AVULSION
advertisement

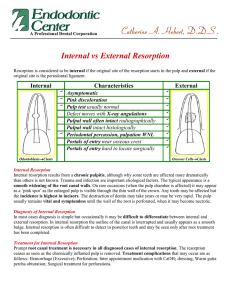
AVULSION AVULSION ( EXARTICULATION OR TOTAL LUXATION ) DEFINITION : The tooth is displaced totally out of it’s socket. CLINICAL APPEARANCE The socket is found empty or filled with coagulum. EPIDEMIOLOGY • Rare injuries(1.6% of dental injury) • Primary dentition > secondary dentition • Boys > girls • The teeth most commonly damaged are upper central incisor ETIOLOGY • Cause: accident contact sports fighting • Predisposing factor : Cl II malocclusion Periodontal disease HISTORY TAKING • When did the injury take place ? • Where did the injury take place ? • How did the injury take place ? HISTORY TAKING • Has treatment been provided elsewhere ? • Has there been previous trauma ? • Has avulsed tooth been accounted for ? HISTORY TAKING » MEDICAL HISTORY » DENTAL HISTORY » SOCIAL HISTORY » FAMILY HISTORY Neurological Assessment - Obtain information : loss of consciousness, neck or head pain, and numbness - Ask about the event…. amnesia? - Other signs: nausea, vomiting, drowsiness, blurred vision EXTRAORAL EXAMINATION • • • • Facial wound Fracture of mandible / maxilla Occlusion Mandibular movement INTRAORAL EXAMINATION • Solf tissue • Foreign body • Alveolar bone fracture RADIOGRAPHIC EXAMINATION • Are routinely to determine the socket • Check for supporting structure and adjacent tooth • Compare with the future radiographs RADIOGRAPHIC EXAMINATION TREATMENT OF AVULSED TOOTH Success of treatment depend on »Extraoral time »Storage media »Stage of tooth development EXTRAORAL TIME • After 60 minutes of dry storage media very few PL cells remain viable. • 120 minutes - complete PL cells necrosis. STORAGE MEDIA – Hank’s balance salt solution (HBSS) – Milk – Saliva – Water TREATMENT OF AVULSED TOOTH • • • • • Preparation of the avulsed tooth Preparation of the socket Replantation Splinting Follow up PREPARATION OF THE AVULSED TOOTH • Saline to remove foreign bodies • Avoid scraping the root surface PREPARATION OF THE SOCKET • The region should be anesthetized • Gently clean with NSS to remove clotted blood and foreign materials PREPARATION OF THE SOCKET REPLANTATION • Press the tooth gently into the socket • Compress buccal and lingual plate of bone • Take radiograph immediately REPLANTATION SPLINTING Requirements of splint • Provide stabilization for the replanted tooth • Slight physiologic movement • Hygienically designed • Not leave the replanted tooth in traumatic occlusion SPLINTING • Wire composite splint • Composite splint • Removable flexible acrylic splint • Orthodontics wire • Etc. SPLINTING SPLINTING How long? the fixation period should be sufficient to allow the reattachment of PDL. This will take from 1 – 3 weeks. FOLLOW UP A well designed follow up procedure is diagnose complication. • 1 week. • 2 weeks. • 3 weeks. A radiographic examination is able to demonstrate periapical radiolucency FOLLOW UP • 6 weeks. A clinical and radiographic examination A clinical and radiographic examination is able to demonstrate most case of inflammatory resorption FOLLOW UP • 2 and 6 months. Optional for cases with questionable healing • 1 year. A clinical and radiographic examination can ascertain the long – term prognosis WOUND HEALING AFTER REPLANTATION • Surface resorption • Replacement resorption • Inflammatory root resorption Surface resorption Surface resorption is manifested as a excavations on the root surface without associated breakdown of the lamina dura. Surface resorption Replacement resorption Replacement resorption (ankylosis) is initially seen as a disappearance of PDL space, later follow by a substitution with bone. Replacement resorption • PDL injury -> inflammation -> osteoclastic activity -> fusion between bone and root surface Inflammatory resorption Inflammatory resorption is seen as bowl shaped cavities on the root surface with an associate radiolucency affecting the lamina dura. Inflammatory resorption Summary The influence of storage conditions on the clonogenic capacity of periodontal cell : implication for tooth replantation P.C. Lekic , D.J. Kenny & E.J. Barrett International Endodontic Journal (1998)31,137-140 INTRODUCTION • Viable periodontal ligament (PL) cells are required for the healing of avulsed teeth after replantation. INTRODUCTION • The viability of PL cells in extra- alveolar conditions may be extended by incubating the avulsed tooth in a physiologic storage medium. INTRODUCTION • Regeneration of PL following replantation is closely related to preservation of the viability PL cells that adhere to avulsed teeth OBJECTIVES • To investigate the effects of combinations of storage media on the clonogenic capacity of human PL cells at two different extra alveolar period. MATERIALS AND METHODS • 20 human premolar teeth were extracted • Aged 11 – 14 years • 4 storage media (saliva , milk , HBSS , MEM) • All teeth were assayed at 30 and 60 min MATERIALS AND METHODS Twenty extracted human premolars Time 15 teeth 0 min Saliva (23c) 5 teeth 5 teeth MEM (+4c) Per condition 15 min 30 min Milk Saliva HBSS MEM (+4c) One-half of PL tissue explanted from premolar(cells released and analyzed for clonogenic capacity) RESULTS % of cells with clonogenic capacity 25 MEM 20 Milk HBSS 15 Saliva 10 5 0 30 60 Time (min) Results of clonogenic capacity assay CONCLUSION • Immediate storage of a avulsed teeth in autologous saliva , a followed by transfer to chilled milk , preserves the presence of sufficient progenitor cells in the PL to warrant replantation and the possibility of PL healing at 60 min extra-alveolar duration. Any Questions? Thanks for your attention REFERENCES • Peter J. Robinson,Louis H. Grernsey: Clinical Transplantation in Dental Specialties.C.V.Mostby,Missouri,1980 • G.J.Robert,P.Longhurst: Oral and Dental Trauma in Children and Adolestcents,Oxford university press Inc. New York, 1996 • Mitsuhiro Tsukiboshi: Autotransplantation of Teeth,Quintessence,Tokyo,2001 • J.O.Andreasen,F.M.Andreasen,L.K.Bakland, et al: Traumatic Dental Injury.Munksgaard.Copenhagen,1999 • M.E.J.Curzon: Handbook of Dental Trauma,Wrigth,Jordan Hill,Oxford,1999