somatosensory pathways
advertisement

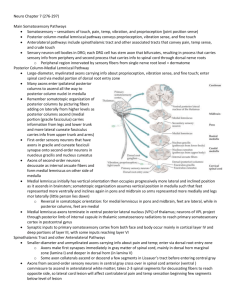
Somatosensory Pathways 1 SOMATOSENSORY PATHWAYS MAIN SOMATOSENSORY PATHWAYS Summarized by Laurie Ryan (minor additions by Kira Armstrong 9/02, shortened by Dean Beebe 11/04) Basic Facts: 1. Somatosensory: bodily sensations of touch, pain, temperature, vibration, and proprioception (limb or joint position sense) 2. Two main pathways: See Table 7.1, Figure 7.1, 7.2 a. Posterior column – medial lemniscal pathway: conveys proprioception, vibration, fine/discriminative touch b. Anterolateral pathways: include spinothalamic tract and other associated tracts that convey pain, temperature, crude touch 3. Some aspects of touch carried by both pathways; not eliminated in isolated lesions to either pathway 4. Four types of sensory neuron fibers have specialized peripheral receptors that subserve different sensory modalities, classified by axon diameter (see Table 7.2) 5. Dorsal root ganglion: neuron cell bodies; bifurcated stem axon – one conveys sensory info from periphery, other carries info into spinal cord through dorsal nerve roots 6. Dermatone: peripheral region innervated by sensory fibers from a single nerve root level; dermatomes for different spinal levels form a map over the surface of the body (see Figure 8.4) See Figure 7.1, 7.4 Posterior column – medial lemniscal pathway: ML Pathway decussate in medulla thalamus posterior limb of internal capsule primary somatasensory cortex 1. Large diameter myelinated axons carry proprioception, vibration, fine/discriminative touch; enter spinal cord via medial portion dorsal root entry zone 2. Many of the axons enter the ipsilateral posterior columns to ascend all the way to the posterior column nuclei in the medulla 3. In addition, some axon collaterals enter the cord central gray matter to synapse onto interneurons and motor neurons 4. Somatotopic organization: See Figure 7.3, add on laterally as it ascends; gracile fasciculus: medial, info from legs/lower trunk; cuneate fasciculus: lateral, info from upper trunk above to about T6 and arms/neck; first order sensory neurons that have axons in these synapse onto second-order neurons in nucleus gracile and nucleus cuneatus 5. Axons of the second-order neurons decussate as internal arcuate fibers and then form medial lemniscus on the other side of the medulla 6. Medial lemniscus axons terminate in the ventral posterior lateral nucleus (VPL) of the thalamus 7. Neurons of the VPL project through the posterior limb of the internal capsule in the thalamic somatosensory radiations to reach the primary somatosensory cortex 8. Touch for the face conveyed via analogous path – trigeminal lemniscus (see ch. 12) Spinothalamic tract and other anterolateral pathways: 1.small diameter unmyelinated axons carrying pain, temperature info also enter cord via dorsal root entry zone but make first synapse immediately in cord gray matter mainly in dorsal horn marginal zone (lamina I) and deeper in dorsal horn (lamina V) THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes. Somatosensory Pathways 2 2. Some axon collaterals ascend/descend a few segments in Lissauer’s tract before entering central gray 3. Second-order central gray sensory neurons cross over in spinal cord anterior (ventral) commissure to ascend anterolateral white matter 4. Takes 2-3 spinal segments for decussating fibers to reach opposite side – lateral cord lesions affect contralateral pain/temp a few segments below 5. Somatotopic organization: feet most laterally represented 6. Thalamus next major relay which projects via thalamic somatosensory radiations to primary somatosensory cortex 7. Pain/temp for face carried by analogous path – trigeminothalamic tract (see ch. 12) 8. Some crude touch also when posterior columns damaged 9.consists of 3 tracts: spinothalamic, spinoreticular, spinomesencephalic Spinothalamic: discriminative pain/touch, e.g., location/intensity; main relay ventral posterior lateral nucleus (VPL); projections to other thalamic nuclei – intralaminar and medial nuclei such as mediodorsal; lamina I & V Spinoreticular: emotional and arousal aspects of pain; terminates medullary-pontine reticular formation which projects to intralaminar thalamic nuclei (centromedian) – project diffusely to entire cortex and thought to be involved in behavioral arousal; lamina 6 - 8 Spinomesencephalic: pain modulation; projects to midbrain periaqueductal gray matter and superior colliculi; lamina I & V SOMATOSENSORY CORTEX See Figure 7.1, 7.2, 6.1 Primary somatosensory cortex: 1.postcentral gyrus; areas 3, 1, and 2 2.thalamaic VPL and VPM nuclei convey somatosensory info to the cortex 3. Somatotopic organization: face most laterally and leg, most medially 4. Conveys info to secondary somatosensory association cortex in the parietal operculum (superior margin of Sylvian fissure); somatotopic organization 5. Further processing occurs in association cortex of posterior parietal lobule including areas 5and 7 6. Extensive connections with motor cortex 7. Lesions produce cortical sensory loss (see KCC 7.3) THE THALAMUS See Table 7.3, Figure 7.6 Basic Facts: 1. “Inner chamber/bedroom” in Greek 2. Important processing station; nearly all pathways that project to cortex do so via relays in the thalamus- major sensory relay station 3. Nuclei receive dense reciprocal feedback connections from cortical areas. In fact, cortical thalamic projections outnumber thalamocortical projections 4. See ch. 14-17 5. Divided into: medial, lateral, and anterior nuclear groups by internal medullary lamina (yshaped, white matter) – it’s nuclei called intralaminar; midline thalamic nuclei (thin, adjacent 3rd ventricle); thalamic reticular nucleus (lateral aspect) THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes. Somatosensory Pathways 3 6. 3 main categories of nuclei: relay, intralaminar, and reticular See Figure 7.7, 7.8 Relay Nuclei: 1. Makes up most of thalamus 2. Lateral: all sensory but olfaction have specific relays; VPL, VPM; lateral geniculate nucleus (LGN) – visual (ch. 11); medial geniculate nucleus (MGN) – auditory (ch. 12); ventral lateral nucleus (VL) – cerebellum/basal ganglia motor 3. Anterior: limbic pathways (ch. 18) 4. Nonspecific nuclei: widespread projections; e.g., pulvinar: posterior, large, pillow-shaped, behavioral orientation; mediodorsal nucleus (MD): major relay to frontal association, cognitive functions Intralaminar Nuclei: 1. Within internal medullary lamina 2. Input from numerous pathways, reciprocal cortical connections; sometimes classified with other “nonspecific” relay nuclei 3. 2 functional regions: caudal intralaminar nuclei – include centromedian nucleus, and mainly basal ganglia (ch. 16); rostral intralaminar nuclei – basal ganglia and inputs from ascending reticular activating system (ARAS) to cortex, maintaining alert/conscious state (ch. 14) Reticular Nucleus: 1. Lateral; only nucleus that does not project to cortex 2. Regulates thalamic activity 3. Receives input from other thalamic nuclei and cortex and then projects back to thalamus 4. Almost pure population of inhibitory GABAergic neurons 5. Other inputs from brainstem reticular activating system and basal forebrain may modulate alertness/attention (ch. 14, 19) KEY CLINICAL CONCEPTS Paresthesias: 1. Abnormal positive sensory phenomena 2. Character and location can have localizing value; e.g., posterior column lesions (medial lemniscal pathways) = tingling, numbness, tight bandlike feeling around trunk/limbs (See 7.1, page 276) 3. Dejerine-Roussy syndrome: parietal/primary sensory cortex lesions; severe contralateral pain 4. Lhermitte’s sign: cervical lesions; electricity-like feeling running down back to extremities with neck flexion 5. Radicular pain: nerve root lesions; radiates down limb in dermatomal distribution; numbness/tingling; provoked by movements stretching nerve root 6. Peripheral nerve lesions can cause – are of nerve distribution (See KCC 8.3) 7. Other terms: dysesthesia (unpleasant); hyperpathia/allodynia (painful) Summary of Types of parathesias depending upon location 1. Lesions of anterolateral pathways – sharp, burning or searing pain 2. Lesions of parietal lobe or primary sensory cortex – numb or tingling, but pain can also be present 3. Thalamus – severe contralateral pain dejerine-roussy syndrome THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes. Somatosensory Pathways 4 Spinal cord lesions: See Table 7.4 1.major disability; involve motor, sensory, autonomic paths 2. Signs/sx’s obvious when sensory level and motor dysfunction correspond to level of lesions (See KCC 7.4) 3. Reflex abnormalities: e.g., abnormal sphincter help confirm diagnosis 4. In subtle cases, minor sensory/motor changes, back/neck pain, or fever may be only clues 5. In acute severe lesions, often initial phase of spinal shock: flaccid paralysis below lesions, loss of tendon reflexes, decreased sympathetic outflow – decreased blood pressure, absent sphincter reflexes, and tone 6. Myelitis: infectious or inflammatory (See KCC 5.9, 6.6) Sensory loss: patterns and localization (See pages 278-285): 1. Primary somatosensory cortex: contralateral; discriminative touch/joint position most severely affected but all modalities may be involved; all primary senses can be relatively spared but cortical sensory loss (extinction, or decreased stereognosis, and graphesthesia, ch. 3) present (See KCC 19.6) 2. VPL/VPM/thalamic somatosensory radiations: contralateral; may be more noticeable in face/hand/foot than trunk/proximal extremities; sometimes with no motor deficit 3. Lateral pons or lateral medulla: contralateral pain/temp loss for body but ipsilateral for face (See KCC14.3) 4. Medial Medulla: contralateral vibration/joint position loss (ch. 14) 5. Spinal cord: See KCC 7. 6. Nerve roots or peripheral nerves: distal symmetrical polyneuropathies cause bilateral sensory loss in a “glove and stocking” distribution in all modalities; specific lesions cause sensory loss in specific territories (See KCC 8.3, 9.1) Spinal cord syndromes: See pages 280-283, Figure 7.10 1. Transverse cord lesion: all sensory/motor paths partially/completely interrupted; often a sensory level corresponding to lesion level; common causes – trauma, tumor, MS 2. Hemicord Lesions: Brown-Sequard syndrome: See page 280; lesions lateral corticospinal = ipsilateral upper motor neuron weakness; posterior columns = ipsilateral loss vibration/joint position sense; anterolateral = contralateral loss pain/temp Common causes – MS, tumors, penetrating injuries 3. Central cord syndrome: small lesions in spinothalamic fibers cause bilateral regions of suspended sensory loss to pain/temp; cervical lesions cause classic cape distribution; sacral sparing (loss below lesions except in this region) 4. Posterior cord syndrome: posterior column lesions cause loss of vibration and position sense below lesion level 5. Anterior cord syndrome: loss of pain/temp below lesion level; anterior horn lesions = lower motor neuron weakness at lesion level THE FINE PRINT: Caveat emptor! These study materials have helped many people who have successfully completed the ABCN board certification process, but there is no guarantee that they will work for you. The notes’ authors, web site host, and everyone else involved in the creation and distribution of these study notes make no promises as to the complete accuracy of the material, and invite you to suggest changes.