The Endocrine System
Pathophysiology
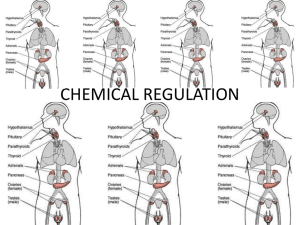
A & P Review of Endocrine System
Mechanism of Hormone Action
•
•
•
•
•
Hormones play an important function in regulation & control of body functions &
metabolism
Hormones exert control that is slower acting but of longer duration than nerve
impulses
Hormones secreted by endocrine glands go to a target organ
How do specific hormones know where to go?
– Receptors in the cell are specific for certain hormones
» Thus get “lock & key effect”
2 types of hormones
• Protein derivative hormones (from amino acids or polypeptides)
» water soluble, thus need plasma membrane receptor
» then need second messenger for hormone to exert its action
» this action occurs in the cytoplasm
• Lipid derivative hormones (primarily steroids)
» Fat soluble, thus pass right through the cell membrane
» bind with receptor in the nucleus
» this complex triggers DNA to make a specific protein
Regulation of Hormonal Secretion
• The control of hormonal secretion is “homeostatic feedback”
• Another name for this is: “negative feedback”
• Remember negative feedback reverses the direction of change back to
physiologic normal
» if hormone level too high----- the gland is shut down
» if hormone level too low ------the gland is stimulated
• Positive feedback augments the direction of change
» if hormone level high ----- the gland is stimulated
» if hormone level too low---- the gland is shut down, even further
• Most endocrine diseases are centered around:
– TOO MUCH = hypersecretion--- from glandular hyperplasia or a
functional tumor (adenoma or carcinoma)
– TOO LITTLE = hyposecretion – from glandular atrophy or a
destructive carcinoma
Prostaglandins
• Written as PG; called “tissue hormones”
– they are substances produced locally by specific tissues
– they travel only short distances & thus have a localized effect
– 2 types: Inflammatory (bad) & non-inflammatory (housekeeping or good)
• Prostaglandins & leukotrienes = usually enhance inflammation
• Prostacyclins & thromboxanes = work in opposition to platelet aggregation
– they are lipids called eicosanoids
• The major eicosanoid fatty acid precursor = arachidonic acid
– This is a essential fatty acid; thus from diet
» Omega 3 fatty acids produce non-inflammatory PG’s
» Omega 6 fatty acids produce inflammatory PG’s
– their synthesis begins when a cell membrane is disrupted e.g. injury
» the disrupted cell membrane releases certain lipids into the
cytoplasm that begins PG synthesis
•
•
Mech of action of PG’s
• COX = cyclooxygenase = enzyme that synthesizes prostaglandins
• 2 forms: COX-I & COX-II
• COX-I = results in products (prostaglandins) that act on stomach,
platelets, & vascular endothelium (prostacyclins)
• These prostaglandins are involved in homeostatic activities
• Also called “housekeeping” activities
• These include:
1. Maintaining GI mucosal barrier
2. Maintaining platelet function
(checks & balances via prostacyclin & thromboxane)
3. Maintaining vascular homeostasis
• COX-II = results in products(prostaglandins) that are
inflammatory chemical mediators
• Get organ smooth muscle contraction (constrict bronchi)
• Vasodilation
• Pain
Anti- prostaglandins (NSAID’s)
• Non-selective NSAID’s inhibit COX I & COX II
• Selective COX II agents exert their actions primarily on the inflammatory process
( they inhibit it)
Pituitary Gland
• 2 glands
– Anterior pituitary
• Adenohypophysis
– Posterior pituitary
• Neurohypophysis
• Extension of
hypothalamus
Diseases of the Pituitary
• TSH
– hypersecretion = hyperthyroidism
– hyposecretion = hypothyroisism
• ACTH
– hyposecretion = Addison’s disease
– hypersecretion = Cushing’s disease
• FSH
– hyposecretion
• M = poor sperm production
• F = low estrogen, amenorrhea
– hypersecretion
• F = menopause
• LH
– hyposecretion
• F = no ovulation
• M = low testosterone
• MSH
– hypersecretion = excess pigment
• GH
– hypersecretion
• during growth = giantism
• after growth = acromegaly
– hyposecretion = dwarfism
• PRL
– hypersecretion = galactorrhea,
infertility
– hyposecretion = poor milk
production
• ADH
– Hypersecretion = SIADH
• Syndrome of inappropriate ADH
secretion
– hyposecretion = diabetes insipidus
Diseases of the Pituitary
• General facts
– Main cause of pituitary diseases = benign adenomas
• Age: 30 – 50 years old
– Symptoms fall into 2 main categories:
• Pressure symptoms from glandular enlargement
» Headache, seizures, drowsiness, visual defects
• Hormonal effects
» Usually stimulatory if functional tumor
» May be inhibitory (non-functional with pressure necrosis)
– Most common hormonally active adenomas = prolactinoma
Specific Pituitary Diseases
Giantism
– If congenital may be accompanied by mental retardation &/or sexual retardation
– If occurs after puberty ---- called acromegaly
• Get enlarged hands & feet, protruding mandible
– Etiology usually pituitary adenoma
Dwarfism
– If congenital get mental retardation(+/-) & no secondary sexual characteristics
– Tx = GH
Prolactinoma
– Most common pituitary functional tumor
– Get high prolactin levels
• In women get galactorrhea, amenorrhea, infertility
• In men get impotency, oligospermia, decrease libido
Diabetes Insipidus
– Symptoms = polyuria & polydipsia
– Get large amounts of dilute urine & dehydration
– Etiol:
• head injury or surgery = temporary condition
• Nephrogenic tubular insensitivity to ADH = permanent condition
– Tx = replacement therapy with ADH
SIADH
– Get too much ADH secretion & get retention of fluid
– Etiol :
– Some cancers especially oat cell lung cancer (very common cancer)
– Post op (temporary, only last 1 week)
– Stress
– Psychiatric diseases
– Pathophysiology = hypoosolarity & hyponatremia
– Symptoms related to low serum sodium
– First = fatigue & weakness
– Then G-I sx
– Then twitchings, convulsions, & coma
Hypothalmus
• Three things it does relating to the endocrine system
– (1) it makes the posterior pituitary hormones
» oxytocin (OT)
» antidiuretic hormone (ADH)
* nb: diabetes insipidus & SIADH
– (2) it controls the anterior pituitary by means of hormones it makes
– This physiology used in pharmacology
» Releasing Hormones
* exp = GnRH (gonadotropin releasing hormone)
» Inhibiting Hormones
– (3) It controls sympathetic output of adrenal medulla
see next slide
Thyroid Gland
• 3 hormones
• Thyroxine (T4) = more abundant than T3, but less potent
• Triiodothyronine (T3) = more potent than T4
• Calcitonin
– Functions:
• Thyroid hormones (T4 & T3) function = increase metabolic rate
• Calcitonin
– lowers serum calcium by preventing the bones from giving it up
– works in harmony with the parathyroid & parathormone
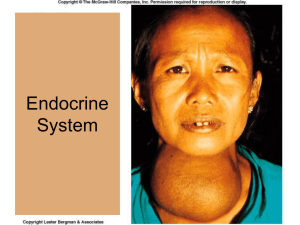
• Disease states
Goiter – may be euthyroid, hyper or hypo
hyperthyoidism
• Grave’s disease = one specific type;autoimmune etiol;
get exophthalmos
hypothyroidism
• cretinism = congenital type
• myxedema = adult type;get edema of face & tongue
• Hashimoto’s disease = autoimmune; chronic inflam.
produces fibrosis of thyroid
Thyroid cancer
Key cause = radiation exposure
Goiter
• By definition just means thyroid enlargement
• Pathophysiology = excess TSH
• If have goiter, patient may be
» Normothyroid
» Hypothroid
» Hyperthyroid
• 3 clinical types
• Endemic goiter --- from lack of iodine in diet (hypothyroid)
» See next slide
• From goitrogens --- from drugs (e.g. lithium) & foods (e.g. cabbage)
– These prevent T3 & T4 production
• Toxic goiter --- hyperthyoidism
– Note: if goiter present & patient hyperthyroid but not toxic ---think of Grave’s disease
Endemic goiter; hypothyroidism
Hyperthyroidism
•
•
•
•
•
2 types: with exophthalmos & without exopthalmos
Graves disease
• Autoimmune
• Most common form of hyperthyroidism
• Get goiter
Symptoms = “motor running fast”
– Tachycardia, systolic hypertension, palpitations, insomnia,
– heat produces discomfort
– Exophthalmos (+/-)
Complication = thyrotoxicosis or thyroid storm
Treatment
• Radioactive iodine
• Surgery
• Antithyroid drugs
Hypothyroidism
• Commonest problem of thyroid
• 3 forms
• Hashimoto’s thyroiditis---- autoimmune
• Myxedema --- adult severe hypothyroidism
– Myxedema = nonpitting edema of puffy face & thick tongue
– In early mild form --- symptoms subtle; hard to diagnose
– Muscle weakness (hung-up reflex)
– Mental apathy
– Dry skin
– Likes heat (always cold)
• Cretinism ---- congenital
– short stature, thick tongue, protruding abdomen, mental retardation
– Lack of hair (axillary)
Parathyroid Glands
•
•
Normally 4 glands located on posterior surface of thyroid
• may have up to 8 glands
produces hormone: Parathormone (PTH)
– it increases calcium in blood by breaking down bone to release calcium
– it works in conjunction & opposite calcitonin
– Effects of parathormone:
– 3 key effects: 2 on bone & 1 on kidneys
» 1. Acutely --- breaks bone down & increases serum Ca++
» 2. Chronically --- get bone remodeling; i.e. bone is broken down &
reformed
» 3. In kidneys resorbs Ca++ & secretes phosphorus
– Tissue effects of calcium:
• Skeletal muscle ------- no effect
• Cardiac muscle ------- low weakens contraction; high strengthens contraction
(arrhythmias)
• Nerve conduction ----- low increases excitability (get twitching, spasm, tetany)
high decreases excitability
– Hyperparathyroidism = hypersecretion = hypercalcemia
• symptoms = SOUP, cardiac irritibility, osteoporosis, skeletal muscle
weakness due to decrease excitability of nerves
• Primary hyperparathyroidism
– Etiology ---- adenoma
• Secondary Hyperparathyroidism more common
– Etiology = decrease serum calcium secondary to:
» Renal disease
• Hypoparathyroidism = hyposecretion = hypocalcemia
• symptoms =
– hyperexcitible neuromuscular system & get twitching, spasms, &
tetany
– Skeletal muscle contraction power = same; no change
– Cardiac muscle = weak contraction
• Etiol
– Metastatic cancer --- raises calcium in blood & thus shuts off gland
– Immobility – causes bone to release calcium
Pancreas
•
Pancreas is both endocrine & exocrine gland
– exocrine = digestive enzymes secreted via duct into duodenum
– endocrine located in Islets of Langerhans
• Cells of the islets
– alpha cells produce glucagon
» it raises blood sugar by increasing liver
glycogenolysis
– beta cells produce insulin & amylin
» Insulin lowers blood sugar by escorting glucose into
the cells
» Amylin contributes to postprandial glucose control
* slows gastric emptying
* regulates appetite centrally
* see comment on “good health” --- next slide
• Insulin
– Anabolic hormone (a type of growth factor)
• Promotes synthesis of proteins, nucleic acids, & fats
• This occurs in liver, muscle, & adipose tissue
• Permits primarily glucose & ,also, amino acids into the cytosol
– Certain cells do not need insulin to get their glucose supply
» Brain
» RBC’s
» G-I tract epithelial cells can absorb glucose from diet
– Theory of good health, longevity, & prevention of “aging” diseases
• Good health = slow rises & falls of insulin production
• Bad health = peaks & valleys production of insulin
• “Glycemic index” & food
Diabetes Mellitus
– Def: a disease that involves an “insulin deficit”
– Get hyperglycemia
– Get lack of available glucose in cells for mitochondria to make ATP
– Thus, mitochondria use fats to generate ATP
– Side effect = ketone body formation
– Pathophysiology (with associated symptoms/signs of the disease)
– Hyperglycemia
– Glucosuria
– Polyuria
– Polydipsia
– Polyphagia
-- & then—
– Fat catabolism
2 types
(90% = type II &
10% = type I)
• Insulin Dependent Diabetes Mellitus(IDDM) = Type I
– autoimmune; get decreased production of insulin
• Non Insulin Dependent Diabetes Mellitus(NIDDM) = Type II
– get cellular insensitivity to insulin
– Current epidemic in USA ; incidence --- 10% of adults
– Major risk factor = obesity
– Alzheimer’s disease & insulin cellular insensitivity
•
•
Etiology = autoimmune process; ? triggered by an infection early in life
Complications ---- divided into acute & chronic
– Acute complications
– Diabetic Coma ---- lethargy, dry (dehydrated)
– Insulin Shock ---- anxiety, sweating
– Chronic complications
– Vascular complications – get macro & microangiopathy
» Macroangiography
* MI’s; CVA’s, peripheral vascular disease
» Microangiography
* Kidneys ---- ruins glomerular capillary basement membrane
*Eyes ------ get diabetic retinopathy which leads to blindness
Adrenal Cortex
•
Has 3 distinct layers or zones
– from outside towards middle:
• Zona Glomerulosa
– secretes mineralcorticoids (Aldosterone)
» Retain sodium (water follows sodium)
» Usually gets rid of potassium &
hydrogen
• Zona Fasiculata
– secretes glucocorticoids (Cortisol)
» Secreted in response to stress
» Causes gluconeogenesis &
hyperglycemia
» Causes protein catabolism
* thus, delays healing
» Is anti-inflammatory
» Maintains BP by sensitizing vessels to
ANS
• Zona Reticularis
» secretes sex hormones (steroids)
Diseases of the Adrenal Cortex
– even though there are 3 different classes of hormones, most diseases affect primarily
the glucocorticoids
– Hypersecretion
– Commonest problem = involves glucocorticoids; but some diseases may
have a combination of components
– Of glucocorticoids = Cushing disease
– Commonest etiology = pituitary adenoma secreting ACTH
– Other etiol:
– ectopic ACTH secreting tumor (oat cell lung cancer, etc)
*called paraneoplastic syndrome
– Adrenal adenoma
– Taking “steroids” (exogenous)
– Of mineralcorticoids = hyperaldosteronism
– Commonest etiol = adrenal adenoma
– Note that 5-10% of people with hypertension have them
– Of sex steroids = feminization or virilization
– Clinical picture depends on sex
– Commonest etiol = adenoma & associated with Cushing disease
•
Cushing Disease (MOODIAH)
– Moon face
– Obesity & edema from salt
&
water
retention
– Osteoporosis
– Diabetes
– Infections
– Atherosclerosis
– Hypertension
•
Etiol
– Pituitary adenoma
– Adrenal adenoma
– Ectopic paraneoplastic
syndrome
– Iatrogenic
• Only cause that
produces adrenal
atrophy & resultant
poor response to stress
see next slide
Etiol
– Pituitary adenoma
– Adrenal adenoma
– Ectopic
paraneoplastic
syndrome
– Iatrogenic
• Only cause that
produces
adrenal atrophy
& resultant poor
response to
stress
– Hyposecretion
– Usually affects both glucocorticoids & mineralocorticoids
• Addison Disease = primary adrenal insufficiency
• Commonest etiol = autoimmune destruction of adrenal cortex
• Get increased levels of ACTH
• In secondary hypocortisolism get low levels of ACTH
• Commonest etiol = exogenous glucocorticoids
Diagnostic clinical difference:
• Increase ACTH & Addison disease = skin pigmentation (bronze color)
• Decrease ACTH & Addison disease = no skin pigmentation
• Clinical features
– get hypotension, fatigue, weakness, & weight loss
* severe hypotension = shock = life threatening
– get dehydration & hyperkalemia* (from lack of aldosterone)
– get bronze skin color & pigmentation ( if increase of ACTH)
– Vitiligo from autoimmune destruction of melanocytes
Adrenal Medulla
•
Works in conjunction with sympathetic nervous system
• Involved in the “stress response”
• Makes catecholamines
• Key ones are norepinephrine (20%) &
epinephrine (80%)
• Epinephrine is 10 times more potent in
producing direct metabolic effects
* note that norepinephrine is more
potent as neurotransmitter
•
Diseases of Adrenal Medulla
– Pheochromocytoma
•
•
•
•
•
Benign tumor of adrenal medulla
Cells of medulla called pheochromocytes
Greek = dusky color
Secretes epinephrine
Get hypertension
Stress Response
•
•
Def: A systemic generalized response to a change (stressor) either internal or
external
– Stressors:
– Physical
– Psychological
– Real
– Imagined
– Anticipated
Stressors are normal component of life
• Can be positive ---- stimulate growth & development
• Can be negative ---- if severe and/or not properly dealt with
• Note possible complications
– Hypertension
• CHF
• Kidney failure
– CNS
• Stroke via vasospasm
• Depression
– Fatigue
• Insomnia
• Tension headache
– Infections ---- see picture
– Digestive
• Stress ulcers
• GERD
• N&V; diarrhea
• IBS
– Diabetes mellitus