Squeeze Up Technique For Bleedingless Excision Of Giant
advertisement

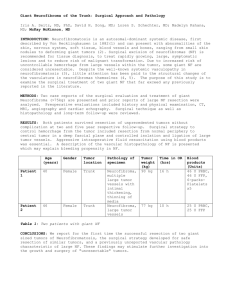
Title: Tie Up Technique for Hemorrhageless Resection of Diffuse Neurofibroma Authors: Sachio Kouraba, MD, Taisuke Sakamoto, MD, Cyu Kimura, MD, Akiteru Takeuchi, MD, Emi Funayama, MD, Yuhei Yamamoto, MD, Tomoko Yokoyama, MD, Tamotsu Kamishima, MD, Masanobu Kumakiri, MD Neurofibromatosis type 1 (NF1) is a common genetic disease that affected one in every 2500 to 3000 live birth. NF1 is of particular interest to the plastic surgeons, as it affects skin with various clinical manifestations. Diffuse neurofibroma, an uncommon but distinctive form, may produce gross disfigurement such as elephantiasis neurofibromatosis. Although the majority of patients require surgical procedure for cosmetic and functional reasons, the associated vascular malformations consist of excessive vascular fragility make most surgeons hesitant to address them. In fact, surgical resection of neurofibroma may cause life-threatening hemorrhage and require massive transfusion. To develop safe surgical procedure, we direct our attention to the pathological characteristics of diffuse neurofibroma. Clinicopathologically, the entire subcutis in diffuese neurofibroma between superficial fascia and dermis is thickened by firm, grayish tumor tissue. Despite its infiltrative growth, it does not destroy the deep strauctures such as muscle. This characteristics of diffuse neurofibroma means hand-grasped pendulous tumor may not contain any of non-affected functional structures. First, these features were confirmed radiologically in a NF1 patient with elephantiasis neurofibromatosis on the trunk. The patient, 28-year-old woman, has repeated history of massive hemorrhage in surgical resection of elephantiasis neurofibromatosis. She was admitted to hospital to treat spontaneous massive hematoma within tumor on the back. On the radiological examination of hematoma with computed tomography, elephantiasis neurofibromatosis lesion next to hematoma was grasped longitudinally with both hands by an inspector. The grasped massive tumor with hands forms narrow pedicle without muscle involvement. On the basis of these findings, we developed “tie up” technique for hemorrhageless resection of diffuse neurofibroma. The details are as follows: (1) grasp up tumor to be excised, (2) pierce through the base of grasped tumor with a needle and suture, (3) tie up the base of tumor tightly 2 - 3 cm in width and repeat it all over the tumor to be excised. After that, blood supply to tumor is perfectly cut off and tumor resection may be completed without bleeding. The wound is sutured tightly in subdermal layer and closed with skin suture without drainage. All of ligation sutures are removed after wound closure. Hemorrhage in sutured wound after ligation suture removal may well controled with simple bolus dressing. We performed this procedure for four times in 3 NF1 patients with a history of massive transfusion in resection of diffuse neurofibroma. Counts of blood loss in each operations were 50g, 15g, 412g and 18g. No transfusion was needed in all patients. Massive hemorrhage (412g) was experienced due to incomplete ligation of tumor.