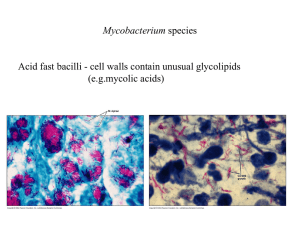
Culture of pediatric respiratory specimens for M
advertisement

Comparison of Yield for Different Culture Collection Methods Gastric aspiration is the classic method of culture collection. Classically, three gastric aspirates are collected first thing in the morning after an overnight fast. Traditionally, the yield is reported to be around 40%, with increased yield in patients who are sicker, have more extensive pulmonary disease, have parenchymal disease (rather than just intrathoracic adenopathy) and who are very young. Yields in infants may be as high as 75%. The first gastric collected has the highest yield with 8893% of the positive results coming from the first specimen collected. Starke JR. Taylor-Watts KT. Tuberculosis in the pediatric population of Houston, Texas. Pediatrics. 84(1):28-35, 1989 Schaaf HS. Gie RP. Kennedy M. Beyers N. Hesseling PB. Donald PR. Evaluation of young children in contact with adult multidrug-resistant pulmonary tuberculosis: a 30-month follow-up. Pediatrics. 109(5):765-71, 2002 Kimerling ME. Vaughn ES. Dunlap NE. Childhood tuberculosis in Alabama: epidemiology of disease and indicators of program effectiveness, 1983 to 1993. Pediatric Infectious Disease Journal. 14(8):678-84, 1995 Al-Dossary FS. Ong LT. Correa AG. Starke JR. Treatment of childhood tuberculosis with a six month directly observed regimen of only two weeks of daily therapy. Pediatric Infectious Disease Journal. 21(2):91-7, 2002 Lobato MN. Loeffler AM. Furst K. Cole B. Hopewell PC. Detection of Mycobacterium tuberculosis in gastric aspirates collected from children: hospitalization is not necessary. Pediatrics. 102(4):E40, 1998 Vallejo JG. Ong LT. Starke JR. Clinical features, diagnosis, and treatment of tuberculosis in infants. Pediatrics. 94(1):1-7, 1994 Schaaf HS. Beyers N. Gie RP. Nel ED. Smuts NA. Scott FE. Donald PR. Fourie PB. Respiratory tuberculosis in childhood: the diagnostic value of clinical features and special investigations. Pediatric Infectious Disease Journal. 14(3):189-94, 1995 Berggren Palme I. Gudetta B. Bruchfeld J. Eriksson M. Giesecke J. Detection of Mycobacterium tuberculosis in gastric aspirate and sputum collected from Ethiopian HIV-positive and HIV-negative children in a mixed in- and outpatient setting. Acta Paediatrica. 93(3):311-5, 2004 Mar. UI: 15124831 Gomez-Pastrana D. Torronteras R. Caro P. Anguita ML. Lopez-Barrio AM. Andres A. Navarro J. Comparison of amplicor, in-house polymerase chain reaction, and conventional culture for the diagnosis of tuberculosis in children. Clinical Infectious Diseases. 32(1):17-22, 2001 Pomputius WF 3rd. Rost J. Dennehy PH. Carter EJ. Standardization of gastric aspirate technique improves yield in the diagnosis of tuberculosis in children. Pediatric Infectious Disease Journal. 16(2):222-6, 1997 From Pediatric TB: An Online Presentation by Ann Loeffler, MD. Produced by the Francis J. Curry National Tuberculosis Center. Sputum induction Sputum can be collected from even very young children by inducing cough and sputum production with nebulized saline or bronchodilators and then asking the patient to expectorate the sputum OR suctioning the back of the pharynx to collect sputum. The recovery rate for sputum induction was 22% (Zar 2005), 28% (Shata 1996), and 30% (Iriso 2005) in children suspected of having pulmonary TB. Zar HJ. Hanslo D. Apolles P. Swingler G. Hussey G. Induced sputum versus gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: a prospective study. [erratum appears in Lancet. 2005 Jun 4-10;365(9475):1926]. Lancet. 365(9454):130-4, 2005 Jan 8-14. Zar HJ. Tannenbaum E. Hanslo D. Hussey G. Sputum induction as a diagnostic tool for communityacquired pneumonia in infants and young children from a high HIV prevalence area. Pediatric Pulmonology. 36(1):58-62, 2003 Zar HJ. Tannenbaum E. Apolles P. Roux P. Hanslo D. Hussey G. Sputum induction for the diagnosis of pulmonary tuberculosis in infants and young children in an urban setting in South Africa.[see comment]. Archives of Disease in Childhood. 82(4):305-8, 2000 Shata AM. Coulter JB. Parry CM. Ching'ani G. Broadhead RL. Hart CA. Sputum induction for the diagnosis of tuberculosis. Archives of Disease in Childhood. 74(6):535-7, 1996 Iriso R. Mudido PM. Karamagi C. Whalen C. The diagnosis of childhood tuberculosis in an HIV-endemic setting and the use of induced sputum. International Journal of Tuberculosis & Lung Disease. 9(7):71626, 2005 BAL Bronchoalveolar lavage (BAL) is particularly helpful in patients in whom the cause of pulmonary disease or infection is not known. Various studies have reported M. tuberculosis BAL yields of 4% (Bibi 2002), 10% (Abadco 1992), 12% (Somu 1995), 21% (Norrman 1988), 22% (Singh 2000) and 43% (Petrovic 2005) from children suspected of having pulmonary tuberculosis. Petrovic S. [Diagnostic value of certain methods for isolation of Mycobacterium tuberculosis in children with suspected pulmonary tuberculosis]. [Serbian] Medicinski Pregled. 58(5-6):231-5, 2005 Bibi H. Mosheyev A. Shoseyov D. Feigenbaum D. Kurzbart E. Weiller Z. Should bronchoscopy be performed in the evaluation of suspected pediatric pulmonary tuberculosis? Chest. 122(5):1604-8, 2002 Singh M. Moosa NV. Kumar L. Sharma M. Role of gastric lavage and broncho-alveolar lavage in the bacteriological diagnosis of childhood pulmonary tuberculosis. Indian Pediatrics. 37(9):947-51, 2000 Somu N. Swaminathan S. Paramasivan CN. Vijayasekaran D. Chandrabhooshanam A. Vijayan VK. Prabhakar R. Value of bronchoalveolar lavage and gastric lavage in the diagnosis of pulmonary tuberculosis in children. Tubercle & Lung Disease. 76(4):295-9, 1995 Norrman E. Keistinen T. Uddenfeldt M. Rydstrom PO. Lundgren R. Bronchoalveolar lavage is better than gastric lavage in the diagnosis of pulmonary tuberculosis. Scandinavian Journal of Infectious Diseases. 20(1):77-80, 1988 Abadco DL. Steiner P. Gastric lavage is better than bronchoalveolar lavage for isolation of Mycobacterium tuberculosis in childhood pulmonary tuberculosis. Pediatric Infectious Disease Journal. 11(9):735-8, 1992 From Pediatric TB: An Online Presentation by Ann Loeffler, MD. Produced by the Francis J. Curry National Tuberculosis Center.