Please insert here the title of your abstract
advertisement

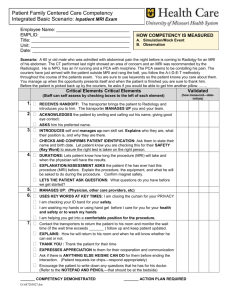
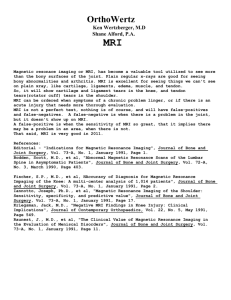
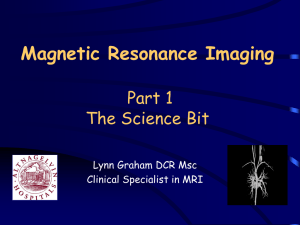
Integrating a MRI scanner with a radiotherapy accelerator: a new concept of precise on line radiotherapy guidance and treatment monitoring B.W. Raaymakers, J.J.W. Lagendijk, U.A. van der Heide, J. Overweg1, K. Brown2, R. Topolnjak, H. Dehnad, I.M. Jürgenliemk-Schulz, J. Welleweerd, C.J.G. Bakker3 Department of Radiotherapy and Radiology3, University Medical Center Utrecht, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands. Philips Research Hamburg1, Germany, Elekta2, Crawley, United Kingdom. Abstract Within a collaboration between the UMC Utrecht, Elekta and Philips Research, Hamburg, we are investigating the integration of a MRI scanner with a radiotherapy accelerator. This system must provide on-line, soft tissue based position verification, but also on line monitoring of treatment results. The technical feasibility study led to a design that will be presented in this paper. Basically the design is a single energy accelerator mounted in a ring around a conventional 1.5 T MRI scanner. Keywords Position verification, MRI, accelerator, treatment monitoring, IMRT, fiducial markers, treatment planning Introduction Precise image guided radiotherapy has to deal with the uncertainties in the exact daily positioning of the radiation fields with respect to the changing anatomy due to internal organ motion and tumour response to treatment. Huge effort is being put in the development of tumour visualisation and position verification technology. The most commonly applied technique is position verification using the megavoltage treatment beam for imaging. The image contrast however is poor and allows merely the visualisation of the bony anatomy or implanted fiducial gold markers [1,2]. Bony structures and markers may also be visualised using ceiling mounted kilovolt X-ray imaging [3]. More sophisticated are the new developments that integrate conebeam CT functionality [4] or integrate megavoltage CT with the accelerator [5]. Also the integration of ultrasound imaging with an accelerator is being investigated [6]. The excellent soft tissue contrast of MRI can be used for two, interconnected purposes, i.e. treatment guidance and treatment monitoring. If it is possible to integrate MRI functionality with a radiotherapy accelerator this may provide unequalled, on-line, soft-tissue based position verification. Besides, MRI has the potential to characterise the tumour in 3D [7]. Parameters related to blood flow, hypoxia, pH, vascularity, etc. can be measured with MRI or MR spectroscopy. New developments in this are the use of antibody or receptor specific nanosensors, contrast agents which are visible with MRI [8]. All this biological imaging can be used for achieving biological conformality [9]. Besides the expected gain on position verification of both tumour and surrounding tissues, a system that integrates MRI and an accelerator can incorporate, and contribute to, these new imaging developments. In collaboration with Elekta and Philips Research, Hamburg, we are investigating the feasibility of such an integrated MRI accelerator system. Technical feasibility and design The design of the MRI accelerator combination is basically a small accelerator mounted on a ring around a modified, Figure 1: Impression of an integrated MRI accelerator. The inner grey drum represents the MRI system, the blue ring around it contains the accelerator. closed-bore MRI system, see figure 1. The magnetic stray field potentially disturbs the operation of the accelerator. On the other hand, magnetisation of the moving accelerator components would lead to modulation of the 1.5 T magnetic field with image distortion and ghost artifacts as possible consequences. Active magnetic shielding has to be applied to magnetically uncouple the MRI system and the accelerator. In order to limit cost and complexity, we decided to base the concept on a cylindrical closed-bore main field magnet, with the accelerator irradiating the patient from outside the MRI system. This choice implies beam transmission through the MRI field generating system. The MRI magnet and the gradient coil need to be modified in order to minimise both scatter and absorption heterogeneity. Furthermore, the photon beam travels unperturbed in the magnetic field. However the actual dose deposition, an avalanche of secondary electrons, is affected by the presence of the permanent 1.5 T magnetic field. The technical feasibility study has focussed mainly on 3 topics: Magnetic interference of the MRI system and the accelerator Beam transmission through the closed bore MRI Dose deposition kernel in a 1.5 T field Main magnet. The magnetic interference is hampering the integrated system in two ways: the operation of the accelerator is distorted by the presence of the magnetic stray field. Especially the gun section with its low energy electrons before full acceleration is sensitive. On the other hand, ferromagnetic accelerator components might become magnetised and thus induce a distortion on the main magnetic field. In order to limit image distortion, the main field homogeneity has to be of the order of few ppm over the entire field of view,. In collaboration with Philips Research, modifications of the coil configuration of a standard Intera 1.5 T magnet have been investigated. The magnetic interference is minimized by active magnetic shielding. By slightly modifying the number of turns of the shield coil of a standard actively shielded magnet design, it is possible to achieve a very low field in a toroidal volume in the midplane of the MRI magnet in which the accelerator can be placed. This modification leads to a slight increase of the far field of the magnet, but the field at larger distances is still sufficiently low to allow installation in the vicinity of conventional accelerators (typically at 10 m distance). The coil configuration of the main magnet can also be modified in such a way that there are no superconducting coil windings in the transversal mid-plane of the MRI system. This means that the equivalent of approximately 6 cm (or less) of homogeneous aluminium remains in the beams eye view, significantly reducing both scatter induction and absorption heterogeneity. This modified magnet is not much different in construction, and induces no significant compromises on the central field quality, i.e. the new design would yield the same imaging performance as a standard Philips system. Gradient coil system. The magnet system, i.e. the cryostat with the superconducting coils can be adjusted to create a beam portal without compromising its performance. The remaining MRI components through which the beam travels are the gradient coils and the RF coils. The RF coils can easily be made very transparent to radiation. A conventional gradient coil however poses a severe scatter and absorption problem. Several patterns of thick copper conductors with gaps of a few mm in between are located on top of each other. When irradiating through this, intensity contrasts upto 80% at a spatial resolution of mm can be expected. Therefore also radiation portals in the gradient coils are required. Again in collaboration with Philips Research, Hamburg, the impact of a 20 cm gap in the gradient coils was investigated. For the gradient in the axial direction (Zdirection), the windings can easily be moved out of the central area. The coils for the transversal gradients (i.e. Xand Y-direction) needed significant modification, but suitable transverse coil geometries without conductors covering the central 20 cm were indeed found. Figure 2 shows magnetic field plots for a possible design. Figure 2: Gradient of the magnetic field with a 20 cm gap in the gradient coils. The left hand panel shows the transversal mid plane, gradient quality similar to a conventional coil, the right hand panel shows the sagital mid plane, in this direction the field of view is limited to 25 cm. These preliminary investigations have provided confidence that the gradient coils can be placed outside the beam’s eye view. For this preliminary design, the image quality in the transversal mid-plane will be unaffected and the field of view in the axial direction will be limited to approximately 25 cm, which is enough for this application. Beam characteristics As discussed, the beam has to travel through various structures. After modifying the magnet and gradient coils, the total amount of (homogeneous) mass in the beams’ eye view is the equivalent of approximately 10 cm Aluminium (~27 gr/cm2). This means the scatter induction at 10 cm from the border of a 10x10 cm2 field is rel. dose % approximately doubled compared to the open beam situation, as shown in figure 3. Here the scatter induction as function of mass in the beam was measured for a 10x10 cm2 field. In these measurements the mass was compressed into a single slab. The next step will be measuring the scatter induction for a range of fields in the actual MRI accelerator configuration, as well as performing Monte Carlo simulations in order to precisely quantify the scatter induction. 2,5 2 1,5 1 0,5 0 0 10 20 30 40 weight gr/cm2 Figure 3: Scatter induction as function of the amount of mass in the beam. The scatter induction is measured at 5 cm depth at 10 cm from the border of a 10x10 cm2. The scatter induction can be further reduced by limiting the system to a discrete number of gantry positions. This allows the creation of beam portals in both the carrier of the superconducting coils in the cryostat, the thermal shields and the carrier of the gradient coils. Whether this is necessary with respect to scatter induction will be further investigated. The only absorption heterogeneity is found in the RF coils, these structures represent an equivalent of approximately 2.3 cm thick aluminium, yielding maximum intensity contrasts of 25% at a spatial resolution of mm. Furthermore there is the helium level in the cryostat for specific gantry angles. A maximum of 15 cm helium can be in the beam’s eye view, leading to approximately 10% intensity contrast. Another source of heterogeneity is the omission of a flatness filter in order to minimise scatter induction and increase the accelerator output. The remaining heterogeneity can be flattened using MLC based [10] or compensator based IMRT. Dose deposition kernel The impact of the 1.5 T magnetic field on the dose deposition of a 6 MV beam was modelled using Monte Carlo simulations, see accompanying paper [11]. The conclusion is that the impact is small and can be taken into account in a conventional treatment planning procedure. The feasibility and calibration of dosimetry equipment in the presence of 1.5 T has to be studied. Technical and clinical challenges The technical feasibility of various issues has been addressed and briefly discussed. The conclusion is that integrating a MRI with an accelerator is technically feasible. Still the actual technical implementation has to be done. First, the preliminary results need further and more detailed investigation. Monte Carlo simulations will be applied for quantifying for instance the scatter induction and the dose deposition kernel in the actual MRI accelerator configuration. The way of compensating the remaining absorption heterogeneities has to be decided; MLC based IMRT versus compensators. The first option provides lower spatial resolution, the second option induces additional scatter, which can be partially dealt with by introducing additional shielding. A comparative assessment between these choices has to be made. The present design aims to keep the two systems as physically separated as possible. A dedicated ring around the MRI has to be constructed in which the accelerator can be mounted. When choosing for compensators to solve the absorption heterogeneity, their placement is a topic of study. They can be placed on the outside of the MRI system, but preferably they will be placed in between the gradient coil and the magnet, there they are positioned closely to the system’s heterogeneity (i.e. the RF coil). Conventionally here the passive shielding system is located, but this system is placed outside the central area to minimise the amount of mass in the beam. Various separate topics need to be investigated to fulfil the aim of the MRI accelerator, i.e. accurate radiation delivery at mm resolution, for instance the problem of absolute positioning. When using MRI images for treatment guidance it is crucial that the images are geometrically correct and that the exact relation between the MRI coordinate system and the accelerator coordinate system is known. At our department a full quality assurance system for correction MR images has been developed [12,13]. System dependent image distortions could be reduced from 13 mm to 2 mm and patient induced distortions could be corrected to the order of the image pixel size. These corrections and dedicated MR scanning procedures were developed explicitly for radiotherapy treatment planning purposes. This work will be continued with the aim to achieve sub-mm accuracy. The main clinical question is: what is the expected benefit for treatment outcome when using a MRI system integrated with an accelerator for daily, on-line position verification of both tumour and surrounding structures? This is being studied parallel with the development of the MRI accelerator. For this study a 1.5 T MRI radiotherapy simulation system serves for repeated, daily and continuous imaging in order to investigate daily anatomy variations [14,15]. The next step is to investigate how to handle this information. Registration with treatment planning images, on-line judgement of position accuracy and position correction and ultimately on-line re-planning are topics that need to be investigated. It is the explicit goal of these efforts to come to highly conformal, adaptive plans with the minimum feasible margins. Conclusion The feasibility of an integrated MRI accelerator system is being investigated. Preliminary results indicate that the design is feasible. Such a system will provide superb on-line position verification of both tumour and normal tissue structures and will facilitate on line treatment optimisation and treatment response monitoring. Acknowledgement [7] Stubbs M. 1999, Application of magnetic resonance techniques for imaging tumour physiology. Acta Oncol. 38, 845-853 [8] Weissleder R, Moore A, Mahmood U, Bhorade R, Benveniste H, Chiocca EA, Basilion JP. 2000, In vivo magnetic resonance imaging of transgene expression. Nat. Med. 6, 351-354 [9] Ling CC, Humm J, Larson S, Amols H, Fuks Z, Leibel S, Koutcher JA. 2000. Towards multidimensional radiotherapy (MD-CRT): biological imaging and biological conformality. Int. J. Rad. Biol. Phys. 47, 551560 [10] Topolnjak R, Van der Heide UA, Lagendijk JJW. 2004, IMRT sequencing for a six-bank multi-leaf collimator system. Submitted to 14th ICCR, Seoul, South Korea. This work is supported by a grant from the Dutch Technology Foundation STW. References [1] Gilhuijs KGA, Van de Ven PJH, Van Herk M. 1996, Automatic three-dimensional inspection of patient setup in radiation therapy using portal images, simulator images and computed tomography data. Med. Phys.23, 389-399 [2] Nederveen AJ, Lagendijk JJW, Hofman P. 2001, Feasibility of automatic marker detection with an a-Si flat-panel imager. Phys. Med. Biol. 46, 1219-1230 [3] Soete G, Verellen D, Michielsen D, Vinh-Hung V, Van der Steene J, Van den Berge D, De Roover P, Keuppens F, Storme G. 2002, Clinical use of stereoscopic X-ray positioning of patients treated with conformal radiotherapy for prostate cancer. Int. J. Rad. Biol. Phys.54, 948-952 [4] Jaffray DA, Siewerdsen JH, Wong JW, Martinez AA. 2002, Flat-panel cone-beam computed tomography for image-guided radiation therapy. Int. J. Rad. Biol. Phys.53, 1337-1349 [5] Ruchala KJ, Olivera GH, Schloesser EA, Mackie TR. 1999, Megavoltage CT on a tomotherapy system. Phys. Med. Biol. 44, 2597-2621 [6] Langen KM, Pouliot J, Anezinos RTT, Aubin M, Gottschalk AR, Hsu IC, Lowther D, Liu YM, Shinohara K, Verhey LJ, Weinberg V, Roach III M. 2003, Evaluation of ultrasound-based prostate localization for image guided radiotherapy. Int. J. Rad.Biol. Phys. 57, 635-644 [11] Raaymakers BW, Jette D, Lagendijk JJW. 2004, An integrated MRI scanner and radiotherapy accelerator: distortion of the dose deposition by the presence of a transverse magnetic field. Submitted to 14th ICCR, Seoul, South Korea [12] Moerland MA, Beersma R, Bhagwandien R, Wijrdeman HK, Bakker CJG. 1995, Analysis and correction of geometric distortions in 1.5 T magnetic resonance images for use in radiotherapy treatment planning. Phys. Med. Biol. 40, 1651-1664 [13] Bhagwandien R, Moerland MA, Bakker CJG, Beersma R, Lagendijk JJW. 1994, Numerical analysis of the magnetic field for arbritrary magnetic susceptibility distributions in 3D. Magn. Res. Imag. 12, 101-107 [14] Van der Heide UA, Van de Bunt L, De Kort GAP, Ceylan C, Ketelaars M, Jurgenliemk-Schulz IM, Lagendijk JJW. 2004, IMRT for cervix tumours: achieving and maintaining conformality. Submitted to 14th ICCR, Seoul, South Korea [15] Lagendijk JJW, Bartels LW, Dehnad H, Van Vulpen M, Van der Heide UA, Ceylan C, Seppenwoolde JH, Tersteeg JHA, Raaymakers BW. 2004 MRI based treatment planning for prostate tumours: fiducial marker based registration and position verification. Submitted to 14th ICCR, Seoul, South Korea