Obstructive and restrictive respiratory diseases
advertisement

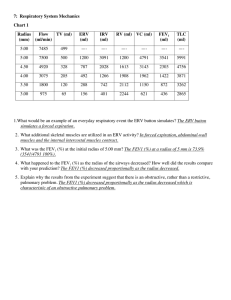
Obstructive and restrictive respiratory diseases Lung volumes • Total Lung Capacity (TLC) - the total volume of the lung, the volume of air contained in the lung at the end of maximal inspiration • Inspiratory Reserve Volume (IRV) - volume, which can be inspired beyond a restful inspiration • Tidal Volume (TV) – volume of a single breath, usually at rest • Functional Residual Capacity (FRC) - The amount of air left in the lungs after a tidal breath out, the amount of air that stays in the lungs during normal breathing • Vital Capacity (VC) – maximum volume which can be ventilated in a single breath • Inspiratory Capacity (IC) - the maximal volume that can be inspired following a normal expiration • Expiratory Reserve Volume (ERV) – volume, which can be expired beyond a restful expiration • Residual Volume (RV) – volume remaining in the lungs after a maximum expiration Volumes • Forced Vital Capacity (FVC) - the volume of air that can forcibly be blown out after full inspiration, measured in litres • Forced Expiratory Volume in 1 Second (FEV1) - the maximum volume of air that can forcibly blow out in the first second during the FVC manoeuvre, measured in liters • FEV1/FVC (FEV1%) - in healthy adults this should be approximately 75–80%. In obstructive diseases (asthma, COPD, chronic bronchitis, emphysema) FEV1 is decreased because of increased airway resistance to expiratory flow and the FVC may be increased (for instance by air trapping in emphysema). FEV1/FVC is decreased (<80%, often ~45%). In restrictive diseases (such as pulmonary fibrosis) the FEV1 and FVC are both reduced proportionally and the FEV1/FVC value may be normal or even increased as a result of decreased lung compliance Obstructive lung diseases • • • • airway obstruction restricted expiration FEV1, FEV1/FVC compliance, elasticity normal • Chronic bronchitis – Bronchiolitis • Asthma • Emphysema • Bronchiectasia • Cystic fibrosis Asthma COPD Condition Major changes Causes Chronic bronchitis Hyperplasia and hypersecretion of mucus glands Bronchiectasis Dilation and scarring Persistent severe of airways infections Cough, purulent sputum and fever Asthma Smooth muscle hyperplasia Excessive mucus Inflammation Immunologic or idiopathic Episodic wheezing cough and dyspnea Emphysema Airspace enlargement Tobacco smoking Genetic Dyspnea and wall destruction Tobacco smoking and air pollutants Symptoms Productive cough Restrictive lung diseases • • • • restricted lung expansion restricted inspiration + expiration FEV1, FVC, FEV1/FVC normal compliance, elasticity • Interstitial diseases – pneumonia • Fibrosis of lungs – asbestosis, silicosis • Restriction to breathing – pneumothorax, malformities, fracturae Signs • dyspnea • hypoxemia • cor pulmonale Flow volume curves Normal spirogram Spirogram in restriction Spirogram in obstruction Asthma • Chronic inflamatory disease of bronchi leading to spasmatic occlusion and hyperproduction of viscous mucus Causes • allergic – allergens – infection • non-allergic – neurogenic – psychogenic Asthma atack • acute exacerbation of asthma Signs and symptoms • dyspnea, wheezing, catching for air • cough – viscous sputum • cyanosis • tachycardia • chest pain Chronic bronchitis • chronic inflammation of bronchi Causes • smoking • air pollutions Signs and symptoms • expectorating cough (productive cough, produces sputum) • dyspnea, wheezing • chest pain • fever • fatigue and malaise Chronic bronchitis Smoking • impairs ciliary movement • inhibits function of alveoli macrophages • hypertrophy and hyperplasia of mucus-secreting gland • causes smooth muscle constriction Air pollutions • ozone • CO • SO2 Emphysema Abnormal, permanent enlargement and destruction of theair spaces distal to the terminal bronchioles withou obvious fibrosis, progressively lose elasticity and eventual rupture of alveoli •Panacinar (or panlobular) emphysema: The entire respiratory acinus, from respiratory bronchiole to alveoli, is expanded. Occurs more commonly in the lower lobes, especially basal segments, and anterior margins of the lungs.Typical for alpha-1-antitrypsin deficiency. •Centroacinar (or centrilobular) emphysema: The respiratory bronchiole (proximal and central part of the acinus) is expanded. The distal acinus or alveoli are unchanged. Occurs more commonly in the upper lobes. Typical for smokers. Emphysema Causes • Inherited – alpha 1-antitrypsin deficiency • Acquired – cigarette smoking – air pollution Signs and symptoms • Dyspnea upon exertion, wheezing, coughing • Pursed lips to maximize ventilation • Right heart failure • Hypoxia, respiratory acidosis Emphysema Alpha 1-antitrypsin deficiency (A1AD) • inflammatory enzymes (such as elastase) destroy the alveolar tissue • most A1AD patients do not develop clinically significant emphysema • smoking and severely decreased A1AT levels (10-15%) can cause emphysema at a young age Chronic obstructive pulmonary disease • combination of chronic brnchitis + emphysema + asthma Cause • Smoking • Occupational exposures – coal mining, gold mining, silicosis • Air pollution • Genetics – alpha 1-antitrypsin deficiency • Other risk factors – a tendency to sudden airway constriction in response to inhaled irritants (asthma) – repeated lung infections • COPD as an autoimmune disease – sustained inflammation mediated by autoantibodies and autoreactive T cells Chronic obstructive pulmonary disease Signs and symptoms • dyspnea, wheezing • mucous sputum • respiratory failure • cyanosis • cor pulmonale • peripheral oedema (RV failure) • tachypnea