CCO`s
advertisement

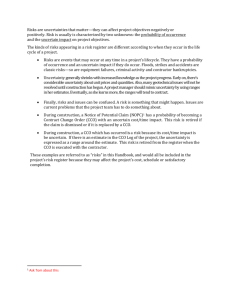
Oregon CCO’s – Passing Fad or A Model for the Future Changing How we Provide Care David Schlactus, CEO, Hope Orthopedics David Schlactus - None CCO’s v. ACO’s How they Came About Why CCO’s A Driving Force for Change? Preparing for CCO’s CCO’s in Portland v. other parts of Oregon A Passing Fad or the Future? “The definition of insanity is doing the same thing over and over again and expecting a different outcome” - Albert Einstein “Americans can always be counted on to do the right thing….after they have exhausted all other possibilities.” - Winston Churchill “In the absence of a compelling reason to change, people don’t” - Phillip Kotter, Leading Change Healthcare on it’s current course is unsustainable as a percent of the GDP 10,000 baby boomers turn 65 EVERY day More than 50 million Americans are uninsured In short: More people are without healthcare The cost curve has not yet been bent Access to healthcare is rapidly decreasing due to flatline reimbursement from Medicare & Medicaid Conceived by Don Berwick, MD, former head of CMS: Improve Access Decrease Costs Improve outcomes / patient experience But seriously - you can’t really do all three right? Well – maybe we can. Hello ACO’s – the new Capitation, albeit, “risk adjusted capitation” All money for the hospital and physician component are put in a basket and the participants fight over who gets how much. “Quality” must be demonstrated 65 demonstration projects in the US Coordinated Care Organization ◦ Includes all revenue for: Hospitals Physicians Behavioral / Mental Health Dental Care ◦ This is NOT a theoretical exercise – they became effective August 1, 2012 ◦ (Mental Health and Dental $$ to be added in 2013 or 2014) Plan to have 60% of ALL Medicaid / OHP patients enrolled by January 1, 2013 Plan to add PEBB and OEBB in 2014 Plan to add Healthcare Exchange patients in 2014 By 2014 – could be as many as 25% of ALL Oregonians in a CCO As of September 15, 2012 13 CCO’s statewide 75% of all OHP patients enrolled Over 500,000 Oregonians! Fixed budget limits upside cost to state Why this is BAD math? ◦ Medicare ◦ OHP ◦ Commercial $36 $28 – 30 $60 - $72 CF CF CF ◦ PEBB and OEBB = 15% of our volume ◦ Once in the CCO – the CCO will control these funds – ah, sorry but mental health and dental are underfunded so we need some of this money No problem – we just won’t participate Nope – SB 158 allows a CCO to MANDATE participation of providers if they provide critically needed services Arbitration for reimbursement rates Who can afford to drop out if it includes roughly 15% of your best paying commercial business? Oh- by the way – did we tell you that OHP rates are slated to go down by 10% on January 1, 2013? What’s a group to do? Change how care is delivered! The goal of Hope Orthopedics is to lower the cost of care (per unit) by 20%. You can not do this by cutting staff ◦ ◦ ◦ ◦ ◦ Meaningful use E-Rx PQRI QRUR Etc….. We have to redefine how care is provided Two groups working on this: ◦ Physicians and PA’s at Hope Orthopedics ◦ Clinic Administrators in Salem 17 physicians 10 PA’s 17 Therapists 6 ATC’s at 6 local HS = 42 providers 2 Clinics + 2 Satellites Staff spread between 4 buildings Buying 2 more buildings MRI, Brace Shop, Therapy, DEXA, ASC, ultrasound coming Don’t just think outside the box – break the box We forced ourselves to think different by creating wild and crazy scenario’s Some of our scenarios included: ◦ MA’s are illegal in the state of Oregon – now what? ◦ Each MD gets only ONE room for the entire day ◦ Everything has to be done by the close of day – no work can be carried over to the next day ◦ Our clinic no longer has a waiting room ◦ Our clinic no longer has any receptionists Some of our ideas include: ◦ Patients Register from home or on I-pads in the lobby ◦ Express line for patients who pre-register ◦ MA Swarm ◦ RN triage ◦ Group pre-op classes ◦ Group physical therapy Some of our ideas include: ◦ New patients seen by a PA first – goal is to keep the MD in the OR three days a week ◦ Do totals at our ASC’s with same day discharge (have successfully completed 7 – with 2 more scheduled) ◦ Rapid Access Clinic run by PA’s and they get 50% of the net income 1 hospital 1 IPA 450 physicians 1 Main EMR funded by IPA 4 EMR’s total in community 50 Administrators that have known each other and worked together for as much as 20 years, in short We have established some trust Some of our ideas include: ◦ The specialists “stake” the PCP’s with extra $$ ◦ The $$ are used to hire navigators who call patients to insure they take their meds, comply with care plans and stay out of the ER. ◦ If we save money – savings go 1st to specialists and then are split in the physician community Some of our ideas include: ◦ Establish a one day per week afternoon clinic for low income / high complication patients, staffed by the PCP’s and PA’s from all the specialists. ◦ Rather than force these people to travel all over town by bus, they come to one clinic and can see all of their care providers in one afternoon. Some of our ideas include: ◦ Pay our patients for compliance / results. ◦ $5 gift cards for showing up to the afternoon care clinics. ◦ Collaboration between all of the PCP and specialty clinics. CCO’s v. ACO’s How they Came About Why CCO’s A Driving Force for Change? Preparing for CCO’s CCO’s in Portland v. other parts of Oregon A Passing Fad or the Future? Your options: ◦ Put your head in the sand and hope this will all go away ◦ Retire early – like at 44 ◦ Wait until it is forced upon you, i.e., Oregon ◦ Get ahead of the curve ◦ Learn how to change how you deliver care and reduce your per unit cost now. Experiment with ideas but don’t make global changes quite yet. Think of it this way – if you could lower your cost by 15%, you could afford to: ◦ ◦ ◦ ◦ see Medicaid patients see more patients (improve access) Spend more time with your patients (improve care) And still make the income you do now ◦ At least that’s our premise and what we at Hope Orthopedics are striving to achieve Who knows But think of it this way – if we succeed and lower our costs by 15% and the CCO’s fizzle – have we wasted our time? But if they are here to stay and we have not changed how we deliver care, at all……..