recurrent jejunal gastrointestinal stromal tumour (gist)
advertisement
")
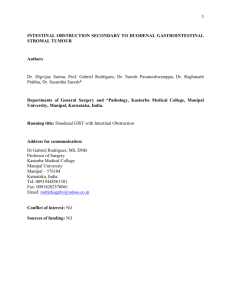
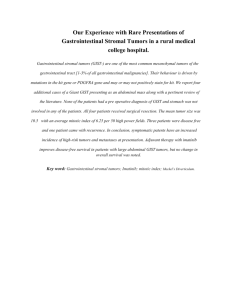
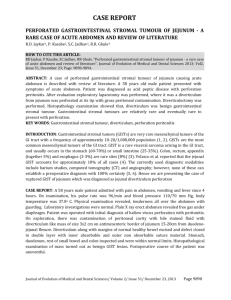
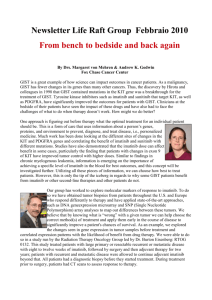
Recurrent Jejunal Gastrointestinal Stromal Tumour (GIST) – A Case Report and Literature Review. 1. Kabir Bolarinwa Badmos Histopathology unit, Laboratory department, Federal Medical Centre Gombe. Nigeria. 2. Laila Salah Seada Histopathology unit, Laboratory department, King Khalid Hospital, Hail. Saudi Arabia. 3. Sunday Kelvin Obianno Surgery department, Federal Medical Centre Gombe. Nigeria. Federal Medical Centre Gombe, Nigeria Correspondence to: Dr KB Badmos Histopathology unit, Laboratory Department, King Khalid Hospital, Hail, Saudi Arabia. (Formerly of Laboratory Department, Federal Medical Centre, Gombe, Nigeria) Telephone: +966 500 780 794 Fax no: +966 534 5959 E-mail: badmoskb@yahoo.com Source(s) of support: None Word counts: Abstract – 148 words Text – 998 words Number of figures - 4 Running title: Recurrent Jejunal Gastrointestinal Stromal Tumour Abstract: We present a 54 year old woman with recurrent jejunal GIST. Despite its complete excision at the first surgery, the huge size of the tumour (>10cm) conferred a great risk of recurrence and metastasis. Thus, tumour recurrence 5 years later necessitated a second surgical resection, immunohistochemistry confirmation of GIST and adjuvant imatinib mesylate (IM) treatment for a mandatory period of 1 year. The tumour was positive for c-KIT, negative for smooth muscle actin (SMA), desmin, CD 34 and S100 which confirmed GIST, thus qualified the patient for enrolment in the free imatinib mesylate (Gleevec) trial study in Nigeria. Although the patient was free of tumour recurrence at 18 months, the risk of recurrence/metastasis was very high due to the huge tumour size. The delay in immunohistochemistry diagnosis and commencement of Gleevec due to economic reasons highlight challenges in oncology management in a low resource economy such as Nigeria. Keywords: Jejunal GIST, Imatinib mesylate, Metastasis, Nigeria, Introduction: Gastrointestinal stromal tumour (GIST) is the commonest mesenchymal neoplasm of the gastrointestinal tract, driven by oncogenic activation of KIT or platelet derived growth factor receptor α (PDGFRA).1,2 Hitherto, most gastrointestinal mesenchymal neoplasms were thought to be smooth muscle derivatives and were thus classified, but identification of KIT a receptor tyrosine kinase protein in this tumour necessitated reclassification. GISTs are consequently thought to arise from interstitial cells of Cajal or their precursor spindle cells that are equally known to express KIT.2 GISTs occur mainly in adult population, about 60% of which are located in the stomach and very rarely in children (<1% of reported cases).3 Small intestinal GISTs are said to account for about 30% of all GISTs with specified location and jejunum is more frequently involved than the ileum.3,4 Small intestinal GISTs are more often malignant than gastric GISTs with 40-50% tumour related mortality. Mortality being higher in tumours >5cm or with mitotic rate >5 per 50HPFs.4 Small intestinal GISTs could either be spindle or epithelioid in appearance with the latter being strongly associated with malignancy.4 Virtually all small intestinal GISTs are KIT positive. Other markers of interest in GIST immunohistochemistry include PDGFRA, CD34, SMA, Desmin, S100, Ki67 and DOG 1 among others. The potential for recurrence and metastasis of this tumour several years after its removal makes it imperative for proper patients’ assessment and treatment plan. We present the case of a 54 year old woman with recurrent huge jejunal GIST, immunohistochemistry diagnosis and treatment challenges. Case report: A 54-year old woman presented first in 2004 with a week history of abdominal pains, vomiting and general body weakness to the surgical outpatient of Federal Medical Centre, Gombe. Important clinical finding was a huge abdominal mass that measured 18x16cm in dimension extending from the epigastrum to the lower abdomen. Abdominal ultrasound was suggestive of a retroperitoneal tumour probably a pancreatic pseudocyst. Exploratory laparotomy revealed a reniform mass attached to the jejunum, measured 20x15x10cm and was surgically removed with 5cm tumour free margins. Histopathological report of the specimen was suggestive of GIST and the patient was discharged a week after surgery to the outpatient clinic. She defaulted from the clinic only to present 5 years later (2009) with complaints and examination findings similar to the first presentation. Abdominal ultrasound (USS) reported a retroperitoneal mass measuring 20x16x10cm while the liver, pancreas, gallbladder and kidneys were normal. Exploratory laparotomy revealed a small intestinal mass that measured 25x20x10cm. Histopathological examination showed a 14cm long small intestinal segment to which is attached a huge mass (Figure 1) which weighed 2.6kg and measured 19x17x11cm. Microscopy revealed spindle shaped cells with elongated nuclei and fibrillary cytoplasm (Figure 2). Initial diagnosis suggested GIST, and patient was discharged to the outpatient clinic one week after surgery. Confirmatory immunohistochemistry (Figure 3 & 4) done 12 months later showed diffuse cytoplasmic KIT-positivity while CD 34 was negative. She was counselled for adjuvant treatment with Imatinib mesylate (IM) but yet to commence treatment 18 months post-surgery although she was free of tumour recurrence. Discussion: The annual incidence of GISTs from a population-based study conducted in western Sweden was found to be 14.5 cases per million.5 In the AFIP study of 906 stromal tumours involving jejunum or ileum, jejunal location tend to be commoner by a factor of 1.6:1. There is slight male predominance and the median age of 59 years was reported.4 Immunohistochemical KIT positivity is a defining feature of GISTs and virtually all small intestinal GISTs (>98%) are KIT positive.4 Tumour size is an important prognostic factor which independently could influence recurrence/metastasis.6 Based on a long-term follow-up studies on GISTs, 52% of patients with jejunal and ileal GISTs with tumour size >10cm and mitotic rate ≤5 per 50HPFs tend to have progressive disease during follow-up.4 The resected tumour in our patient was >10cm, which conferred a high risk of recurrence/metastasis on the patient. Histologically, small intestinal GISTs are mostly spindle cell tumours as observed in our case. The presence of epithelioid pattern seen in 5% of small intestinal GISTs is significantly linked to malignant transformation.4 Also the presence of extracellular collagen fibers referred to as skenoid fibers as seen in this case conferred a favourable prognostic feature and is commonly seen in non-malignant cases.7 Mitotic count is another important prognostic parameter, tumours with mitotic rate ≤5 per 50HPFs have comparatively better prognosis compared to those with mitotic rate >5 per 50HPFs when other factors are constant.3,6 The mitotic count in the case presented is low, ≤5 per 50HPFs, and this probably has a positive influence on the progression of the disease in this case. Immunohistochemical staining confirming GISTs is a prerequisite for diagnosis. The panel of stains commonly employed includes KIT, CD34, SMA, desmin, S100 and protein kinase C theta.8 Although KIT was positive in this case and it is a major defining feature for GIST, it is no longer considered an absolute requirement. CD34 which was negative in this case is reported to be positive in about 50% of small intestinal GISTs but it has little prognostic value. SMA is positive in about 35% of small intestinal GISTs and showed inverse pattern in frequency of expression as compared with CD34. Desmin and S100 are very rarely encountered in small intestinal GISTs. Protein kinase C theta is positive in a high percentage of GISTs but the staining pattern is less distinctive and weaker compared to KIT positivity.8 Targeted treatment with KIT and other receptor tyrosine kinase inhibitors such as IM in unresectable, recurrent and metastatic GISTs have considerably improved survival and disease free interval in large number of patients.9 In Nigeria, free Glivec (IM) trial study commenced in 2003 with a prerequisite immunohistochemical diagnosis before treatment.10 Conclusion: Tumour recurrence in this patient is strongly linked to the huge tumour size despite other favourable morphological parameters seen histologically. The prohibitive cost of immunohistochemistry (US160 dollar) in low resource economy such as Nigeria often results in treatment delay as demonstrated by this case even though IM is totally free. References: 1. Lasota J, Corless CL, Heinrich MC, Debiec-Rychter M, Sciot R, Wardelmann E, et al. Clinicopathologic profile of gastrointestinal stromal tumours (GISTs) with primary KIT exon 13 or exon 17 mutations: a multicenter study on 54 cases. Modern Pathology, 2008;21: 476-484. URL: http://www.nature.com/modpathol/journal. 2. Miettinen M, Lasota J. Gastrointestinal stromal tumours (GISTs):- Definition, occurrence, pathology, differential diagnosis and molecular genetic features. Pol J Pathol, 2003;54: 3-24. URL: http://www.ncbi.nlm.nih.gov/pubmed 3. Miettinen M, Lasota J. Gastrointestinal stromal tumours: Pathology and Prognosis at Different Sites. Semin Diagn Pathol, 2006;23: 70-83. URL: http://www.ncbi.nlm.nih.gov/pubmed 4. Miettinen M, Makhlouf H, Sobin LH, Lasota J. Gastrointestinal stromal tumours (GISTs) of the jejunum and ileum: a clinicopathologic, immunohistochemical and molecular genetic study of 906 cases prior to imatinib with long-term follow-up. Am J Surg Pathol, 2006;30: 477-489. URL: http://www.ncbi.nlm.nih.gov/pubmed 5. Nilsson B, Bumming P, Meis-Kindblom JM, Oden A, Dortok A, Gustavsson B, et al. Gastrointestinal stromal tumours: the incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era: a population-based study in western Sweden. Cancer, 2005;103: 821-829. URL: http://onlinelibrary.wiley.com 6. Koay MH, Goh YW, Iacopetta B, Grieu F, Segal A, Sterrett GF, et al. Gastrointestinal stromal tumours (GISTs): a clinicopathological and molecular study of 66 cases. Pathology, 2005;37: 22-31. URL: http://www.ncbi.nlm.nih.gov/pubmed 7. Min KW. Small intestinal stromal tumors with skeinoid fibers. Clinicopathological, immunohistochemical, and ultrastructural investigations. Am J Surg Pathol, 1992;16:145–155. URL: http://www.ncbi.nlm.nih.gov/pubmed 8. Motegi A, Sakurai S, Nakayama H, Sano T, Nakajima T. PKC theta, a novel immunohistochemical marker for gastrointestinal stromal tumours (GIST), especially useful for identifying KIT-negative tumours. Pathol Int, 2005;55: 106-112. URL: http://onlinelibrary.wiley.com 9. Deshaies I, Cherenfant J, Gusani NJ, Jiang Y, Harvey HA, Kimchi ET, et al. Gastrointestinal stromal tumour (GIST) recurrence following surgery: review of the clinical utility of imatinib treatment. Therapeutics and Clinical Risk Management, 2010;6: 453-458. URL: http://www.ncbi.nlm.nih.gov/pmc 10. Durosinmi MA, Ogbe PO, Salawu L, Oyekunle AA. Herpes zoster complicating imatinib mesylate for gastrointestinal stromal tumour. Singapore Med J, 2007;48: 1618. URL: http://www.sma.org.sg/smj Fig 1. Macroscopic appearance showing greyish-white tissue on cut section with pale yellowish areas. Fig 2. Microscopy showing spindle shaped cells with elongated nuclei, fibrillary cytoplasm and loose texture stroma with areas of abundant extracellular eosinophilic skenoid fibres. Haematoxylin & Eosin x 40 Fig 3. Immunohistochemistry showing diffuse cytoplasmic KIT-positivity. x400 Fig 4. Immunohistochemistry showing CD 34 negativity. x400