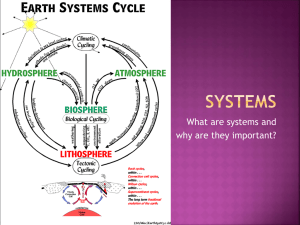
blepharoplasty
advertisement

Lip Teh December 2005 Blepharoplasty History >2000 years ago: Susruta eyelid surgery 1000s: Avicenna first recorded skin only blepharoplasty 1600s: Pare described the functional correction of excess eyelid skin Sichel 1844: first accurate description of the herniated orbital fat Fuchs 1899: first to recognize the cosmetic value and coined the term blepharochalasis Miller 1907: first cosmetic surgery text Bourguet 1929: described the transconjuctival approach and fat compartments Castanares 1951: detailed description of the fat compartments Furnas 1970s: described removal of redundant orbicularis Tenzel 1976: recognized extropion being due to lower eyelid laxity Putterman1982: first text book dedicated to cosmetic oculoplastic surgery Bosniak 1985: described the use of diathermy to sculpt the fat Putterman 1990: described laser techniques Indications Blepharochalasis o Rare bilateral disease o Usually young women, usually upper lids o Thin, atrophic, wrinkled skin in excess o Protruding fat due to weakened septum o due to recurrent episodes of angioneurotic oedema (IgE mediated) o difficult to treat as likely to recur Dermatochalasis o Common bilateral disease o Male=female, middle-elderly o Horizontal redundancy of skin with herniation of fat o Supratarsal fold complex degenerates with age, and migrates superiorly ptosis Facial palsy o brow ptosis, lower eyelid retraction with horizontal eyelid laxity, lagophthalmos o prominent palpebral-malar and nasojugal sulci with hollowing of the infraorbital region o reduced nasolabial fold Hazards Ptotic brow o If compensated, then brow ptosis won’t be noticed until after blepharoplasty Graves disease o Proptosis o Lid retraction o Lid lag – inability of the upper eyelids to relax adequately to cover the corneas on down gaze Dry eyes – Schirmers test not reliable 1. relative or real proptosis 2. exophthalmos 3. hypotonia of the lower eyelids 4. maxillary hypoplasia 5. inferior scleral show Weak or absent Bell’s phenomenon Absent corneal reflex Lip Teh December 2005 Lagopthalmos Ptosis Lack of lower eyelid support o Negative vector o Scleral show o Ectropion Bleeding tendencies Considerations Incision and approach Skin excision Muscle excision Fat excision or repositioning Supratarsal fold Canthal support and/or repositioning Upper Blepharoplasty x=12mm Skin Excision o need for precise planning of the caudal aspect of the incision - at crease in younger patients, 1mm caudal with older o superior margin marked with pinch technique or leave 12mm skin from fold to brow. o incisions have been made with scalpel, fine-tip diathermy, CO2 laser, scissors o should have 2-3mm lagopthalmos at the end Orbicularis Excision o non essential step o may allow definition of fold o 5-8mm strip above supratarsal fold(Baker), 2-3mm less than skin resection(Tebbetts) or 2-3mm maximum (Flowers) Postseptal fat excision o beware infratrochlear nerve and terminal branch Ophthalmic artery with medial fat pad excision o beware injury to extraocular nerves o hemostasis essential o overresection will lead to hollowed out look Lacrimal gland repositioning (Dacryopexy) Lip Teh December 2005 o partial excision is not recommended due to risk of dry eyes Supratarsal fold fixation o aim is to excise less skin, recreate a more youthful upper lid, and achieve longer lasting results o methods: 1. percutaneous 2. suture anchor (eyelid invagination – Flowers) Transect pretarsal extension of aponeurosis Sutures secure to cephalad edge of tarsus, pretarsal skin flap dermis and aponeurosis. Suturing to tarsus avoids eye lash eversion. Percutaneous fixation Post Operative: Cold compress Document vision prior to discharge Eye drops during day, ointment at night – 2 weeks (until lagopthalmos resolves) Sleep head up Ancillary procedures: o Brow correction – browpexy o Resection of procerus, corrugator o Ptosis correction o Canthopexy o Excision of ROOF fat pad o Ostectomy for prominent supraorbital rims especially out laterally Male blepharoplasty Often associated with brow ptosis Lip Teh December 2005 Most men don’t want to have ptotic brow address – bleph needs to be conservative and patient advised accordingly Asian blepharoplasty Asian upper eyelid is characterized by a. absent palpebral crease b. a medial epicanthal fold hooding the caruncle c. upward tilt of the lateral canthus d. a narrow palpebral aperture. 50% of Asian patients possess an upper eyelid with a low but defined upper eyelid crease, while the other 50% show little or no sign of crease formation. Causes: o Lower insertion point of the levator aponeurosis expansion into the dermis o An alternative theory states that the fold corresponds to the level of the septoaponeurotic sling. Lower height of the sling in Asians allows the prelevator fat to sit lower in the eyelid, leading to a puffy eyelid and a lower fold. Lip Teh December 2005 Procedures 1) Classical (Sayoc 1953) preferred for patients with thicker skin, thick pretarsal orbicularis muscle, or excess skin or for those for want permanence a. supratarsal incision b. excision of a 2-mm strip of orbicularis muscle over the entire length of the eyelid c. removal of excessive prelevator fat d. anchoring the lower muscle/skin flap to the insertion of the levator aponeurosis at the upper tarsal edge to construct the absent fibrous attachment 2) Percutaneous techniques preferable for patients with eyelids so thin that they fold spontaneously on an intermittent basis. Epicanthal folds Causes: Down syndrome Turner syndrome Phenylketonuria (PKU) Williams syndrome Noonan syndrome Rubinstein-Taybi syndrome Blepharophimosis syndrome Management Does not need to be modified in most cases and probably should not be unless it constitutes a severe deformity. Lip Teh December 2005 Epicanthoplasty If doing bleph at the same time, perform epicanthoplasty first because this alters the medial anatomy of the skin. 1) spilt V-W technique (Flowers) Total height of a V-W plasty is approximately 5 X 5 mm, with each arm of the V and W being approximately 2 mm 2) Z plasty (Fuente del Campo) 3) Dancing man (Mustarde) Lip Teh December 2005 Lower Blepharoplasty Approaches Skin only flap o best for patients with normal muscle tone but excess skin and severe wrinkling o Subciliary incision—skin only raised to infraorbital margin o Triangular skin excision more laterally — measure degree of skin excision with mouth open o high risk of lid retraction Skin Muscle Flap (McIndoe-Beare technique) o those with a balanced excess in skin and muscle. Less effective with marked skin redundancy o Better vascular supply—dissection in avascular plane under muscle. Results in less postoperative ecchymosis, subcutaneous scarring, and irregularity of the skin surface. o Corrects sagging from either muscle or skin cause o Preserve preseptal orbicularis to prevent ectropion o Risk – possible denervation of orbicularis causing lower lid malposition/ectropion 1. Recent studies (PRS Aug 2005) suggest that any denervation is temporary and clinically insignificant. o Technique: 1. Eyeshield 2. subciliary incision, stopping short of punctum 3. thru orbicularis leaving pretarsal orbicularis attached to tarsus. 4. Dissect submuscular plane, preserving orbital septum until infraorbital rim 5. Incise thru septum and excise medial, central, lateral fat pads as necessary 6. Excise skin and muscle (around 2mm so muscle doesn’t overlap pretarsal area) 7. hemostasis Separate skin/muscle flap o Advantages: 1. leaves the orbicularis-tarsus relationship intact 2. pretarsal orbicularis remains innervated. 3. Skin and muscle can be removed independently. Transconjunctical o Best used where herniated fat is the main problem o Benefits 1. avoids lower lid retraction 2. Retains natural appearance of palpebral fissure 3. Addresses bulging fat directly Lip Teh December 2005 o o o o o 4. Permits skin excision if required Disadvantage 1. limited exposure 2. inadequate fat removal, particularly from the lateral compartment 3. Difficult if requiring resection for hypertrophied orbicularis 4. extraocular muscle injury Relatively contraindicated in patient with tight lower eyelid due to poor exposure Preseptal or retroseptal approach. Retroseptal leaves septum intact which may lead to less ectropion. If has fine wrinkles – safely combine with laser or chemical peel resurfacing If has excess skin – skin only subciliary excision or pinch technique. Ancillary procedures Fine wrinkles o skin care programs, chemical peel, and laser resurfacing (CO2 erbium:yttrium) o laser resurfacing will result in 4-6mm of shortening so when combined with bleph, take less skin. Animated wrinkles o Overactive orbicularis – crows feet o Botox - to reduce the risk of temporary paralytic ectropion, conservative graded dosing is used in the lower orbicularis (5 units) Excess orbicularis o Leave pretarsal orbicularis intact o Some split the muscle vertically at lateral canthus to treat crows feet Orbicularis muscle suspension o May aid in correcting muscle hypertrophy, hypotonia/laxity, festoons and crows feet. Also believed to reduce risk of lid malposition (ie scleral show and rounding of eyelid) o Lateral part suspended to orbital rim periosteum or temporal fascia Excessive swelling - Radiofrequency eyelid sponge thermoplasty o Utilizes an insulated tungsten needle placed transcutaneously into the fluid sponge in the lower eyelid or cheek o The radiofrequency energy is applied in closed fashion to desiccate and scar the fluid sponge Orbital septum o Castañares and Beare concluded that it was not necessary to suture-reconstruct the septum during blepharoplasty to prevent subsequent reherniation of fat. o Despite this others routinely suture either septum or calsulopalpebral fascia to periosteum Deep nasojugal/malar grooves o Fat injection or fat grafting o Fat repositioning technique (Hamra) Malar descent o Midface lift Narrow palpebral angle o By elevating the malar fat pad and interrupting the arcus marginalis, the palpebral angle is narrowed and creates a more youthful appearance. Negative vector o At risk of clotheslining after horizontal tightening of the lateral canthus if proptosis >19mm on Hertel exopthalmometer - downward sliding of the lid and increasing lower lid retraction (McCord PRS 1998) o Treat with superior placement of the canthoplasty suture Enopthalmos o tendency of the lid to separate from the globe surface with tightening o canthoplasty fixation must be placed more deeply inside the lateral orbital rim to Lip Teh December 2005 avoid separation Lower lid laxity The most common complication of lower eyelid blepharoplasty is distortion of the lid, either overresection or unrecognised preoperative lower lid laxity causes of lower eyelid retraction after blepharoplasty: related to surgery a. inadequate skin (anterior lamellar insufficiency) – over resection b. middle lamellar inflammation and subsequent scarring between the orbital septum and capsulopalpebral fascia. i. Hematoma is the most common cause of ectropion ii. Fat pad manipulation or resection causes inflammation that can act as a scaffold for fibrosis between the overlying orbital septum and capsulopalpebral fascia, related to aging (need to be determined preop) c. lateral canthal tendon laxity or disinsertion – most common cause d. midfacial descent. Treatment 1. temporary external support of the lid margin 2. wedge resection to shorten the lid (Kuhnt -Szymanowski procedure) i. involves removal of a portion of the midtarsal plate ii. does not correct the lax lateral canthal tendon iii. violates commissure 3. suspension or tightening of the lower lid using skin or muscle components to create a suspensory sling 4. lateral tarsal strip - tarsal suspension to the periosteum or soft tissue of the lateral orbital rim i. addresses lateral canthal tendon laxity directly 5. lateral canthoplasty - Lateral retinacular suspension canthoplasty(Jelks) a double-armed suture is used to hitch the lateral canthal tendon to the periosteum of the upper lateral orbital rim. Hamra’s trancanthal canthopexy is a variation of this. Lip Teh December 2005 Complications 1. Blindness o Incidence 0.04% , 1 in 2500 (75 reported cases) o rapid onset of pain and proptosis, usually accompanied by eyelid ecchymosis o Cause Intraorbital hemorrhage (proptosis, dilated pupil) Ischemic optic neuropathy from fat retraction (tearing vessels) Vascular spasm from adrenaline Glabellar fat infections (fat embolism) Direct injury to globe o Management Remove all dressings and sutures immediately Opthamology consult Surgical emergency – 90 mins before permanent impairment Reduce intraocular pressure o 20% Mannitol 1–2 mg/Kg body weight (the first 12.5 g over a 3-minute period and the remainder over a 30-minute period) o Dexamethasone o Acetazolamide 500mg IV o 95% O2/5% CO2 mixture o Orbital bone decompression o Anterior chamber paracentesis Surgical decompression – release arcus marginalis and lateral canthus Bone decompression as last resort (lateral orbitotomy) Lip Teh December 2005 2. Hematoma o Retrobulbar - Most commonly from fat pad vessels o Superficial hematomas most commnly come from orbicularis and do not threaten vision o When small, they can usually be allowed to resolve spontaneously. If larger, they can be evacuated after liquefaction occurs 7 to 10 days later 3. Corneal injury o Prevention is the key. Consider use of corneal shields Lip Teh December 2005 4. Dry eyes o Select out patients at risk of this o Worsened by lagopthalmos 5. Diplopia o Temporary diplopia has been attributed to wound reaction, edema, and hematoma. o Permanent strabismus results from structural damage to the extraocular muscles or nerves o Most commonly injured are inferior oblique and superior oblique but also inferior rectus – may need to treat with strabismus surgery 6. Enopthalmos o Rare, although it could occur from very excessive removal of fat. o Relative enophthalmos more common: fat removal makes orbital rims more prominent. 7. Ptosis o most frequent cause is the failure to recognize the condition preoperatively o may also occur with direct injury to the aponeurosis during blepharoplasty. o Any injury that is recognized intraoperatively or immediately postoperatively should be repaired immediately 8. Lagopthalmos o well tolerated by patients who have normal tear production, and resolves with conservative treatment such as lubrication, massage, lid taping, and patching o Persistent lagophthalmos may be secondary to excessive skin resection or incorporation of the orbital septum in the incisional scar. o Treatment = recreating the defect and applying a full-thickness skin graft. 9. Lower lid malposition o Ranges from scleral show(15%), rounding of margin to ectropion(1%) o Causes: a. Excess skin, fat, muscle removal b. Scar contracture c. Denervation of orbicularis oculi (controversial) Deep lateral dissection d. Lid oedema e. Adhesions of orbital septum f. Hematoma g. Predisposing factors (Poor patient selection) a. Lax lid margin b. Proptosis/negative vector c. Ipsilateral high myopia o Management a. Most settle – due to oedema a. Eyelid massage (10x for 10mins for 10days) b. Eyedrops c. Taping d. Frost suture b. Subacute a. Scar-in-formation – consider steroid injection behind the scar, not intralesional b. Temporary tarsorrhaphy c. Release sutures and allow to heal secondarily c. Established (>6 months) a. Wedge tarsectomy (posterior lamella) b. tarsal strip lateral canthoplasty c. Skin graft if cicatritional 10. Overresection/Underresection 11. Asymmetry Lip Teh December 2005 12. Epiphora o Due to chemosis and oedema of lids with associated distortion of the lacrimal system. o Temporary paresis of orbicularis can aggravate epiphora. o Treatment is usually conservative and the patient reassured. o Rarely, it persists beyond a few days. If so, the inferior canaliculus can be probed and irrigated. 13. Chemosis o o o o 14. Scars o Vicious cyclical complication Swelling of conjuctiva = separation of lower lid from sclera = exposure of conjuctiva Cause o Blockade of eyelid lymphatics o Allergy to medications Management o Stop medications o Patching o topical and/or systemic steroids o decongestant eye drops o Temporary tarsorrhaphy as last resort Usually heals well