Syncope in the older patient: ECGs you must know
advertisement

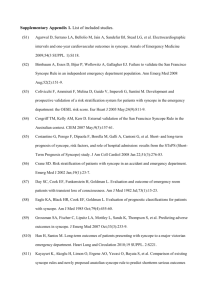
Syncope in the older patient: ECGs you must know Dr Steve W Parry Clinical Senior Lecturer and Honorary Consultant Physician Falls and Syncope Service, Royal Victoria Infirmary and Institute for Ageing and Health, Newcastle University Fig 1 Causes of syncope by age Parry SW, Tan MP BMJ 2010;340:c880 Copyright ©2010 BMJ Publishing Group Ltd. Streamlining and Risk Stratification: Initial Evaluation True syncope from “non-syncopal” disorders Cardiac from non-cardiac syncope Clinical features and basic investigations suggesting a diagnosis or route of referral Basic Evaluation • History – Witness account – Clues to underlying diagnosis • Stokes-Adams presentation • VVS, CSS, OH • Familial sudden death syndromes • Seizures, psychiatric disorders • Subclavian steal, CVD • Examination – Cardiovascular, neurological • 12 lead ECG – Normal: low risk of cardiac syncope – Abnormal: independent predictor of increased mortality • Lying/standing blood pressure measurement Syncope: Certain diagnosis based on symptoms, signs and ECG findings •Classical vasovagal syncope •Precipitating events (fear, pain, emotional distress, instrumentation, prolonged standing) associated with typical prodromal/post event symptoms •Situational syncope •Micturition, defaecation, cough, swallowing •Orthostatic hypotension •Syncope or pre-syncope documented during orthostatic fall in blood pressure Certain diagnosis based on symptoms, signs and ECG findings •Cardiac ischaemia related syncope •Arrhythmia-related syncope •Clear ECG evidence of symptom-rhythm correlation •(Mobitz II, 3rd degree AVB, SVT/VT, sinus pauses >3 sec etc) •Suggestive from history or ECG Brugada syndrome Arrhythmogenic right ventricular dysplasia T inversion in right precordial leads Epsilon waves Ventricular late potentials Ventricular tachycardia Ventricular fibrillation Normal ECG Long QTc QTc= QT/√R-R Torsade de Pointes VT Mobitz I AVB (Wenckebach) Mobitz II AV block Complete heart block Complete heart block Bifascicular block: RBBB with LAFB (LAD broadened QRS) Trifascicular block: RBBB with 1st degree AVB and LAD Sinus node dysfunction with junctional bradycardia Early repolarisation as normal variant Wolff Parkinson White Syndrome PR depression in pericarditis ECG abnormalities suggesting arrhythmic syncope • • • • RBBB, LBBB Very prolonged PR interval Previous MI Chronotropic incompetence – cf trend on 24 hour ECG When is syncope scary? Red flags in transient loss of consciousness • Prolonged unconsciousness, post-event confusion and/or neurological signs, lateral tongue biting • Unheralded syncope with prompt recovery (Stokes Adams attack) or other features suggesting lifethreatening arrhythmias • Family history of premature sudden cardiac or unexplained death • Syncope during exercise • Supine syncope Red flags in transient loss of consciousness • Chest pain, breathlessness • Palpitations preceding syncope • Syncope in patients with heart failure or established heart disease • Frequent and/or injurious syncope • Syncope while driving • ECG abnormalties – Long QTc, SCD, sinus brady <50, broad QRS • Anaemia • Electrolyte imbalance Risk prediction tools • Attempts to quantify risk and identify those at most risk following presentation • Predominantly A&E based and developed • OESIL, EGSYS, Boston Syncope Rule, ROSE rule • San Francisco Syncope Rule (Quinn et al Ann Emerg Med 2004) – Recent meta-analyses and systematic reviews (Serrano et al Ann Emerg Med 2010) suggest SFSR is most promising – Problems in older patients • None have gained wide acceptance • Comparison with clinician best judgement shows equivalent risk prediction (Quinn et al Am J Emerg Med 2005) San Francisco Syncope Rule (Quinn et al Ann Emerg Med 2004, 2006) – – – – History of congestive heart failure Haematocrit <30% Abnormal ECG or cardiac monitoring Systolic BP <90mmHg at triage ROSE (Risk Stratification of Syncope in the ED) (Reed et al EMJ 2007) – – – – – – – BNP >300pg/ml Bradycardia <50 bpm PR exam with faecal occult blood (if GIB suspected) Anaemia Chest pain ECG with q wave Sats <94% on room air