Bordetella pertussis
advertisement

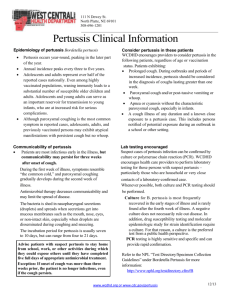
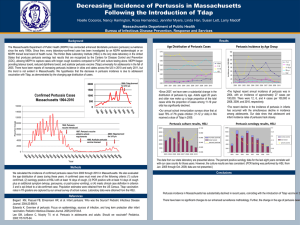
Bordetella species of clinical importance B. pertussis B. parapertussis B. bronchosepticus A 2-year-old male is presented to you with a 10-day history of persistent cough. The long cough spells are followed by a deep breath. The cough often leads to choking, vomiting, gasping and cyanosis. His pulse rate is 190 (n: 100-160) and respiratory rate is 72 (n: 10-20). Chest x-ray is normal. WBC counts are16,000/cm2 with 70% lymphocytes. 1. 2. 3. 4. What is the organism and what are its physiologic characteristics? What are the pathogenic factors of this organism? Why is there a preponderance of lymphocytes? What is the epidemiology of and prophylaxis for the disease? Bordetella pertussis Causative agent of whooping cough Gram negative cocobacillus Requires special media to grow Bordetella pertussis Gram negative coccobacilli Small, transparent hemolytic colonies on BG medium Oxidase+,Urease-; (B. parapertussis: oxidase-, urease+; B. brochosepticus: +/+) Pertussis: epidemiology pertussis is a disease mainly of children Pertussis: course of disease Pertussis: virulence factors Pertussis toxin (pertussigen)* Adenylate cyclase toxin Tracheal toxin Dermonecrotic toxin Filamentous haemagglutinin* Lipopolysaccharide Pertussigen: (an AB-toxin, oligopeptide) Increases histamine and LPS sensitivity Increases IgE levels T-cell lymphocytosis Impairs phagocyte functions ADP-ribosylates the Gi protein (results in increased cAMP) Pertussigen: Structure Pertussigen: dysregulation of adenylate cyclase Pertussis toxin Cholera toxin ATP cAMP Pertussis: adenylate cyclase toxin Activated by calmodulin Catalyses ATP to cAMP conversion cAMP Pertussis tracheal Toxin A peptidoglycan-like molecule Binds to ciliary epithelial cells Inhibits ciliary movement Kills ciliary ciliary epithelial cells Causes pertussis Pertussis: dermonecrotic toxin Strong vasoconstrictor Causes ischemia Synergizes with tracheal toxin to causes tracheal necrosis Pertussis: filamentous haemagglutinin Causes binding of bacteria to ciliated epithelial cells B. pertussis: interactions with pneumocyte B. pertussis: lipopolysaccharide Activates inflammatory cytokines Activates complement In larger quantities, causes shock and cardiac arrest Pertussis: diagnosis Based on symptoms Culture on Bordet-Gengou (potato- glycerol-blood agar) medium Laboratory Diagnosis Specimens Post / per nasal swab (no cotton swab) / cough plate Microscopy Gram negative coccobacilli Fluorescent antibody stain Culture Bordet – Gengou Medium mercury drop pearl appearance colonies Identification Microscopy & slide agglutination Antibiotic Erythromycin / Co-trimoxazole Pertussis: treatment Erythromycin is the drug of choice Vaccine is extremely effective Immunization 1st Pertussis vaccinewhole cell Combination vaccines Diphtheria Primary Acellular vaccine now used D P Pertussis 3 doses Intervals of 4 - 6 wks 4th dose year after T VACCINE Tetanus Booster School entry A 2-year-old male is presented to you with a 10-day history of persistent cough. The long cough spells are followed by a deep breath. The cough often leads to choking, vomiting, gasping and cyanosis. His pulse rate is 190 (n: 100-160) and respiratory rate is 72 (n: 10-20). Chest x-ray is normal. WBC counts are16,000/cm2 with 70% lymphocytes. 1. 2. 3. 4. What is the organism and what are its physiologic characteristics? What are the pathogenic factors of this organism? Why is there a preponderance of lymphocytes? What is the epidemiology of and prophylaxis for the disease?