Surgically treated patients, especially those with cerebellar
advertisement

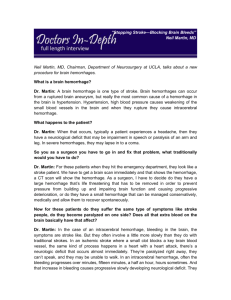
EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Salama & Kelany MINI-CRANIECTOMY FOR EVACUATION OF HYPERTENSIVE SUPRATENTORIAL INTRACEREBRAL HEMATOMA By Hosni H, Salama* and Atef Kelany** Department of Neurosurgery, *El-Minia and **Zagazig University ABSTRACT: Background: Surgical treatment of intracerebral hematoma (ICH) is rarely indicated, yet there is a need to clarify the benefits of this approach. Aim of the work: :is to evaluate the clinical outcome in patients harboring large superficial hypertensive ICH treated by minicraniectomy. Patients and methods: 18 patients harboring large superficial hypertensive ICH are evaluated clinically and radiologically, and subjected to minicrniectomy and followed to determine if there is clinical success or not. Results: There was 10 males and 8 females, aged ranged from 53-76 years with a mean of 62 years. Preoperative (Glasgow Coma Score) GCS was 3-8 in two cases, 912 in 14 cases, and from 13-15 in two cases. Amount of preoperative midline shift was 1-3 mm in two cases, 3-6 mm in 8 cases, and 6-10 mm in 8 cases. Postoperative GCS was 3-8 in two cases, 9-12 in 6 cases, and 13-15 in 8 cases. There was mortality of two cases due to chest infection. After 6 months using (Glasgow Outcome Score)GOS there was 8 cases of good outcome (good recovery and moderate disability) and 8 cases bad outcome (severe disability or vegetative) Conclusion: Minicrniectomy may be a useful approach for treating large superficial hypertensive-based ICH. KEY WORDS: Intracerebral hematoma Surgical treatment Follow up. Abbreviations: ICH= Intracerebral hematoma, GCS = Glasgow Coma Score, GOS = Glasgow Outcome Score, ICP= Intracranial pressure.CAA=Cerebral amyloid angiopathy. modifiable risk factor for spontaneous intracerebral hematoma (SICH). Although definitive evidence favoring surgical intervention is lacking, there is good theoretical rationale for early surgical intervention3. The question of appropriate indications for surgical removal of ICHs is being intensively debated in the literature at present4,5,6. Various surgical approaches have been described to evacuate large, hypertension-based ICHs, including craniotomy and transcortical,7,8 9 transsylvian, and transcallosal10 approaches. Simple aspiration of ICH INTRODUCTION: Although intracranial hemorrhage accounts for approximately 10 to 15% of all cases of stroke, it is associated with a high mortality rate1. Despite major advances in brainimaging examination procedures, improvements in neurosurgical critical care, and refinements in microsurgical techniques, only a few subgroups of patients with spontaneous intracerebral hematomas are usually listed as candidates for surgical treatment in the reported series2. Hypertension, however, remains the single greatest 138 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 through a burr hole is relatively noninvasive and associated with lower morbidity than craniotomy. However, early series reported poor localization of the hematoma and inadequate removal11. Salama & Kelany Anesthesia; Local anesthesia at the site of craniectomy about 5 cm in diameter using 15 cc xylocaine 2% diluted 1:1 with saline starting perpendicular to the bone and reaching it to inject subperiosteally then subgaleal and subcutaneous. In some patients who could move during surgery IV drip of Dormicum as sedation may be used. In addition, stereotactic aspiration with or without the use of fibrinolytic agents12,13,14 has also been described. Finally, many surgeons have used endoscopic instrumentation to evacuate large ICHs15. Technique: A vertical incision at the site of the planned craniectomy and within the area locally infiltrated, is used. Periosteal incision and elevation is done to expose the site of craniectomy. Burr hole is done using the Hudson manual drill till reaching the dura then widening of the hole is done using bone rongeures and kerrisons for a diameter about 3 cm .After exposure of the dura a mini dural flap is done using dural knife and scissors.Corticotomy at the site of the maximum thickness of the hematoma is done using bipolar coagulation. Advancement of small patties through this corticotomy till the hematoma is reached. Self retaining nasal speculum or spatulas using Yasergil retractors may be used. Suction of the hematoma is started with the aid of the tumor forceps to remove the unsucable clots and the use of continuous irrigation by saline and the use of bipolar coagulation if there is oozing from the bed of the hematoma is used until the hematoa is mostly removed. Sometimes a small part at the bottom of the cavity is left not to open an already closed source of bleeding. Covering the wall by Surgicel is done, leaving intracavitary catheter 8 G drain then closure of dura, periosteum, galea and skin. PATIENTS AND METHODS: Our study included 18 patients presenting with spontaneous supratentorial intracerebral hematoma in patients known as hypertensive or discovered accidentally after stroke as hypertensive patients. All patients were admitted to El-Minia and Zagazig university hospitals to the stroke unit, and after a request from neurologists we evaluated them radiologically and clinically and categorized them as surgical candidates according to the following criteria; 1) size, diameter more than 3 cm. 2) site, superficially located not more than 2 cm in depth from the cortex. 3) symptomatizing as a cause of increased ICP (evidenced by midline shift radiologically and disturbed conscious level clinically). Most of these patients are old ages, hypertensives, comatosed so they are not fit for general anesthesia. Positioning; All patients were operated in the supine position with tilt of the head so that the site of hematoma is the highest part with elevation of the head to reduce venous congestion and increased ICP.The head is fixed using adhesive tape fixation to the head rest. Postoperatively: The patient is put under continuous observation with maintenance of antiepileptic drugs, 139 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 dehydrating measures, antibiotics and anti hypertensive drugs. Follow up CT brain is done within the first week to verify the amount of decompression and the severity of midline shift. The Salama & Kelany catheter is removed in the third postoperative day. Clinical evaluation using GCS in the early stages and GOS after 6 months was done. A B A) Preoperative large left temporal intracerebral hematoma. B) Immediate postoperative CT showing nearly complete evacuation of the hematoma. C D C) superficial large left parieto-occipital hematoma with midline shift. D) right occipital large superficial intracerebral hematoma. using minicraniectomy. The results were as the following; There was 10 males (55%) and 8 females (45%), aged ranged from 5376 years with a mean of 62 years, hypertension was present in all cases, RESULTS: Eighteen patients having spontaneous supratentorial intracerebral hematoma and fulfilling the criteria of surgery were operated upon 140 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 preoperative GCS was 3-8 in two cases (11%), 9-12 in 14 cases (78%), and from 13-15 in 2 cases (11%). Amount of preoperative midline shift was 1-3 mm in two cases (11%), 3-6 mm in 8 cases (44.5%), and 6-10 mm in 8 cases (44.5%). Postoperative GCS was 3-8 in two cases (11%), 9-12 in 6 cases Salama & Kelany (33%), and 13-15 in 8 cases (44%). There was two cases mortality (11%) due to chest infection. After 6 months using GOS there was 8 cases (44%) of good outcome (good recovery and moderate disability) and 8 cases (44%) bad outcome (severe disability or vegetative). Table (1): Preoperative GCS. GCS Number of patients 3-8 2 (11%) 9-12 14 (78%) 13-15 2(11%) Table (2): Amount of preoperative midline shift on CT. Amount of midline shift Number of patients 1-3 mm 2 (11%) 3-6 mm 8 (44.5%) 6-10 mm 8 (44.5%) Table (3): Postoperative GCS Postoperative GCS Number of patients 3-8 2 (11%) 9-12 6 (33%) 13-15 8 (44%) surgery itself 11, these goals are adequately fulfilled by our approach. DISCUSSION: The indication for surgical therapy for brain hemorrhage continue to be modified, Although clear-cut indications are not yet available for all patients, clinical and CT guidelines for therapy have been proposed16. Regarding the choice of the patients for surgery our study included patients harboring large hematoma >3cm , this is agreed by most neurosurgeons who operate on large hematoma either by using the diameter17 or the volume 3080 ml18. Donan and Davis 20034 consider evacuations in younger patients with moderately sized lobar hematomas who are not comatose, but are clinically deteriorating, we operate in comatosed patients with GCS not less than 5 because we consider that reduction of ICP is the main aim of the surgery. A retrospective review of lobar brain hemorrhage by Radberg and colleagues 199119 showed that regardless of treatment all patients with hematoma volume of greater than 80 ml died, and all patients with hematoma volume less than 30 ml survived. Nath et al., 198620, determined that a hematoma could produce ischemic changes in the surrounding brain, without affecting cerebral perfusion pressure, which could be severe and were proportional The ideal goals of surgical treatment of ICH should be to remove as much blood clot as possible as quickly as possible with the least amount of brain trauma from the 141 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 to the volume of hematoma, which suggests that removal of even small hematomas could result in improvement in the microcirculation of the surrounding brain. Salama & Kelany operated after 6 hours (average time interval 23 hours). Surgery can be life saving in the deteriorating patient24, while others state that deterioration itself is a bad prognostic index2. As regarding the side of the hematoma, we did not exclude any case because of is lateralization because all the hemtomas were lobar, large and near to the surface, so there was no fear of further brain damage along the very short trajectory. There was some hesitation (uncertainty between neurosurgeons about surgery on deep left sided hematomas17. Simple aspiration was abandoned before it was properly evaluated because only small amounts of clot could be removed, and it could precipitate "blind" re-bleeding25. Our study uses the minicraniectomy approach to avoid the drawbacks of simple aspiration and to take the benefits of more visualization to perform complete evacuation under vision. All our patients were having clinical and radiological evidence of increased ICP. Simply because reduction of intracranial pressure (ICP) is the main aim of surgery. Postoperatively, improvement in the clinical condition occurs in most patients as evaluated by postoperative GCS. 2 patients died, (22%), this mortality rate is better than most conservative series like Aur et al., 198926 who stated that mortality rate was 79% in conservative and 30% in surgically treated patients. Mortality rates differ in different series that is because it depends on preoperative GCS. As regards the conscious level of the patients, we operate on patients with GCS 5 to 13, this is because no benefit is expected with GCS <5 because irreversible brain stem damage already occurred and no need for reduction of ICP if it is nearly normal GCS >13 in spite of the benefit expected from hematoma removal even if the patient is conscious because this gives a chance to surrounding brain recovery. In our series ,after 6 months using GOS there was 8 cases (44%) of good outcome (good recovery and moderate disability) and 8 cases (44%) bad outcome (severe disability or vegetative). The time of operation was a matter of debate between authors. Some21 performed surgery in the first 6 hours to minimize ongoing bleeding, irritation of the brain and edema, others suggest waiting at least 6 hours to minimize the possibility of rebleeding22. Rehemorhage although uncommon typically occurs in the first 6 hours after the initial hemorrhage although significant rehemorrhage had been documented in hypertensive patients as late as 109 hours after the first ictus23. All our patients were According to a review of 35 patients who underwent neurosurgery for cerebral amyloid angiopathy related (CAA-related) ICH reported by Leblanc et al, 199127 13 (37%) died after intracerebral hematoma evacuation, and only 7 (20%) were neurologically well (good recovery or moderately disabled) postoperatively. However, many of these patients were 142 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 in a poor neurological condition preoperatively because of severe intracranial hypertension caused by the mass effect of the hematoma, and Izumihara et al., 199928 consider this to be the main reason for their poor outcome, and in his series of patients with hematomas of various sizes (10 to 130 mL), 20 (54%) had a good outcome (good recovery or moderately disabled), and only 4 (11%) died. Salama & Kelany 9) Kaya RA, Turkmenoglu O, Ziyal IM, et al., (2003): The effects on prognosis of surgical treatment of hypertensive putaminal hematomas through transsylvian transinsular approach. Surg Neurol 59:176–183, 2003 10) Kurtsoy A, Oktem IS, Koc RK, et al: Surgical treatment of thalamic hematomas via the contralateral transcallosal approach. Neurosurg Rev 24:108–113, 2001 11) Broderick JP, Adams HP Jr, Barsan W, et al., (1999): Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. A statement for healthcare professionals from a special writing group of the stroke council, American Heart Association. Stroke 30: 905–915, 1999. 12) Matsumoto K, Hondo H (1984): CT-guided stereotaxic evacuation of hypertensive intracerebral hematomas. J Neurosurg 61: 440–448 1984 13) Niizuma H, Shimizu Y, Yonemitsu T, et al., (1989): Results of stereotactic aspiration in 175 cases of putaminal hemorrhage. Neurosurgery 24:814–819, 1989 14) Teernstra OP, Evers SM, Lodder J, et al:(2003): Stereotactic treatment of intracerebral hematoma by means of a plasminogen activator: a multicenter randomized controlled trial (SICHPA). Stroke 34:968–974, 2003 15) Bakshi A, Bakshi A, and Banerji AK (2004): Neuroendoscopeassisted evacuation of large intracerebral hematomas: introduction of a new, minimally invasive technique. Preliminary report Neurosurg Focus 16 (6):e9, 2004. 16) Crowell RM,Ojeman RG, (1981): Surgery for brain hemorrhage. In Mossy J, Reinmuth OM (eds): Cerebrovascular disease. New York, Raven Press,1981, pp233-254. REFERENCES: 1) Quinones-Hinojosa A, Gulati M, Singh V, et al.(2003): Spontaneous intracerebral hemorrhage due to coagulation disorders. Neurosurg Focus. 2003 Oct 15;15(4):E3. 2) Carvi Y Nievas MN.(2005): Why, when, and how spontaneous intracerebral hematomas should be operated. Med Sci Monit 2005 Jan;11(1):RA24-31. 3) Fewel ME, Thompson BJ, Hoff JT.(2003): Spontaneous intracerebral hemorrhage: a review. Neurosurg Focus, 2003 Oct 15; 15(4):E1 4) Donnan GA, Davis SM: (2003): Surgery for intracerebral hemorrhage: an evidence-poor zone. Stroke 34:1569–1570, 2003 5) Hankey GJ: (2003): Evacuation of intracerebral hematoma is likely to be beneficial—against. Stroke 34: 1568–1569, 2003 6) Minematsu K: (2003): Evacuation of intracerebral hematoma is likely to be beneficial. Stroke 34:1567–1568, 2003 7) Morgenstern LB, Demchuk AM, Kim DH, et al., (2001): Rebleeding leads to poor outcome in ultra-early craniotomy for intracerebral hemorrhage. Neurology 56:1294–1299, 2001 8) Peresedov VV (1999): Strategy, technology, and techniques of surgical treatment of supratentorial intracerebral hematomas. Comput Aided Surg 4:50–63, 1999 143 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 17) Barbara A. Gregson and A. David Mendelow, (2003): (STITCH) International Variations in Surgical Practice for Spontaneous Intracerebral hemorrhage. Stroke 2003; 34; 25932597. 18) H. M. Fernandes, B. Gregson, S. Siddique, et al., (2000): Surgery in Intracerebral Hemorrhage. The Uncertainty Continues, Stroke. 31: 2511. 19) Radberg JA, Olsen JE, Radberg CT (1991): Prognostic parameters in spontaneous intracerebral hematomas with special reference to anticoagulant treatment.Stroke 22:571-576,1991. 20) Nath FP, Jenkins A, Mendelow AD, et al., (1986): Early hemodynamic changes in experimental intracerebral hemorrhage. J. Neurosurg. 1986; 65: 697-703 21) Kaneko M, Tanaka K, Shimada T, et al., (1983): Long-term evaluation of ultra-early operation for hypertensive intracerebral hemorrhage in 100 cases. J Neurosurg 58:838-842. 22) Kaufman HH (1996): Spontaneous Intraparenchymal Brain Hemorrhage In Neurosurgery by Wilkins RH, and Rengachary SS.2nd ed. Vol.5, Ch.254pp 2567-2585. Salama & Kelany 23) Hamilton MG, and Zabramiski JM (1997): Spontaneous Brain Hemorrhage in The Practice of Neurosurgery, 1997 By George G. Tindal, Paul R. Cooper and Daniel L. Barow Vol 5 .Ch 150, pp 2295-2312. 24) Ojeman RJ, Heros RC, and Crowell RM (1988): Surgical management of cerebrovascular disease, 2nd Ed.Ch 25, pp435-449. 25) Graeme J. Hankey (2003): Evacuation of Intracerebral Hematoma Is Likely to Be Beneficial—Against, (Stroke. 2003; 34:1568.) 26) Auer LM, Deinsberger W, Niederkorn K, et al., (1989): Endoscopic surgery versus medical treatment for spontaneous intracerebral hematomas: a randomized study. J Neurosurg 1989; 70:530-535. 27) Leblanc R, Preul M, Robitaille Y, et al., (1991): Surgical considerations in cerebral amyloid angiopathy. Neurosurgery. 1991; 29: 712–718. 28) Izumihara A, Ishihara T, Iwamoto N, et al., (1999): Postoperative Outcome of 37 Patients With Lobar Intracerebral Hemorrhage Related to Cerebral Amyloid Angiopathy (Stroke. 1999;30:29-33.) المعالجة الجراحية باستخدام تربنة صغيرة لنزيف المخ التلقائى **حسنى سالمة* و عاطف كيالنى أقسام المخ واألعصاب *كلية طب المنيا و**كلية طب الزقازيق المعالجة الجراحية باستخدام تربنة صغيرة لنزيف المخ التلقائى يشار إليهاا ناادرا رمام:الخلفية ذلك هناك حاجة لتوضيح منافع هذه الطريقة أن يقيّم النتيجة السريرية في المرضى ذوى إرتفاع ضغط د ّم باالضاافة الاى نزياف:هدف العمل .سطحي كبير عولج باستخدام فتحة تربنة صغيرة مااريذ ذوو إرتفاااع ضااغط د ّم مااع نزيااف سااطحي كبياار مق ايّم سااريريا18: المرضىىى والطىىر وبشكل إشعاعي تم فحصهم قبل وبعد اجراء جراحة تربنة لتفريغ النزيف عاماااا و76 و53 سااايداج و تاااراو السااان باااين8 حااااالج رجاااال و10 النتيجىىىة كاااان هنااااك حالاة14 و8-3 باستخدام مقياس جالسجو لقياس درجة الغيبوبة كانج هناك حالتان بدرجاة مان 12-9 حااالج مان6 و8-3 و بعد الجراحة كانج هنااك حاالتين15-13 و حالتان من12-9 من وعلى المدى الطويل كانج هناك نسبة تحسن جيدة15-13 حاالج من8و المعالجة الجراحية باستخدام تربناة صاغيرة لنزياف الماخ التلقاائى هاى طريقاة مفيادة: الملخص لعالج النزيف السطحى التلقائى فى المخ الناتج عن ارتفاع ضغط الدم 144