internal jugular _____ lumen port placement
advertisement

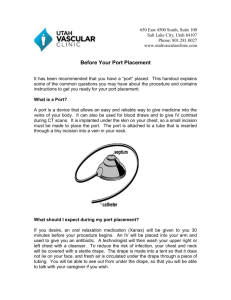
PGCHPORT PROCEDURE: Ultrasound and fluoroscopic-guided _ internal jugular _ lumen port placement. CLINICAL INDICATION: _ PHYSICIAN: Dr. Paul Gryzenia MEDICATIONS: _ COMPLICATIONS: None immediate. RADIOLOGIST INTRASERVICE TIME/CONSCIOUS SEDATION TIME: _ minutes. The patient was monitored throughout the procedure by the IR nurse. I was personally present in the above mentioned conscious sedation time. PROCEDURE AND FINDINGS: After discussing the risks and benefits of the procedure with the patient, oral and written consent was obtained. The patient was placed in a supine position on the fluoroscopy table. The patient was prepped utilizing maximum sterile barrier technique. Initial sonographic evaluation of the _ internal jugular vein demonstrated a patent and compressible _ internal jugular vein. A stored sonographic image was obtained. The _ neck and upper chest were prepped and draped in the usual sterile fashion. Using sonographic guidance and local anesthesia, the _ internal jugular vein was accessed with a 22 gauge microaccess needle with the aid of a 0.018 inch guidewire. The guidewire was advanced into the superior vena cava and the needle was exchanged for a short 5-French microaccess sheath. Through this, a 0.035 inch guidewire was advanced into the inferior vena cava. Subsequently, over the guidewire, an 8-French peel-away sheath was inserted. Under suspended respiration, a 6-French catheter was inserted through the peel-away sheath to the level of the cavoatrial junction. Attention was then directed to the _ chest wall. A small incision was made over the _ upper chest and a subcutaneous pocket was created using blunt dissection. The port was then secured to the deep tissues using two 3-0 Vicryl sutures. A subcutaneous tunnel was then created from the incision site to the venotomy and the catheter was pulled through the tunnel. The catheter was retracted so that the distal tip of the catheter was noted at the level of the atriocaval junction. Subsequently, the catheter was cut and attached to the port. The port was then accessed with a Huber needle and aspirated and flushed well. The port was then placed within the pocket and secured with two sutures. The incision was closed using a single running subcuticular 3-0 Vicryl suture. In addition, the incision site was closed using skin glue. The venotomy was closed with a single 3-0 Vicryl suture and skin glue. The port was then accessed and flushed with heparin flush (heparin 100 units/cc). The final fluoroscopic image demonstrates the port in satisfactory position with the distal tip at the level of the atriocaval junction. The patient tolerated the procedure well without immediate complication. IMPRESSION: Successful insertion of a _ internal jugular _ lumen port with distal tip at the level of the cavoatrial junction. The port is ready for use. CPT 6030F