Screw and Fin Implant
advertisement

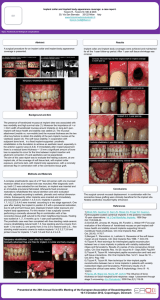
Information on Screw and Fin Implant Treatment 6 The Purpose of the procedure. Implants are man made roots to which dentures or crowns are attached. Implant Placement. Implants are placed in the jaws and left to heal for four to nine months before dentures or crowns are attached. The Number of Implants to be placed. All the necessary implants may be place at once or several implants can be placed to start with, followed by others later. Additional Procedures. Extra procedures may be found necessary at the time of implant placement. Occasionally, insufficient bone is found present. Bone from a bone bank may be added allowing implants to be placed then or later. There would be an additional fee for any extra procedures. Denture wearers. After placement of implants, the under surface of dentures may require modification to adapt to the implants. This may weaken the denture and breakage may occur. A repair may be necessary. The use of denture adhesive may help keep dentures in place during the healing period. The Final Restorative Procedures. Implants are left to become firmly attached to bone for six to nine months before a denture or crown and bridgework is fitted to them. Home Care. Implants, like teeth may suffer from gum disease resulting in loss of bone. Daily removal of plaque from implants will prevent this occurring. Immediate Post-operative Effects: Some patients have little or no problems at all. Some have bruising, swelling and discomfort. It is not possible to predict who has what after effects. Occasionally dizziness or mild loss of balance may be experienced. If this occurs telephone immediately Later Complications: The possibility of infection is low. If an implant does not heal in place satisfactorily, it will require removal and replacement later. Lower Implants: Occasionally numbness of the lip occurs after the procedure. This usually lasts a few weeks and occasionally several months. It is very rarely permanent. Smoking and Alcohol both reduce the success rates of implants. Success Rates of modern implants are very acceptable. Implants, like teeth, can be affected by gum disease and may require treatment. There would be no fee for the time spent on the treatment or replacement of an implant in the first year. However there would be a fee for materials used and the cost of the implant. 1 6 Alternative forms of Treatment Missing teeth may be replaced without implants with dentures and, if there are sufficient healthy natural teeth, by crown and bridgework. Timing. Avoid special business or social functions for about ten days. In the event that the procedure is unsuccessful I understand that it may be necessary to repeat the procedure and that there would be no charge for the time spent. However I will be required to pay the cost of any materials used and for a possible sedation fee. Please initial here to confirm you have read the above statement Initials ________ You may not want to work for a few days, up to 10 days. Questions : Please do not hesitate to ask, if you have any questions. 2 Consent Form for Implants. 6 This consent form is to make sure that you are fully informed about what implant treatment entails. 1. I have been informed and I understand the purpose and the nature of the implant surgery procedure. I understand what is required to place an implant under the gum or in the bone. 2. My dental surgeon has carefully examined my mouth. Alternatives to this treatment have been explained. I have considered these methods, but I want an implant to help secure the replaced missing teeth. 3. I have been informed of the possible risks and complications 4. I understand that if I am having lower implants placed there is a risk a lip numbness. I understand that if I am having lower implants placed there is a risk a lip numbness. This usually recovers in a few weeks but may last several months. In very rare cases it is permanent. Initial here to confirm you understand the above statement Initials ________ 5. My dental surgeon has explained that there is no method to accurately predict the gum and bone healing capability in each patient following the placement of the implant. 6. I understand that sometimes implants fail and must be removed. 7. I understand that excessive smoking, alcohol, or sugar may affect gum healing and may limit the success of implants. I agree to follow my dentist's home care instructions. I agree to report to my dentist for regular examinations as instructed. 8. I consent to photography of procedures for my records and the advancement of implant dentistry. 9. I fully understand that during and following the contemplated surgery or treatment, conditions may become apparent which warrant, in the judgment of the dental surgeon, additional or alternative treatment pertinent to the success of comprehensive treatment. I also approve of the modifications in design, materials, or care, if it is felt necessary by my dentist. 10. If at the time of treatment it is not possible to place implants I understand that the procedure will be discontinued and there will be a charge for time spent and for materials used. 11. I understand that implants like teeth require maintenance and occasional treatment such as gum treatment. I understand that there would be fees for the treatment and any materials used. 12. I understand that in the unlikely event that an implant should fail in the first year, there would be no fee for the replacement except the cost of the new implant and any materials used. 3 6 I have had the opportunity to ask questions regarding the placement of implants. I accept the use of Human Bone from a Bone bank Yes / No Initials_____________ I accept the use of Material derived from Pigs Yes / No Initials______________ I accept the use of Material derived from Cows Yes / No Initials____________ I accept the use of Material derived from Sheep Yes / No Initials______________ I have been informed that I will be treated in a teaching environment Initials______________ I have been informed that my treatment may be viewed by Students Initials ______________ I understand that some if not all of my treatment may be performed by Members of the Harpole Centre Faculty Initials ______________ I understand that my treatment will / will not be performed by Stuart Orton-Jones Initials ______________ That my treatment may be Videoed or Photographed Initials ______________ I have read and understood this consent form and have been given a copy to take home Initial _______________ I agree to the placement of............................implants If the procedure has to be re-done in the first year, I accept that I will be required to pay for the materials used and for the sedation Initials_____________________ I have read and understood this consent form and have been given a copy to take home Initials_____________________ Name ( Block Capitals)_______________________________________________ Patient's Signature………….........................................................Date........................... Dentist's Signature........................................................................Date........................... Stuart Orton-Jones Northampton, NN7 4 DH, UK.Telephone:- 01604 832399 Mobile:- 07885 349300 email stuart@sojinstitute.co.uk 33 High Street, Harpole, Fax:- 01604 832867 4 Postoperative Care to help healing. 6 For the next Few Days after Surgery. 1. Alcohol. Avoid alcohol for 2 weeks as this can affect the healing of the tissues. 2. Smoking. Avoid smoking for 3 days before treatment and 2 weeks after. Smoking slows down the healing process. 3. Avoid Very Hot Food and Drinks and spicy and acidic foods. 4 Avoid Hard Crusty Foods. 5. A surgical dressing may be placed around the incision after surgery. This should remain in place for one to two weeks. 6. Avoid Vigorously Brushing this area Clean gently. 7. Do not play with the area with your tongue, 8. If you have had a sinus graft procedure, or upper posterior implants placed, a) Please avoid blowing your nose for approximately 2 weeks after surgery. This will help prevent infection. b) Please try and sneeze through your mouth and not through your nose. c) Please avoid swimming for 2 weeks after surgery First and Second Week. 1. Rinse with Chlorhexidine ( Corsodyl ) twice a day. 2. Take antibiotics and pain relieving pills as prescribed. Finish the course of antibiotics. If you have a reaction to the medication, please telephone. 4. Avoid brushing the area. 5. Maintain a soft, high protein diet. 6. Avoid excessive physical exertion (i.e. sports, heavy lifting etc.). Third Week Lightly brush the area. 5 Fourth Week. Resume normal cleaning. 6 It is very important that you maintain your oral hygiene and home care at a high standard and that you attend for regular check-up appointments. I have been given the opportunity to ask questions about my treatment and understand the post-operative instructions. If anything concerns you at any time contact your dentist immediately. If you are not able to contact your Dentist, contact Stuart Orton-Jones. I have read this, have understood it and have a copy to take home. Patient's Name in BLOCK Capitals ___________________________________ Patient’s Signature_________________________________________________ Escort’s Name in BLOCK Capitals ___________________________________ Escort’s Signature_________________________________________________ Dentist's Name in BLOCK Capitals ___________________________________ Dentist’s Signature_________________________________________________ Stuart Orton-Jones 33 High Street Harpole Northampton England. Telephone:- 01604 832399 Fax:- 01604 832867 (Mobile) 07885 349300 6