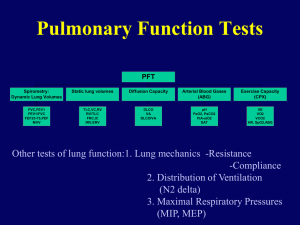
An Approach For
Spirometry and
DLCO Interpretation
Airway Function Tests
Spirometry
– Flow – Volume Loop (FVL)
Airflow obstruction
Mild on left
Severe on right
Variable extrathoracic
Large airway obstruction
Fixed
Quality check and consequences
Patient should exhale
suddenly and forced.
Patient should exhale
suddenly and forced
Patient should cough before
starting the measurement
www.spiro-webCard.de
Patient should inhale longer
and to the maximum
Different reasons;
more details in next slight
Patient should exhale as long
as possible; minimal 6 s
Criteria for acceptable
Minimum 3 trials
repeatability
Quality check of best 2 trials
ERS/ATS
FEV1 & FVC < 150 mL
FVC (<1L) < 100mL
FEV1 und FVC < 5%
PEF < 10%
Acceptable repeatability
D IVC = 3%
D FEV1 = 2%
Insufficient repeatability
D IVC = 15%
D FEV1 = 14%
FVC
Interpretation of % predicted:
–
–
–
–
80-120%
70-79%
50%-69%
<50%
Normal
Mild reduction
Moderate reduction
Severe reduction
FVC
FEV1
Interpretation of % predicted:
–
–
–
–
–
>70
60-69
50-59
35-49
<35
Mild
Moderate
Moderately severe obstruction
Severe
Very severe
FEV1
FVC
FEF25-75
Interpretation
– >60%
– 40-60%
– 20-40%
– <10%
of % predicted:
Normal
Mild obstruction
Moderate obstruction
Severe obstruction
Lung volumes
Dynamic
lung volumes
Static lung volumes
Residual Volume is
determined by one of 3
techniques.
Gas
Dilution Techniques
– Nitrogen washout
– Helium dilution
Whole
Body Plethysmography
Radiography
Volume-constant body plethysmograph
Functions of body box
1-Allows complete analysis of breathing
mechanics of the respiratory system→
Specific airway resistance(sRaw)
Intrathoracic gas volume
(FRCpleth)
Both →Airway resistance (Raw)
2-In combination with spirometry →
Absolute volumes →RV-TLC
Partial volumes → ERV-IRV
Lung capacities → VC-IC
Three types of measurments:
1-
Insp. and exp. flow rate during
the breathing cycle.
2-Air
volume changes inside the
cabinet
3
– Changes in air pressure at the
subject mouth
– 1+2 →Determine sRaw
Boyle’s Law
If temperature is constant:
Pressure1 x Volume1 = Pressure2 x
Volume2
P1 and V1 are the absolute
pressure and volume before the
manoeuvre while P2 and V2 are
the pressure and volume after
the manoeuvre.
Body - Measurement
Calculated parameters
RV
= FRCplet – ERV
TLC
= VC + RV
Important resistance
parameters
sRtot → the points of max. volume shift on
the loop.
→high sensitivity down to the
peripheral airways.
sReff → derived from the area covered by
the work of breathing.
→high sensitivity within the
central airways.
Rtot= sRtot/(FRCplet +VT/2)
Reff= sReff/(FRCplet +VT/2)
Interpretation
Shape
of the graphs
resistance Raw =0.6-2.8 cm/L/sec
sRaw =0.190.667 cm/L/sec
pred./best < 80%
Lung volumes FRC and RV65135%
TLC 80-120%
RV/TLC%
20-35%
VC
80-120%
Lung volumes
Volume
Restrictive
TLC
↓
N
↑
VC
↓
↓
N
FRC
↓
↑
↑
RV
↓
↑
↑
RV/TLC%
N
↑
↑
Air trapping Hyperinflati
on
What about lung volumes and
obstructive and restrictive disease?
COPD
Asthma
Soll Ist
Soll
Ist
VOR
Ist
NACH
Emphysema+asthma
Ist
Soll
Soll
Ist
VOR
Ist
NACH
Restriction
The maximal voluntary ventilation (MVV) is
not generally included in the set of lung function
parameters necessary for diagnosis or follow-up
of the pulmonary abnormalities because of its
good correlation with FEV1 .
However, it may be of some help in clinical
practice. For example, a disproportionate
decrease in MVV relative to FEV1 has been
reported in neuromuscular disorders and UAO .
In addition, it is also used in estimating breathing
reserve during maximal exercise.
Obstructive abnormalities
An obstructive ventilatory defect is a
disproportionate reduction of maximal
airflow from the lung in relation to the
maximal volume (i.e. VC) that can be
displaced from the lung .
It implies airway narrowing during
exhalation and is defined by a reduced
FEV1/VC ratio below the predicted value.
This slowing of expiratory flow is most
obviously reflected in a concave shape on
the flow–volume curve.
Quantitatively, it is reflected in a
proportionally greater reduction in the
instantaneous flow measured after 75% of
the FVC has been exhaled (FEF75%) or in
mean expiratory flow between 25% and
75% of FVC than in FEV1.
measurement of lung volumes is not
mandatory to identify an obstructive defect.
It may, however, help to disclose underlying
disease and its functional consequences.
For example, an increase in TLC, RV or the
RV/TLC ratio above the upper limits of natural
variability may suggest the presence of
emphysema, bronchial asthma or other
obstructive diseases , as well as the degree of
lung hyperinflation.
Restrictive abnormalities
restrictive ventilatory defect is
characterized by a reduction in TLC below
.
the predicted value, and a normal
FEV1/VC.
The presence of a restrictive ventilatory
defect may be suspected when VC is
reduced, the FEV1/VC is increased (>85–
90%) and the flow–volume curve shows a
convex pattern.
.
low TLC from a single-breath test
(such as VA from the DL,CO test)
should not be interpreted as
demonstrating restriction, since such
measurements systematically
underestimate TLC .
The degree of underestimation increases
as airflow obstruction worsens. In the
presence of severe airflow obstruction,
TLC can be underestimated by as much as
3 L.
Mixed abnormalities
A
mixed ventilatory defect is
characterised by the coexistence of
obstruction and restriction.
Since VC may be equally reduced in
both obstruction and restriction, the
presence of a restrictive component
in an obstructed patient cannot be
inferred from simple measurements
of FEV1 and VC.
If FEV1/VC is low and the measured VC is below
its lower limits of normal (LLN), and there is no
measurement of TLC by body plethysmography,
one can state that the VC was also reduced,
probably due to hyperinflation, but that a
superimposed restriction of lung volumes cannot
be ruled out .
Conversely, when FEV1/VC is low and VC is
normal, a superimposed restriction of lung
volumes can be ruled out .
 0
0