Common Intestinal Worms
Nematodes
Introduction
The warm regions of
the world are also the
worm regions. In the
rural villages and
unsanitary
overcrowded cities of
the tropics, infection
with the 'big three'
(Ascaris, Trichuris &
Hookworm) is so
common that it Is
accepted as a natural
phenomenon.
Continued
Because these infections are rarely fatal, and
their control seems such a formidable
undertaking, relatively little effort has been made
to free the world of its worm burden. This
complacency is hardly warranted; the most
common intestinal nematodes can cause
considerable morbidity particularly when the host
is already weakened by malnutrition and
concurrent disease"
R DESOWITZ
Question 1
What types of Intestinal worms do you know?
Answer 1
Nematodes
(Round Worm)
Cestodes
(Flatworm)
Trematodes
(Flukes)
The three large families
are the Nematodes,
the Cestodes and the
Trematodes, each of
which has members
of importance as
causes of childhood
illness. Nematodes
will be discussed in
this programme, and
Cestodes and
Trematodes in the
next.
Question 2
How common is worm infestation in South
African children?
Answer 2
The prevalence of childhood parasitic infections in
some areas will be seen in the following graph,
taken from a study by Taylor et al in Southern
Kwazulu/Natal (2). Many patients host more than
one parasite.
Contd...
Continued
Prevalence of Parasitic Infestations
Kwazulu/Natal
A. lumbricodes
T. trichiura
Coa stland
82%
96%
Inland
81%
57%
Total
81%
81%
A. Duodenale
S. haematobium
H. nana
44%
6%
2%
4%
2%
2%
29%
4%
2%
Taenia spp.
G. lamblia
18%
4%
3%
2%
13%
Contd ...
Continued
The lack of clean water and adequate sanitation
are major contributors to infestation and
reinfestation, while the extent of morbidity
(illness) is proportional to the intensity of
infestation.
Question 3
What are the anatomical characteristics of the
nematodes?
Answer 3
NEMATODES
The worms are round in cross-section
unsegmented
possess mouth, oesophagus and anus
generally have separate sexes
reproduction - oviparous/larviparous
Contd ...
Continued
Ascaris is commonly referred to as 'roundworm",
but a number of other worms belong to the
roundworm or nematode family. Name a few.
Continued
Members of the Round Worm Family
Ascaris lumbricoides
Trichuris trichuria
Ankylostoma
Enterobius vermicularis
Strongyloides stercoralis
Filaria
Trichinella
Toxocara
3 continued
The most important in Southern Africa, apart from
ascaris, are trichuris (whipworm) , ankylostoma
(hookworm) and enterobius (thread- or pinworm) .
Although infestation is more prevalent in tropical
and subtropical climates, those living in
temperate and cold climates are not spared.
Question 4
What are these
worms?
Answer 4
Adult roundworms - Ascaris lumbricoides
Ascariasis is the most prevalent of all human
helminthic infections, with an estimated 1 billion
Individuals affected throughout the world.
Children are generally more heavily infected than
adults and are therefore more likely to suffer
pathological consequences from these infections.
4 continued
Ascaris prefers warm moist climates - in some
areas of the Pacific 94% of children are affected.
Eggs are killed by dry heat. Nevertheless,
infection still occurs in caller climates - There are
more than 4 million affected children in
N.America.
Question 5
What is the size of the worm?
Answer 5
Ascaris is the largest roundworm. It may reach up
to 40 centimetres in length. it is a white-pink
colour and tapers at both ends. The male can be
distinguished by his curved posterior end. The
female has a lifespan of 1 - 2 years and is capable
of producing 200 000 eggs per day !!
Question 6
Describe the life-cycle
Answer 6: Life Cycle of Ascaris
Live eggs in
dust or soil,
child swallows
eggs
Larvae mature into
adult worms in gut
Larvae penetrate
gut wall enter
blood stream
Larvae enter small
bronchi up trachea
and down
oesophagus
Contd ...
Continued
Ascariasis is a soil-transmitted Infection.
Transmission depends on the dissemination of
eggs In environmental conditions suitable
for their maturation. Human fingers are
contaminated by soil contact and live eggs
transmitted to the mouth. Alternatively
food Items such as vegetables may become
infected. Eggs are ingested by human host, and
hatch in the duodenum.
6 continued
The larvae/embryos penetrate the intestinal wall and
migrate to the lungs via the portal venous or
lymphatic circulations. Once in the lungs, these
larvae break out into the alveoli, pass up the
bronchi. are swallowed and re-enter the intestine
where the adult worm matures. The worms lie free
In the bowel and do not attach
to or damage the mucosa.
Question 7
What does the next
slide show?
Answer 7
Fertilised eggs of Ascaris. which have a rounded
shape and corticated outer shell.
Unfertilised eggs may also be seen in faeces. They
have an ellipsoidal shape and indistinct internal
structure. They may be seen in children who
harbour only female worms.
Question 8
What are the clinical features?
Answer 8
In the majority the infestation is completely
asymptomatic.Symptoms are commonly
attributed to Ascaris because the worms tend
to migrate and be vomited, or passed in the stool
when the child is ill for whatever reason.
8 continued
Clinical features of Round Worm Infestation
Pulmonary infiltration
- cough,sputum
- pneumonitis
- wheeze & bronchospasm
Gastrointestinal
- worm passed through mouth, anus, nose
- vague symptoms (abdominal)
- obstruction
-complications of obstruction
8 Continued
Worms may escape
from mouth, anus,
nose
With heavier worm loads
a tangled mass of
worms can obstruct
the bowel, or an
individual worm can
block a duct.
Contd ...
8 Continued
Vague abdominal symptoms - pain and
distension
obstruction with sudden onset of colicky
abdominal pain and vomiting, possibly bilestained.
complications of obstruction - bowel wall
necrosis, perforation, volvulus, ischaemia and
gangrene
Clinical features of
Roundworm continued.
Biliary tract
- rarer manifestations
Liver
- parenchymal penetration
- secondary infection
Pancreatic duct
- pancreatitis
Cont...
8 continued
A worm may block the lumen of the appendix
causing acute appendicitis.
A worm may migrate up the bile duct and present
with colicky abdominal pain in the right upper
quadrant, nausea, vomiting and fever.
RARELY: jaundice, calculi, strictures.
May penetrate the liver parenchyma causing a
granulomatous inflammatory reaction, secondary
infection and abscess formation.
8 Continued
Obstruction of the pancreatic duct may lead to
pancreatitis.
Worms may even turn up in distant parts of the
body.
If migration of larvae through the lungs is heavy
and/or repeated, marked hypersensitivity
develops.
This is a common cause of wheeze and
bronchospasm
8 Continued
Pulmonary infiltration with recurrent cough, and
bloodstained sputum
Eosinophilia and raised serum lgE.
Question 9
What steps would you take to arrive at a
diagnosis?
Answer 9
Stool microscopic examination for ova Straight Xray of abdomen may show - Worms
partial/complete obstruction Ultrasound - very
useful to show worms in biliary tract Amylase - if
pancreatitis is suspected Barium Meal or IV
cholangiography may be required.
Question 10
Suspicion is the first step to diagnosis !
What is the treatment ?
Answer 10
• Mebendazole 109mg twice a day for 3 days OR
• Albendazole 400 mg as a single dose
These are safe and highly effective treatments for
uncomplicated intestinal ascariasis
Piperazine syrup causes neuromuscular
paralysis and rapid expulsion of worms. It is the
best drug for intestinal and biliary obstruction as
the worms are not killed.
Cont...
Continued
It is given before the evening meal in a dosage of
75 mg/kg to a maximum of 4 9
Piperazine sometimes causes sensitivity and
neurotoxic reactions.
Chemotherapy is not useful against the
pulmonary phase of the infection. Larval
pneumonitis responds dramatically to
corticosteroids
Question 11
What prevention and control measures would you
suggest?
Answer 11: Preventive
Measures
Sanitary practice in faecal disposal
Good hygienic practices with food
Regular hand washing
Mass de-worming programmes
11 Continued
Sanitary practices of faecal disposal, are the
most effective long-term measure. Good hygienic
practices with food, and regular washing of
hands should be propagated. Mass de-worming
programmes, repeated at 3-6 month intervals,
have been advocated in areas of high prevalence.
Question 12
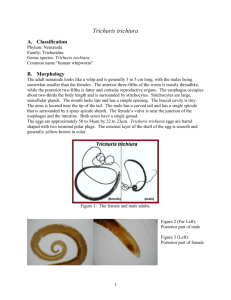
What Is this parasite?
Answer 12
A
TRICHURIS
-
trichiura
Also known as whipworm, it is one of the most
common helminthic Infections In humans. There
are approximately 112 billion cases world-wide,
and infection is common in South Africa.
Trichuris prefers warm climates, but like Ascaris
may also be found in cold regions.
Cont...
Answer 12 continued
Trichuris has an anterior whip like portion (the
head end) and a posterior bulky part. They
measure approximately 40 mm. The worm
remains in the gut by embedding the head and
anterior portion of the body in the intestinal
mucosa. Each adult worm sucks about 0,005 mI
of blood per day, causing also damage to the
mucosal surface, which results in protein and
other losses.
Question 13
Describe the life cycle.
Whip-worm life-cycle
Child ingests eggs
in soil
Develop into adult
worms and attach
to large bowel
mucosa
Larvae hatch in
terminal ileum
and caecum
Cont.
Answer 13
Parasite eggs are passed in the stools of Infected
individuals and mature within three weeks of
being deposited in soil. Eggs are ingested by the
child and larvae penetrate small intestinal villi.
After 3-10 days they move down to the caecum and
ascending colon where they mature into adult
worms. Each female passes 5000 eggs/day. In
contrast to ascaris, there Is no visceral invasion
in the case of trichuris.
Question 14
What are the clinical manifestations of trichuris?
Answer 14
Only heavy Infestations cause symptoms. There
may then be:
chronic diarrhoea
anaemia from blood loss and iron deficiency
Failure to thrive/marasmus
rectal prolapse (rare)
RARELY a child will develop congestive cardiac
failure because of anaemia and fluid retension
hypoproteinemia and oedema
Answer 14 continued
clubbing
blockage of lumen of appendix may lead to
appendicitis
Milder infestations may cause vague abdominal
complaints, such as colic and abdominal
distension. However, the symptoms may be due
to co-existing protozoa and other parasites (eg
giardia, ascaris).
Question 15
How Is the diagnosis made?
Answer 15
1. Stool microscopy
shows characteristic
"tea tray eggs”
2. Sigmoidoscopy
may enable
visualisation of worms
Question 16
How is whipworm treated?
Answer 16
Mebendazole - cure rate of 70% - 90%
- reduces egg output by 90 - 99%
OR
Albendazole
Treat the iron deficiency anaemia.
Question 17
What Is this worm?
Answer 17
HOOKWORM - Aj2cylost~ duodenale (variety found
in the Americas:Necator americanus)
These roundworms are widely distributed
throughout the tropics and subtropics. It is
estimated that more than 1 billion people are
infected world-wide. Most commonly infected are
children, agricultural workers and miners. In
northern Zululand, some locations have a
childhood infection prevalence of up to 70%.
However, Infection is virtually negligible In other
parts of Southern Africa.
Question 18
How large is the adult hookworm?
Answer 18
They are greyish-white, slightly curved and measure
5 - 13 mm in length. Teeth in their buccal cavity
enable their attachment to intestinal mucosa from where they suck their host's blood.
Blood loss is greater than with trichuris - 0,03 to
0,3ml/worm/day. The worm's mean life span Is 1 3 years, and they produce several thousand eggs
per day.
Question 19: Hookworm
lifecycle
Larvae
penetrate
Child's skin
Eggs excreted
in faeces
Child ingests
eggs,larvae
penetrate gut
wall
Mature females
pass eggs
Migrate through
lungs, up airways,
to reach small
bowel
Answer 19
The larvae live in the soil for 1-2 weeks, moult
twice and change into infective larvae capable of
penetrating the skin. They migrate up the veins
from the skin and are carried to the lungs. From
here, they follow the same migratory path as
ascaris, by breaking into the alveolar spaces,
migrating up the bronchial tree, being swallowed
and passed to the jejunum where they attach and
mature.
Cont ..
19 Continued
The child may thus become Infected via 3
mechanisms:
I. Larvae penetrating the intact skin - most
commonly
2) Drinking contaminated water
3) Pica - transferring eggs to the mouth via dust and
dirt.
The next slide shows a mature egg with the
embryo inside
19 continued
Mature egg with an
embryo inside
Question 20
what are the symptoms?
Answer 20
Once again the majority are asymptomatic.
Larval invasion through the skin may be
associated with an irritating dermatitis 'ground
itch'.
lung migration - bronchospasm
- pneumonitis
Small intestine epigastric pain and tenderness
thought to be due to worms
invading the mucosa.
- anaemia, hunger and pica,
depending on wormload and
dietary Iron Intake.
20 continued
• Heavy infestations
- diarrhoea (blood and mucus
- slow development of anaemia
(Hb can be below 5 g%) which
can lead to congestive heart
failure and even sudden death.
- hypoproteinemia and oedema.
The next slide shows numerous hookworms on
the bowel mucosa:
20 continued
Hookworms on the
bowel mucosa
Question 21
How is diagnosis made?
Answer 21
Microscopic examination of stool for ova.
Question 22
What is the treatment?
Answer 22
1) Evaluate Intensity of infection and severity of
anaemia. If Hb < 5 g%, need to be treated with
Iron first = elemental iron 2 mg/kg t.d.s.
2) Treat congestive failure.
3) Mebendazole by mouth
Question 23
What are the control measures?
Answer 23
This depends on sanitation and mass
chemotherapy. Prevented by wearing shoes and
protective clothing.
Question 24
What are threadworms?
Answer 24
Enterobius vermicularls. (The American literature
refers to Enterobius as the 'pinworm' and calls
Strongyloides stercozalis the 'threadworm').
Enterobius occurs world-wide and Infects
individuals of all ages and socio- economic
levels, but it is especially common In children. In
contrast to other roundworms, it prefers
temperate climates. Congested living conditions,
institutions, and Infected families predispose to
childhood infection. The infection is essentially
harmless and problem are more social than
medical.
Question 25
Describe the lifecycle.
Answer 25
The child ingests embryonated eggs, usually
carried on fingernails, clothing, bedding or
house-dust. Eggs hatch in stomach, larvae
migrate to caecal region where they mature into
adults. The egg-bearing adult females migrate by
night to perianal region, to deposit masses of
eggs and then disintegrate. Perianal itching from
the eggs Induces scratching, and hence the
eggs are transmitted to the mouth on the fingers.
Question 26
How would you recognise a threadworm If you
met one?
Answer 26
They are small white worms about 1 cm in length.
The eggs are characteristic, because after a 6
hour maturation period, a single coiled larvae can
be seen within each ovum. They may remain
viable for 20 days.
Question 27
What are the clinical features?
Answer 27
1. Nocturnal anal pruritis. The cause of this is
unknown, but may be related to the intensity
of the infestation, and/or an allergic reaction
to parasite.
2. Sleeplessness, because of the irritation.
3. Vulvovaginitis, and even urethritis may occur
in girls when migrating worms lay their eggs
in these sites.
4. Abdominal pain or appendicitis resulting from
threadworms are considered to be very rare.
Question 28
How is the diagnosis made?
Answer 28
Eggs are collected by
pressing adhesive
cellophane tape on
the perianal region
early in morning. This
is then stuck to a
glass slide which is
examined under a
microscope.
Question 29
How would you treat a child with threadworms?
Answer 29
Mebendazole or abendazole Regular bathing and
changing of underclothes Keeping fingernails
short Treat the whole family
Question 30
What is Strongyloides?
Answer 30
This is a small
roundworm with a life
cycle similar to
hookworm. It is
common In the tropics
and subtropics, but
can also occur in
temperate zones. The
adult worms live In the
crypts of glands in the
upper intestine.
30 Continued
The larvae enter the skin, and auto
infection is also common, larvae in the
faeces entering the skin in the perianal
region.
The active larva is seen in the previous
slide
Question 31
What are the symptoms?
Answer 31
In heavy Infections there are abdominal pain,
bloody diarrhoea, iron deficiency and debility.
Immune compromised individuals (e.g. HIV
infected) may succumb to overwhelming Infection
with strongyloides. There may be a recurrent
perianal dermatitis from autoinfection.
Question 32
What is the treatment?
Answer 32
Albendazole Is the treatment of choice.
Question 33
Name 2 roundworm parasites found in animals
which can cause symptoms in humans?
Answer 33
The dog roundworm toxocara canis (closely related
to ascaris) causes visceral larva migrans. In this
condition there are multiple granulomata in
various organs caused by migrating larva, which
cannot complete their life-cycle as they are In the
wrong host. The lungs, the liver and spleen, and
the back of the eye are most commonly affected.
The results may be protracted fever, failure to
thrive, wheezing, or loss of vision in one eye, with
appearances simulating a tumour.
Question 34
How would you make a diagnosis?
Answer 34
Ask if there has been a new puppy in the
household.
There is generally a very marked eosinophilia in
the peripheral blood.
Hyperglobulinaemia
Specific serological tests
Clearly, the ova cannot be found in the stool, as
in ascariasis.
Question 35
What is the treatment?
Answer 35
Most generally recommended is thiabendazole:
50ng/kg per day for 3-5 days, or 25 mg/kg for 1-4
weeks. The newer albendazole also shows
promise. Corticosteroids are helpful for ocular
lesions.
Regular and routine deworming of dogs is the
most important preventative measure.
Question 36
What worm causes
this rash?
Answer 36
The larvae of the dog hookworms, especially
Ankylostoma braziliense and A caninum after
penetrating the child's skin, are unable to enter
the blood or lymph vessels, and instead wander
about In the skin, causing intensely itchy wormlike tracks 'sand-worm' 'creeping eruption', or
'cutaneous larva migrans'. The most commonly
affected areas are the buttocks and feet.
Question 37
What Is the treatment?
Answer 37
The best cure rates are with thiabendazole
applied topically (crush a tablet in some vaseline
and apply 3 times a day). Do NOT use an ethyl
chloride spray: this Is painful and ineffective.
Summary of Treatment.
Worm
Treatment
Dosage
Ascaris
Piperazine or
Mebendazole or
Trichuris
Albendazole
Mebendazole or
Albendazole
120mg/kg, repeat after 1
week
100mgbd x3 days
400mg once
100mg bd x3 days
400mg once
Hookworm
Mebendazole or
Albendazole
100mg bd x3 days
400mg once
Treat iron deficiency
Mebendazole or
Albendazole
100mg bd x3 days
400mg once
Enterobius
Mebendazole or
Albendazole
100mg bd x3 days
400mg once
Toxocara
Thiabendazole or
Albendazole
50mg/kg/day x5
15mg/kg/day x5
Sandworm
Thiabendazole
Applied locally
Strongyloides
Further Reading
Taylor; Pillai & Kvalsig: SAMJ; 1995; 85:871
NELSON; Textbook of Paediatrics; p991 - 1007
COOVADIA & LOENING; Paediatrics a Child
Health; 1992; p212 - 217 JEFFREY; Atlas of
Medical Helminthology & Protozoology; 1991; p5
LAMBERT; Slide Atlas of Infectious Diseases;
Unit 14; p14.5 - 14.11
TAYLOR ET AL; Targeted chemotherapy for
parasitic Infestations in rural black preschool
children; SAMJ; 1995; 85(9) p870 874 3rd Year
Lecture Notes 6th Year Lecture Notes Anatomical
Pathology Specimens