Grade
advertisement

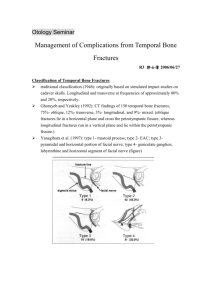
Otology Seminar Facial Nerve Paralysis Induced by Temporal Bone Fracture R3 黃俊棋 2005/09/07 Anatomy of facial nerve: Segment Cerebellopontine cistern IAC segment Labyrinthine segment Tympanic segment Mastoid segment Extratemporal segment Location Brain stem to IAC In IAC Fundus of IAC to geniculate ganglion facial hiatus to pyramidal eminence Pyramidal process to stylomastoid foramen Stylomastoid foramen to pes anserinus Length, mm 15-17 8-10 3-4 8-11 10-14 15-20 Grade system of facial plasy: The Detailed Evaluation of Facial Symmetry (DEFS): total paralysis more paralyzed more normal face at rest 0 6 14 wrinkling forehead 0 3 7 eye closure 0 9 21 Smiling 0 9 21 Whistling 0 3 7 Yanagihara facial nerve grading system: normal symmetry 20 10 30 30 10 House-Brackmann Classification of Facial Function: Grade I. Normal II. Mild dysfunction III. Moderate dysfunction IV. Moderately severe dysfunction V. Severe dysfunction VI. Total paralysis Characteristics Normal facial function in all areas Gross Slight weakness noticeable on close inspection May have slight synkinesis At rest, normal symmetry and tone Motion Forehead - Moderate-to-good function Eye - Complete closure with minimal effort Mouth - Slight asymmetry Gross Obvious but not disfiguring difference between the two sides Noticeable but not severe synkinesis, contracture, or hemifacial spasm At rest, normal symmetry and tone Motion Forehead - Slight-to-moderate movement Eye - Complete closure with effort Mouth - Slightly weak with maximum effort Gross Obvious weakness and/or disfiguring asymmetry At rest, normal symmetry and tone Motion Forehead - None Eye - Incomplete closure Mouth - Asymmetric with maximum effort Gross Only barely perceptible motion At rest, asymmetry Motion Forehead - None Eye - Incomplete closure Mouth - Slight movement No movement Type of temporal bone fracture: Traditional classification: Longitudinal Fracture 70 - 80 %; 10 - 25 % facial palsy; perigeniculate region; compression and ischemia; delay type Transverse fracture: 10-30 %, 30 - 50 % facial palsy, geniculate ganglion and proximal tympanic segment (small size and lack of fibrous supporting tissue); avulsion or severed by bony fragments; immediate type Mixed fracture: 0-20 % Otic capsule sparing vs. otic capsule violating fracture Otic capsule violating fracture: 2.5 - 5.6%, 2 times to develop facial paralysis Yanagihara’s classification: Classifications of Nerve Injuries: Pathology Conduction block, damming of axoplasm Transection of the axon with intact endoneurium Transection of nerve fiber (axon and endoneurium) inside intact perineurium Above plus disruption of perineurium (epineurium remains intact) complete transection of a nerve Sunderland First degree Second degree Third degree Seddon Neurapraxia Axonotmesis Neurotmesis Fourth degree Neurotmesis Fifth degree Neurotmesis usually mixed type; degree II to V will cause wallerian degeneration with degeneration and break up of axoplasma and myelin sheaths and cleared away by macrophage 72 hours later Diagnosis: Electrical testing: distinguish degree I from II - V lesions but cannot distinguish II from V rapid wallerian degeneration → neurotmesis; slowly → axonotmesis 100% wallerian degeneration occurs over 3 to 5 days as the distal axon slowly degenerates Nerve excitability test (NET): electrode on the skin over the stylomastoid foramen difference > 3.5 mA → progressive degeneration useful only during the first 2 to 3 weeks of complete paralysis Maximum stimulation test (MST): maximal or supramaximal stimuli; but painful Electroneurography (ENOG) or Evoked electromyography (EEMG): transcutaneous bipolar electrode at the stylomastoid foramenwith maximal or supramaximal stimulation and recorded by electrode in the nasolabial groove average difference: 3%; test-retest errors: 20%; > 30% → meaningful degeneration > 90% within 6 days or > 95% within 14 days → poor Electromyography (EMG): Needle electrode into the orbicularis oculi and orbicularis oris muscles Voluntarily active facial motor units → good spontaneous recovery polyphasic reinnervation potentials in 4 to 6 weeks → good recovery fibrillation potentials 10 to 14 days later → degenerating motor units Schirmer test HRCT Clinical presentation: Immediate onset with degeneration: avulsion or severed by bony fragments Immediate onset without degeneration: compression and ischemia Delayed onset with degeneration: compression and ischemia delayed diagnosis of infection Delayed onset without degeneration: compression and ischemia Management: Steroid Surgical exploration Indication of surgical exploration: Immediate, complete facial palsy, degeneration > 90%, without voluntary motor unit, HRCT showed fracture line; others are controversial Fisch: ENoG showed degeneration > 90 % within 6 days of onset of facial palsy 90-98 % complete spontaneous recovery in delayed onset cases Time to exploration: McCabe: 72 hours; if impossible, 21th day (nerve cell body is maximally capable of pushing axoplasmic filaments across the neuronal gap) Fisch: 3 weeks later to allow resolution of edema and hematoma Chang and Cass: beneficial within 14 days Poor return of function 6-18 months later → late exploration and grafting Quaranta: 77.7 % good recovery with surgical exploration 2-3 months later Ulug: 81 % good recovery with surgical exploration 3 months later References: Ulug T, Arif Ulubil S. Management of facial paralysis in temporal bone fractures: a prospective study analyzing 11 operated fractures. Am J Otolaryngol. 2005 Jul-Aug;26(4):230-8. Ulug T, Ulubil SA. Bilateral traumatic facial paralysis associated with unilateral abducens palsy: a case report. J Laryngol Otol. 2005 Feb;119(2):144-7. Li J, Goldberg G, Munin MC, Wagner A, Zafonte R. Post-traumatic bilateral facial palsy: a case report and literature review. Brain Inj. 2004 Mar;18(3):315-20. Review. Darrouzet V, Duclos JY, Liguoro D, Truilhe Y, De Bonfils C, Bebear JP. Management of facial paralysis resulting from temporal bone fractures: Our experience in 115 cases. Otolaryngol Head Neck Surg. 2001 Jul;125(1):77-84. Quaranta A, Campobasso G, Piazza F, Quaranta N, Salonna I. Facial nerve paralysis in temporal bone fractures: outcomes after late decompression surgery. Acta Otolaryngol. 2001 Jul;121(5):652-5. Dahiya R, Keller JD, Litofsky NS, Bankey PE, Bonassar LJ, Megerian CA. Temporal bone fractures: otic capsule sparing versus otic capsule violating clinical and radiographic considerations. J Trauma. 1999 Dec;47(6):1079-83. Yanagihara N, Murakami S, Nishihara S. Temporal bone fractures inducing facial nerve paralysis: a new classification and its clinical significance. Ear Nose Throat J. 1997 Feb;76(2):79-80, 83-6. Review. Brodie HA, Thompson TC. Management of complications from 820 temporal bone fractures. Am J Otol. 1997 Mar;18(2):188-97. Review. Coker NJ. Management of traumatic injuries to the facial nerve. Otolaryngol Clin North Am. 1991 Feb;24(1):215-27. Review. Cannon CR, Jahrsdoerfer RA. Temporal bone fractures. Review of 90 cases. Arch Otolaryngol. 1983 May;109(5):285-8. Harker LA, McCabe BF. Temporal bone fractures and facial nerve injury. Otolaryngol Clin North Am. 1974 Jun;7(2):425-31. Review.