ANOPHTHALMIC Posters
advertisement

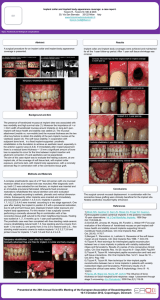
ANOPHTHALMIC SOCKET Intraoperative Modification of Porous Polyetylene Sheet for the Treatment of Enophthalmos Haytham Nasr, M D. Cairo University, Heliopolis, Cairo. Introductory Sentence: Enophthalmos can occur as a complication of neglected blow out fracture, resolved orbital abscess, after orbital tumor excision & in cases of anophthalmos. It leads to deep superior sulcus deformity with drooping of the upper eyelid as a result of lack of support.To treat this deformity, the orbital volume must be augmented. To achieve good esthetic results, the volume must be augmented posteriorly more than anteriorly. Posterior orbital augmentation raises the orbital fat up to fill the superior sulcus without raising the eye globe to avoid diplopia when the eye is there & seeing.. Methods: A retrospective study included 9 cases suffering from enophthalmos with superior sulcus deformity. Neglected blow out fracture in 5 cases , post-tumor excision in one case & enophthalmic anophthalmic socket in 3 cases. Porous polyethylene 105 mm thickness sheet was bent after hot water imersion then placed in a cold saline to mantain shape. the sheet is fashioned according the available subperiosteal space. It is fashioned in a way that it is flat anteriorly & bulging posteriorly to push the orbital fat up. Patients were followed for at least 3 months postoperatively. Results: Postoperative course was uneventful in all cases with minimal post operative pain in some cases. Parasthesia & hyposthesia were present in 6 cases & disappeared within 6 weeks. Full satisfaction was achieved in 7 cases & partial satisfaction in 2 cases. Conclusions: Intraoperatively designed & fashioned porous polyethylene sheet is a good solution to treat superior sulcus deformity resulting from enophthalmos. It can be used in anophthalmic cases as well as in cases with intact globe. It gives satisfactory results with minimal complications. Bibliography: Hawes MJ, Dortzbach RK. Surgery on orbital floor fractures: influence of time of repair & fracture size. Ophthalmology1983;90:1066-1070. Jordan DR, St Onge P, Anderson RL, Patrinely JR, Nerad JA Complications associated with alloplastic implants used in orbital fracture repair Ophthalmology - 1 October 1992 (Vol. 99, Issue 10, Pages 1600-1608) Author Disclosure Block: H. Nasr, None. The Use of Dermis Fat Graft in Infected Cases Haytham Nasr, M D. Cairo University, Heliopolis, Cairo. Abstract Body: Introductory Sentence: The presence of infected exposed integrated orbital implant is a stubborn complication, usually accompanied with failure of different techniques tried to cover the defect. Removal of the infected implant is mandatory to eradicate infection. In this study implant is removed & dermis fat graft is implanted as one stage operation instead of two staged operation. Methods: Ten children with infected exposed integrated orbital implant were entrolled in a retrospective study. In all cases the infected implamt was removed with trial to preserve the muscles. Dermis fat graft was harvested then sutured in place. A hard transparent silicone conformer was placed at the end of surgery. Patients were followed up for at least 6 months. Results: Satisfactory results with quiet postoperative course were achieved in 9 cases (90%). In one case, severe orbital cellulitis occurred which was controlled with massive parentral antibiotcs followed by drainage of pus. Conclusions: Implantation of dermis fat graft in the same sitting with removal of the exposed infected integrated orbital implant appears to be safe with high success rate. Dermis fat graft grows with the orbit in children leadin to a long term satisfactory results. Bibliography: Remulla HD, Ruben PAD, Shore JW, et al. Complications of porous spherical orbital implants. Ophthalmology,1995;102:586-593. Heher KL,Katowitz JA, Low JE. Unilateral dermis fat graft implantation in the pediatric orbit. Ophthal Plast Reconstr Surg 1998;14:81-88. Author Disclosure Block: H. Nasr, None. Hydroxyapatite Postenucleation Orbital Implant In Children: Long-Term Results In 374 Eyes Carol L. Shields, MD, Sara Lally, MD, Noel Perez, MD, Arman Mashayekhi, MD, Brian P. Marr, MD, Thaddeus Nowinski, MD. Wills Eye Hospital, Philadelphia, PA. Introductory Sentence: To evaluate results of scleral wrapped hydroxyapatite orbital implants in children Methods: Retrospective chart review of 374 cases of enucleation in patients age 20 years or less Results: The patients’ age ranged from 1 week to 20 years. Reasons for enucleation included retinoblastoma (88%), choroidal melanoma (3%), blind painful eye (3%), Coats disease (1%), medulloepithelioma (1%) and others (4%). Over a mean follow up of 6.2 years with range up to 15 years, complications included implant exposure (1%), implant infection (1%), conjunctival cyst (3%), and conjunctival pyogenic granuloma (1%). There were no cases of implant extrusion or orbital pain. Patients who had received prior chemoreduction (n=12) or external beam radiotherapy (n=22) showed no implant exposure, infection, or extrusion. Conclusions: In the long term, it appears that properly placed hydroxyapatite implants are well tolerated in the pediatric orbit. Bibliography: references to follow Author Disclosure Block: C.L. Shields, None; S. Lally, None; N. Perez, None; A. Mashayekhi, None; B.P. Marr, None; T. Nowinski, None. Pyogenic Granuloma, as a Presenting Sign of Hydroxyapatite Orbital Implant Exposure: A Clinicopathologic Study in five cases. Naser Owji, MD Ophthalmologist1, Alireza Sadeghipour, MD, Pathologist2, Perikala Vijayanadan Kumar1, Hossein Salour3. 1 Shiraz University of Medical Sciences, Shiraz, 2Iran University of Medical Sciences, Trhran, 3Shahid Beheshti University of Medical Sciences, Tehran. Introductory Sentence: Pyogenic granuloma, as a complication of H.A orbital implant, occurs infrequently in the absence of a peg , and was reported as a minor complication of H.A orbital implant in previous reports 1. The purpose of this article is to report the unusual cases with exposed hydroxyapatite orbital implants, presenting with pyogenic granuloma. Methods: Five patients with pyogenic granuloma on the hydroxyapatite orbital implant, with underlying exposure defect, were studied. Explantation of the implant was done due to recurrent pyogenic granuloma and very large exposure defect in two cases (fig1). Simple excision of the lesions and direct repair of the underlying exposure defects were performed in three patients. Results: The pyogenic granulomas were detected 1.5 to 30 months after implantation in five patients. In contrast to previously reported pyogenic granuloma on the ocular surface 2, the present lesions were multiple, not related to the wound margin in most instance, and were not covered by the surface epithelium (fig2). Exposure defects were detected at the time of the lesions excision in four patients. But, pyogenic granuloma was developed on the old exposed area in the fifth patient at follow-up priod. Slit lamp examination revealed penetrating fibrovascular tissues from the wound margin to the interconnecting pores. Fibrovascular cord traverse horizontally and then originate from the superficial pores on the exposed area as granulation tissue buds and pyogenic granulomas (fig3). Mean exposure size in largest dimension was 16 mm (range 9-20 mm). Histopathologic examination of the explanted hydroxyapatite disclosed chronic inflammation and micro abscess formation (fig4). Foci of osteoinduction were noted (fig5). Also there was a layer of residual surface epithelium on anterior part of hydroxyapatite ball which seems to be originated from border of conjunctival dehiscence and displayed a down growth pattern of proliferation into anterior pores and extending centrally for 3-4 mm (fig6). Conclusions: Pathogenesis of pyogenic granulomas on exposed hydroxyapatite implant differ from previously presented one in ocular surface. Pyogenic granuloma should not be considered a benign lesion on the hydroxyaptite orbital implant, especially in recurrent one. It should be alert the ophthalmologist to the possible of conjunctival dehiscence with hydroxyaptite exposure beneath the lesion. Bibliography: 1-Jordan DR, Bawazeer A. Experience with 120 synthetic hydroxyapatite orbital implants (FCI3). Ophthal Plast Reconstr Surg 2001; 17: 184-90. 2 - Liszaure AD, Brownstein S, Codere F. Pyogenic granuloma on a dermis fat graft in acquired anophtalic orbits. Am J Ophtalmol 1987; 104; 641-44. Author Disclosure Block: N. owji, None; A. Sadeghipour, None; P.V. Kumar, None; H. Salour, None. Comparison Of Exposure Rate In Different Wrapping Materials For Hydroxyapatite Orbital Implant. Jin S. Yoon, M.D., Jung B. Choi, M. D., Kyung H. Kook, M.D., Sang Y. Lee, M.D.. Yonsei medical univeristy,Severance hospital Eye center, Seoul. Introductory Sentence: Wrapping the implant may help the surgeon insert it into the orbit more smoothly during the procedure and protect the anterior part of orbital soft tissues from rough surfaces, in addition to providing attachment sites for the extraocular muscles. We compared the postoperative complication such as implant exposure of three wrapping materials for hydroxyapatite(HA) ocular implantation (vicryl mesh, Tutoplast® and autologous sclera) Methods: This study was a retrospective, interventional, comparative case series of 174 consecutive patients who received HA implantation using three different wrapping materials from March 1997 to October 2004. Especially, autologous sclera was used as the wrapping material in case with phthisis bulbi having insufficient sclera to perform evisceration or with previous eviscerated eye. As sclera was insufficient to cover whole surface of implant in most cases, especially in severely consticted eviscerated eye with small implant, we unfolded the consticted autologous sclera and wrapped the anterior surface of the hydroxyapatite remaining the posterior part uncovered. In case of intraocular malignancy or unremained sclera, the choice of wrapping materials were vicryl mesh or Tutoplast ®. Results: We used vicryl mesh in 65 eyes, Tutoplast® in 72 eyes, and autologous sclera in 37 eyes. Implant exposure developed in 4 eyes (6%) using vicryl mesh which occurred in 2-5 (mean 3.5) months, but no exposure developed in eyes using Tutoplast® and autologous sclera. Conclusions: When using vicryl mesh as the wrapping material, it is advisable to pay more attention to the possibility of implant exposure than using Tutoplast® or autologous sclera. Coarse surface of vicryl mesh irritating tenon’s capsule and conjunctiva might be a reason of higher exposure rate. By using autologous sclera, fibrovascular proliferation can be facilitated through the posterior part of the implant not covered by autologous sclera and anterior part covering coarse surface of HA would prevent exposure. Bibliography: Jordan DR, Allen LH, Ells A, et al. The use of Vicryl mesh (polyglactin 910) for implantation of hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg. 1995;11:95-99. Oestreicher JH, Liu E, Berkowitz M. Complications of hydroxyapatite orbital implants. A review of 100 consecutive cases and a comparison of Dexon mesh (polyglycolic acid) with scleral wrapping. Ophthalmology. 1997;104:324-329. Shields CL, Shields JA, De Potter P, Singh AD. Lack of complications of the hydroxyapatite orbital implant in 250 consecutive cases. Trans Am Ophthalmol Soc. 1993;91:177-189 Author Disclosure Block: J.S. Yoon, None; J.B. Choi, None; K.H. Kook, None; S.Y. Lee, None. Alternating Layered Flap (ALF) Technique for Scleral Closure in Evisceration with Ball Implant Mohammad A. Hafez, MD,FRCS, Erfan A. Elgazayerli, Ph.D. Magrabi Eye hospital, Cairo Egypt. Abstract Body: Purpose: The main disadvantage of evisceration is implant extrusion. In the classic evisceration,the corneoscleral button is removed .In many cases,this button is healthy and even thicker than the normal tissue. In our study,instead of removing the button, we used it to fashion four flaps to be closed in an alternaing way to add more protection to the implant anteriorly. Methods: 80 Consecutive cases were enrolled. Cases were subjected to surgery using the new technique and biointegrated balls were implanted. Follow up ranged from 6 months to 2 years. Results: Early postoperative wound healing problems occurred in only 4 cases (5%). Late postoperative implant exposure occurred in only 2 cases (2.5%). Smooth dome shaped quiet bulbar surface was achieved in 76 cases (95%). Prosthetic wear comfort was achieved subjectively in 72 cases (90%) .Disadvantages of the new technique are that it is more time consuming and it does not apply to eyes with corneal melting or thinning. Conclusion: The new technique reduces postoperative wound healing problems and implants exposure while allowing a more comfortable prosthetic wear and mobility. Bibliography: 1-John A. Long, Thomas M. Tann III, Christopher A. Girkin. Evisceration: A New Technique of Trans-Scleral Implant Placement. Ophthalmic Plastic and Reconstructive Surgery 2000;16:5:322-325. 2-Guy G. Massry, John B. Holds. Evisceration With Scleral Modification. Ophthalmic Plastic and Reconstructive Surgery 2001;17:1:42-47. Author Disclosure Block: M.A. Hafez, None; E.A. Elgazayerli, None.