Progressive Neuroscienc
advertisement

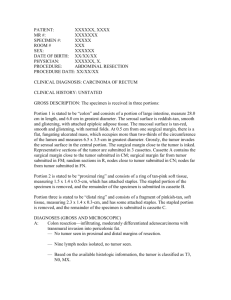
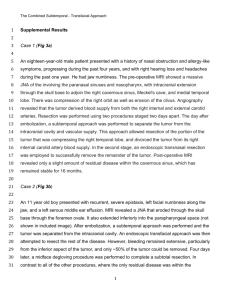
Case Report Resection of Lumbar Giant Cell Tumor By Benjamin R. Cohen, MD Neurosurgeon Winthrop-University Hospital fter failing all means of conservative treatment for back pain, a man in his 40s presented with intractable, worsening pain that traveled from his right hip and buttock down the posterolateral aspect of his right leg to the foot. The left lower and upper extremities were normal. A He complained of difficulty walking and episodes of right lower extremity paralysis, as well as being unable to function independently because of the pain and neurological problems. An MRI of the lumbar spine showed a lytic lesion consuming the body of L4 with extradural extension and compression of the thecal sac. The Giant cell tumors (GCT) of the spine are uncommon, accounting for approximately 2%-4% of bone neoplasms.1 While technically benign, these lesions can be aggressive, resulting from overproliferation of osteoclasts. With a high rate of recurrence,2 GCTs are typically seen in men and women between ages 20-45. Most patients present with debilitating back pain. However, the condition is usually diagnosed after development of a neurological deficit caused by the tumor’s compression of the spinal cord or nerve roots at the site of involvement. Given the complicated structure of the spine, diagnosis can be challenging, requiring the exclusion of degenerative disease, infections, muscular strains and neurologic impingements. In addition to pain, symptoms can range from slight weakness or an abnormal reflex to complete paraplegia, as well as bladder and bowel incontinence. MRI imaging studies are critical to pinpointing the tumor’s size, location, local extension and extent of neurological compression. For histological confirmation — and to exclude the leading differential diagnosis of aneurysmal bone cyst — a CTguided needle biopsy is necessary. While management of long bone GCTs usually involves curettage and filling the defect with bone cement,3 the treatment of choice for spinal GCTs is complex surgery, requiring careful preoperative planning and a multidisciplinary approach. The procedure — en bloc resection — offers the greatest chance for a cure.4 The role of adjuvant chemotherapy and/or radiation is controversial. Since tumors in this region frequently do not present until the mass has grown very large, surgery carries the potential for mechanical and neurological complications. Moreover, GCTs can be hypervascular, often mandating preoperative arterial embolization to reduce the potential for hemorrhaging during surgery. Ongoing multidisciplinary follow-up care — with routine X-rays and MRI studies — is crucial to monitoring for recurrence. remaining L4 vertebral body had deteriorated to nothing more than an “egg shell.” A needle biopsy confirmed that the lesion was a benign giant cell tumor (GCT) that needed to be excised in order to address the patient’s neurological deficits and spinal instability. Angiogram and Embolization Given the vascular nature of most GCTs, a preoperative angiogram was conducted, revealing a hypervascular mass at L4. Embolization was performed to reduce the tumor’s vascularity and the potential for extensive blood loss during surgery. Using the right transfemoral approach, a catheter was placed in the L4 lumbar artery, where a small amount of polyvinyl alcohol (PVA) glue was instilled to achieve devascularization of the tumor. Resection and Stabilization The surgery consisted of an intricate two-stage procedure conducted over two days. Stage one involved a complete posterior laminectomy from the bottom of L3 to the top of L5, with stabilization and fusion. The procedure resulted in the removal of a good portion of the L4 vertebral body, a wide surgical resection of the tumor and decompression of the nerves. Stage two, involved an anterior corpectomy at L4 for resection of the remaining tumor with reconstruction using an expandable cage. Near-complete resection of the tumor was completed. Since the lesion was contained in one area and near total resection was achieved, adjuvant therapy was not recommended. Two weeks postoperatively, the patient reported significant improvement of his symptoms, with the preoperative right lower extremity pain, weakness and dysfunction completely resolved. To help determine this patient’s future care and ensure timely treatment should the GCT recur, postoperative monitoring will involve regular examinations with interval X-rays, CT scans and MRI studies. For more information call the Institute for Neurosciences at 1-866NEURO-RX or visit www.winthrop.org. REFERENCES 1. Mendenhall WM, Zlotecki RA, Scarborough MT, et al. Giant cell tumor of bone. AJCOnc 2006; 29:96-99. 2. Abbas AK, Kumar V. Fausto N, et al. Robbins and Cotran Pathologic Basis of Disease, Professional Edition E-Book, W.B. Saunders Co. 2010 ISBN:1437721826. 3. Turcotte RE. Giant cell tumor of bone. OrthoClinNorthAm 2006;37:35-51. 4. Martin C, McCarthy EF. Giant cell tumor of the sacrum and spine:series of 23 cases and a review of the literature. IowaOrthoJ 2006;30:69-75.