Gastrointestinal Disorders with
Pregnancy
Amr Nadim, MD
Ass. Prof. of Obstetrics and Gynecology
Ain Shams faculty of Medicine
Topics to be covered...
• Hepatic Disorders
– Intrahepatic Cholestasis
– Chronic Liver Diseases
– Viral Hepatitis
• Hepatitis A
• Hepatitis B
• Hepatitis C and others
Topics to be covered...
• Gastrointestinal Diseases
– Gastroenteritis
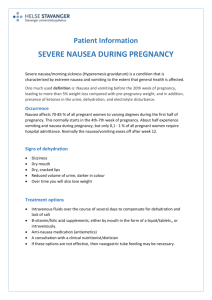
– Nausea and Emesis gravidarumHyperemesis gavidarum
– Gastroesophageal Reflux
– Peptic Ulcer
– Inflammatory Bowel Disease
Topics to be covered...
• Acute events
–Acute Appendicitis
–Acute Pancreatitis
–Acute Cholecystitis
Guidelines for Managing
Gastrointestinal Problems with Pregnancy
• Many are due to physiologic changes and are self limiting
• most of the problems could be managed by dietary
measures and reassurance.
• The decision to continue or to modify treatment for
a pre-existing condition should take into account the
benefit/risk ratio for mother and fetus
• A decision to treat in the first trimester should be
considered exceptional
Dietary habits in pregnancy
• Dietary craving:
– Towards peculiar tastes
– Pica: e.g geophagia but also to chalk, clay, ice
• Dietary aversions
– towards meat, fish, fatty food, etc….
• The occurrence of such food habit bears
nothing in common with nausea and
vomiting.
Disorders of the Oral Cavity
• Aphthous stomatitis:
– Vitamin B12 or folic acid deficiency
– May herald onset of GIT, collagen disorders or
blood diseases
– Treatment is symptomatic+topical steroids and
local anesthetics and that of the cause
• Hyperplastic gingivitis:
– Related to elevated hCG and sex hormones.
• Dental caries (1.5-2 times non pregnant):
– Increased acidophilic organisms under E+P
predominance
– Calcium deficiency is no more incriminated
Gastro-esophageal Disorders
Reflux
• Dyspepsia and heartburn are distressing symptoms
that occur in 70% of pregnant women starting from
the first trimester.
• In pregnancy there is drop of the “Barrier Pressure” :
[LOSP] - [Intragastric Pressure]
• Lowering of LOSP is due to the effect of E+P
• Heartburn is more severe after meals and is
aggravated in the recumbent position
Reflux
• General measures:
– Elevation of the head of the bed, small meals,
reduced fatty and spicy diet, avoidance of
smoking, caffeine and chocolate, refraining
from meals or liquids other than water within
3 hours from going to bed.
– OTC antacids:
• Avoid Na bicarbonate and particulate antacids
• 10-15 ml after meals and at bed time
–
–
–
–
Sucralfate 1g. Tds
Cimetidine 400 mg after the evening meal
Ranitidine- Famotidine
Domperidone (Motilium) may raise the LOSP
Emesis Gravidarum
Morning sickness: does not influence health
• Unknown etiology.
– Elevated levels of Gonadotropins and progesterone
– Elevated level of T4: occult thyrotoxicosis (GTT or else)
– Beta-endorhins secreted by the placenta and binding to
opioid receptors at the vomiting center
– bla bla bla!!!
• Is encountered in 50-85% of pregnancies. Most
frequently 6-8 weeks but in 20% may continue into
the second and third trimester.
Hyperemesis Gravidarum
Vomiting occurring before the 20th week and
requiring admission to the hospital
• Affects 0.5 to 10 per 1000 pregnancies.
• Peak incidence between 8th and 12th weeks.
• Multifactorial etiology: Hormonal, neurological,
psychological, metabolic and toxic factors…
• Beware of molar pregnancy and Hyperthyroidism.
• Laboratory data:
– Ketonuria, increasaed urine sp. Gravity, increased Ht.
– Hyponatremia, hypokalemia, metabolic alkalosis
– Alteration of Kidney and liver function tests.
Treatment
Should be tailored to suit individual cases.
• General measures:
–
–
–
–
Small, frequent meals.
Avoiding spicy and greasy diet.
Vitamins (including thiamine supplementation).
Nutritional consultation
• Initial therapy : oral therapy with oral or rectal
antiemetics.
• Hospitalization:
– Intractable emesis
– Hypovolemia and/or electrolyte imbalance.
– Laboratory anomalies.
Antiemetics
The FDA has approved no drug for treatment
of nausea and vomiting during pregnancy.
•
•
•
•
•
•
•
•
Pyridoxine(vitamin B6), 25mg tds
Phospharylated carbohydrate solution.
Doxylamine
Metoclopropmide (Primpran-Plasil)
Promethazine (Phenargan)
Chlorpromethazine
Ondasterone (Zofran): 4-8 mg tds
Methylpednisolone
Peptic Ulcer Disease
• Is of rare occurrence during pregnancy
• Some are reporting improvement of their
symptoms.
• Dietary recommendations
• Avoidance of NSAIDs
• Antacids and H2 receptor antagonists
• Serious complications are rare …However
if occurring they should be managed as the
non pregnant patient
Inflammatory Bowel Disease
Ulcerative Colitis - Crohn’s Disease
• Disease of young adults:
– UC: 15-30 years and CD: 20-35 years
– The fertility rate is unaffected in UC but reduced in CD
because of pelvic adhesions resulting from the
inflammatory process.
• Medical Management:
– Sulfazaline and Corticosteroids are safe
– Folate supplementation is a must
– The use of 6-mercaptopurine or azathiopine or
ciprofloxacine should be reserved to individual cases
IBD...
• Surgical Intervention:
– As for non pregnant ladies
• Effect on the outcome of pregnancy:
– There is increased fetal loss if:
• Manifest for the first time during pregnancy
• Colonic rather than small bowel disease.
• Uncontrolled and requires surgery
• How to deliver?
– Vaginal delivery unless perineal scarring
– Active perineal disease may render episiotomy healing
difficult
– Difficult intraperitoneal adhesions are expected in CS
Gastroenteritis
Viral , Bacterial or Parasitic
• Nausea, vomiting, cramping ands diarrhea with
headaches , myalgia and low grade fever.
• Symptoms last for 48 hrs.
• Treatment is supportive:
– Keep patients hydrated with adequate electrolyte
balance and place the bowel at rest.
– Bowel rest.
• Intrahepatic Cholestasis
• Most common disorder unique to pregnancy of
Variable incidence
• Increased risk of prematurity and IUFD
• Recurrent in 70% of the cases
– C/O:
•
•
•
•
Pruritis
Jaundice in 50% of cases
No Fever, Emesis, nor nausea
D.D. Viral Hepatitis, Gall bladder Disease.
Laboratory Investigations
–
Alk. Phosphatase +++
– Moderate
Serum Transferases.
– Bilirubin (Direct , rarely > 5 mg/dl
– Bile acids up to 10 folds.
• Diagnostic criteria: Pruritis + Increased
bile acids and salts
– Management
• Cholestyramine: 8-6 g /day (3-4 divided doses)
– Weekly Check PT; if prolonged give vit K(10 mg/day).
• Diphenhydramine
• Dexamethazone
• Phenobarbitone
– Tests for Fetal well being
– Terminate pregnancy when maturity is achieved
– Usually the condition subsides 2 days after
delivery
– Be cautious for postpartum use of COCs
Hepatitis B Virus
Parenteral exposure - STD - Vertical transmission
• Maternal Infection:
– HBV prodrome of arthralgia, myalgia, ±jaundice,
fever , nausea & vomiting
• Fetal infection; HBeAg carries a risk of 85 to
90% risk of chronic HBV and associated
sequelae.
• Morbidity and mortality:
– No worsening of the disease with pregnancy
– No CFM, IUFD, abortions or IUGR
Hepatitis B Virus
Hepatitis Markers
–
–
–
–
HBsAg: denotes carrier or infective status
HBeAg: High infectivity
Anti-HBcAg: partial convalescence.
Anti-HBsAg: immunity or recovery
• The risk of fetal transmission is highest in
HBeAg +ve mothers at the time of delivery
Hepatitis B Virus
Management
• The US CDC recommend universal screening of
pregnant women for HBV.
• HBIG interrupt vertical transmission in 90% of
cases:
– 5ml of HBIG administered as soon as exposure is
suspected.
– 0.5 ml of HBIG given to the newborn in 12 hrs from
delivery to be followed by the standard 3 doses of the
vaccine.
• Recombinant Hepatitis B Vaccination...
Hepatitis C
• Persistent disease is common.
• In utero transmission: 50% higher than HBV.
– To date there is no teratogenic Syndromes.
– There is however a risk for acute hepatitis or chronic
carrier state.
• Antibody to HCV - PCR for HCV-RNA
• Prevention of vertical transmission by HCIG is
equivocal.
• Exposed newborns; 0.5ml HCIG followed by
another dose 4 weeks later.
Chronic Liver Disease
• Chronic active hepatitis:
– Responds to immunosuppression with corticosteroids.
– Increased risk of stillbirths, ,prematurity and PE.
• Liver cirrhosis:
– Infertility is common.
– High perinatal loss and poor maternal outcome.
• Budd-Chiari Syndrome:
– May occur due to the hypercoagulable state of
pregnancy.
– Abdominal pain + Hepatomegaly & ascitis of abrupt
onset.
Acute Appendicitis
The most common surgical complication in
pregnancy
• A high suspicion index is needed…the classical
signs are often absent.
• Patients present with anorexia, nausea, vomiting,
fever, abdominal pain(site depending on the GA).
• DD:
–
–
–
–
–
Ectopic pregnancy
Pyelonephritis (Most common misdiagnosis)
Acute Cholecystitis
PID
Adnexal Torsion
Appendicitis...
• Therapy:
– Laparoscopy
– Laparotomy: There acceptable negative laparotomy rate
is 20-35%.
– Antibiotics
• Complications include: preterm labor, abortion. If
the delay is more than 24 hours the maternal and
fetal morbidity is increased
Mortality may approach 5% in case of surgical delay
Acute Cholecystitis
Second most common surgical complication
of pregnancy.
• 3.5% of all pregnant women have gall stones
• C/O:
– Abrupt onset of right upper quadrant pain, nausea, vomiting ,
anorexia, intolerance to fatty food
• Investigations:
– U/S
– CBC, serum lipases and amylases
• Treatment:
– Conservative
– ERCP
– Surgical
Acute pancreatitis
1 per 1000 to 1 per 3800 pregnancies
• Gall stones are the most common predisposing
factor.
• C/O:
– Midepigastric pain or left upper quadrant pain radiating
to the back
– Nausea, vomiting, ileus and low grade fever.
• Elevated Amylases and lipases are the Keyfindings
• Treatment is essentially conservative
– Cholecystectomy after the first trimester
– ERCP

![Questionnaire used in the study Demographics GENDER: M [ ] F](http://s3.studylib.net/store/data/006712173_1-21c851410b04058d524e1b79e54e32b0-300x300.png)