Blair _Wormer_[NCSC_ACS_2013]
advertisement

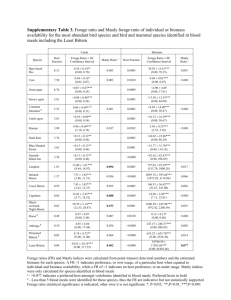
THE FIRST NATIONAL EVALUATION OF LAPAROSCOPIC VERSUS OPEN FUNDOPLICATION IN INFANTS Wormer BA, Schmelzer T, Bradley JF 3rd, Williams KB, Cosper G, Bambini DA, Heniford BT Background: Over the past decade, laparoscopic fundoplication (LF) has gained momentum as an alternative technique for treatment of antireflux in infants versus open fundoplication (OF). Our aim was to compare the two techniques using a large nationwide database. Methods: The Nationwide Inpatient Sample, which captures approximately 20% of all United States inpatient admissions, was queried from 2004-2010 for pediatric patients under 2 years of age who underwent LF or OF using ICD-9-CM coding. Demographics and outcomes were compared using Chi-square, Fisher’s exact test and Wilcoxon rank sums. Results: In total, 6,398 infants met inclusion; 2,102(33%) underwent LF and 4,296(67%) underwent OF. From 2004-2006, 3,115 fundoplications were performed, 703(23%) underwent LF and 2412(77%) underwent OF. From 2008-2010, 2,499 fundoplications were performed, 1091(44%) underwent LF and 1408(56%) underwent OF. Overall, the mean age was older for infants undergoing LF than OF (80±152 days old v. 57±133 days old; p<0.0001); there was no difference in gender or race. A higher proportion of infants undergoing LF had neurologic disorders than OF (17.2% v. 13.3%; p<0.0001). Postoperative pulmonary complications were lower in those undergoing LF than OF (4.0% v. 5.3%;p=0.0222), as well as decreased postoperative infections (1.7% v. 3.2%;p=0.0003), and postoperative gastrointestinal complications (1.6% v. 3.6%;<0.0001). Procedural bleeding was lower in those undergoing LF compared to OF (1.1% v. 2.4%;p=0.0004). Those undergoing LF had a lower overall postoperative complication rate (8.8% v. 14.7%; p<0.0001) and in hospital mortality (1.1% v. 3.2%; p<0.0001) than those undergoing OF. Days to fundoplication from admission was shorter for LF versus OF (24±37 v. 31±43;p<0.0001) and length of stay was significantly shorter in those undergoing LF versus OF (37±48days v. 50±58 days; p<0.0001). Total mean hospital charges were lower in those undergoing LF versus OF ($205,027±289,080 v. $228,485±273,948; p<0.0001). Both operations were performed predominately in urban hospitals; however a higher proportion of LF (90%) were performed at teaching hospitals than OF (84%) (p<0.0001). LF was also performed more often in areas of high median household income based on zip code than OF (40% v. 32%; p<0.0001). Conclusions: With the largest evaluation of fundoplication in infants to date, we have shown that outcomes of LF in infants mimic those in adults with decreased individual and overall postoperative complications in comparison to OF. However, unlike adults, LF has not become the predominate technique despite its increase in incidence over the last 7 years. Although LF appears to lead to decreased cost and length of stay, strong conclusions cannot be made due to the complicated long preoperative hospitalizations of the patients in our study sample.