David Jablons - Wedge Resection
advertisement

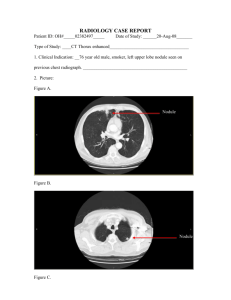
PREOPERATIVE DIAGNOSIS: metastasis. Left lower lobe nodule, rule out thyroid cancer POSTOPERATIVE DIAGNOSIS: metastasis. Left lower lobe nodule, consistent with thyroid OPERATION: 1. Flexible bronchoscopy. 2. Left video-assisted thoracoscopy. 3. Left mini thoracotomy. 4. Wedge resection of left lower lobe nodule. ANESTHESIA: Single- and double-lumen general endotracheal. CLINICAL INDICATIONS: This patient is a reasonably healthy 69-year-old woman with a history of thyroid cancer who was noted to have an isolated 8-mm to 1-cm nodule in the posterior basilar segment of the left lower lobe, amenable to resection. She has no other distant disease. She is taken to surgery today for definitive resection. FINDINGS: 1. On bronchoscopy, there was a normal tracheobronchial anatomy and no endobronchial lesions seen. 2. On thoracotomy she had a subtle 8-mm to 1-cm nodule in the posterior basilar segment of the left lower lobe, amenable to wedge resection but requiring a small minithoracotomy of several centimeters for exposure and safe resection. DESCRIPTION OF OPERATION: The patient was brought to the operating room and placed in supine position. After achievement of successful single-lumen general endotracheal anesthesia, bilateral venous compression stocking boots were placed, as were a Foley catheter and a radial arterial line. A flexible bronchoscope was introduced through the single-lumen endotracheal tube. The trachea and carina were inspected. The carina was in the midline and sharp. The right tracheobronchial tree down to the subsegmental level was grossly normal. No obvious endobronchial lesions were seen. A minimal amount of mucopurulent secretion was lavaged and suctioned clear. On the left side as well, no obvious endobronchial lesions were seen. All secretions were lavaged and suctioned clear. The bronchoscope was pulled back and removed. The patient tolerated this well, with oxygen saturations remaining greater than 98% throughout the procedure. Due to the difficult airway an endobronchial blocker was placed into the left mainstem, verified in correct position fiberoptically and taped in place. The patient was rotated leftside-up and prepped and draped in the usual sterile fashion for a thoracoscopy. A single Thoracoport incision was fashioned at the seventh or eighth interspace and carried down under direct vision. The chest was entered. There was reasonably good lung collapse. A small access port was placed posteriorly over approximately the eighth interspace, and the chest was entered. The nodule could be felt, but due to incomplete lung collapse as well as her anatomy and the thickened inferior pulmonary ligament, slightly increased visualization was required. Therefore, the access port was lengthened by several centimeters to facilitate exposure. At this point, then, the inferior pulmonary ligament could be further released carefully, and the nodule in the lower lobe was delivered up toward the small access port, then palpated more carefully. Several soft, mobile nodules were appreciated deep in the parenchyma of the posterior segment of the left lower lobe. This was grasped with a stump clamp, and then serial firings of an EZ45 thick-tissue stapler were able to successfully wedge it out with comfortably negative margins. It was sent to the back table and bivalved, with the margins grossly negative. The chest was irrigated copiously with hot water and antibiotic-containing irrigation and suctioned clear. Generous Tisseel treatment was applied. Pinpoint electrocautery was used for hemostasis and pneumostasis. Marcaine 0.25% 10 cc was injected subpleurally as an intercostal block. A single #28 straight chest tube was placed through anterior and inferior camera port incision and placed along the staple line, then directed toward the apex. It was sewn in with heavy silk ties. Two single pericostal sutures were placed carefully under direct vision and tied down. The lung was reinflated and filled the space nicely. The small wound was then irrigated, suctioned clear and closed in layers with absorbable sutures; running subcutaneous, subcuticular stitches and staples were applied. ESTIMATED BLOOD LOSS: Minimal. SPONGE AND NEEDLE COUNTS: Verified as correct x2 at the end of the procedure. DISPOSITION: The patient appeared to tolerate the procedure well and was pending awakening, extubation and transfer to the recovery room intensive care unit in satisfactory condition. SURGICAL ATTENDANCE: The services of the first assistant, James T. Wu, M.D., were required given the complexity of the case and the lack of otherwise experienced thoracic surgical assistants. ASSISTANT SURGEON(S): James T. Wu, M.D. If the assistant surgeon is other than a qualified resident, I certify that the services were medically necessary and there was no qualified resident available to perform the services.