of lumb. Lordosis) athetoid or ataxic movement UMN or spastic paresis resistance to passive movement Babinski +ve Equinus FFD Knee Pathology I Skeletal muscle growth depends on regular stretching of relaxed muscle, under physiological loading In CP: ✚ Muscle does not relax (spasticity) ✚ Reduced activity (weakness + balance) Pathology II I. Dynamic Contractures II. Muscle Contractures III. Secondary Bone Changes correctable deformity fixed deformity e.g. medial femoral torsion, lateral tibial torsion Management Concepts Limitations ✚ Treating the sequelae of a neurological lesion, not the lesion itself ✚ Many of the operations were developed for the management of polio myelitis Stage I Stage II Stage III Physiotherapy, Orthotics, Botulinum Toxin, Selective Posterior Rhizotomy Timing critical and controversial Unpredictable results Staged vs. single procedures Correctional osteotomies for torsional + joint deformities Tendon Transfer: Principles ✚ ✚ ✚ ✚ ✚ ✚ ✚ Correct joint contractures muscle of adequate strength muscle of adequate excursion one tendon for one function an expendable donor a straight line of pull Position and time transfers so that they lie in tissue of optimal condition Lower Extremity I Age of surgery critical ✚ Gait evolves into adult pattern by age seven years ✚ Gait deterioration during adolescence is quite common Preoperative evaluation ✚ Multiple joint evaluation required ✚ Eg. TA correction in presence of tight hamstrings will result in persistent crouch at knee and calcaneus gait ✚ Gait Analysis critical ✚ Swing-phase foot clearance, foot progression angle Lower Extremity II Hemiplegia Group I Group II Group III Group IV mild foot-drop gait equinus gait Knee, medial hamstrings, quadricepts involvement Hip flexion, medial torsion Spastic Diplegia leaf-spring AFO stretching casts, botulinum toxin, AFO, lengthening gastroc recession, medial hamstring lengthening, distal rectus femoris transfer lengthening psoas, external rotation osteotomy, and above Most achieve good function Hip flexors, adductors, medial rotators, calf most affected Secondary bone torsional problems Lower Extremity III Lengthening Achilles Tendon overused “a little equinus is better than calcaneus” ? Silveskiod Test (Gastroc vs. Soleus) Gastrocnemius Recession Z Lengthening or Percutaneous Techniques Varus Deformity of the Foot Tib Post usually resonsible (stance and swing) Tib Ant (swing only) Lengthening vs. transfer Valgus Deformity Lengthening, Fusion, Osteotomies Lower Extremity IV Knee Flexion Contracture “crouch” Surgical lengthening of medial hamstrings consideration of NV bundle in severe contracture Stiff-Knee Gait may occur if rectus femoris co-spasticity Rectus Femoris transfer indicated Hip Flexion Contractures often secondary to knee/ankle issues Thomas or Staheli tests Psoas lengthening Lower Extremity V Hip Subluxation Rotational Osteotomies Hip Reconstructive Surgery (spastic quadriplegia) Upper Extremity Evaluation ✚ Sensation ✚ Electromyography Principles ✚ Define goals ✚ Restore ✚ Rebalance Upper Extremity Shoulder ✚ Internal rotation, adduction common Botulinium type A Supscapularis, Pec Major lengthening External rotational osteotomy Elbow ✚ Static and dynamic flexion contractures flexor release dependent on NV bundle Wrist/Digits ✚ Wrist flexion +/- pronation, ulnar deviation lengthening and transfer procedures Thank you BARCZYNSKI, A., PASIERBEK, M., GAZDZIK, T. S. & KLOSA, Z. 2002. Management of foot deformity in cerebral palsy. Ortop Traumatol Rehabil, 4, 21-6. GRAHAM, H. K. 2005. Classifying cerebral palsy. J Pediatr Orthop, 25, 127-8. KAROL, L. A. 2004. Surgical management of the lower extremity in ambulatory children with cerebral palsy. J Am Acad Orthop Surg, 12, 196-203. GRAHAM, H. K. 2003. Musculoskeletal Aspects of Cerebral Palsy. Journ. Bone & Joint Surgery (British). 85-B, 2:157 SAEED, W. R. 2003. Cerebral Palsy of the Upper Extremity: A Surgical Perspective. Current Orthopaedics. 17:105-116