Shobaloju A.G.
OUTLINE:
Intro
Morphology
Adrenal
medulla and function of its hormones
Regulation of adrenal medulla secretion
Biosynthesis of adrenal medullary hormones
Adrenal cortex hormones biosynthesis.
Effects of adrenal androgens and estrogens
Regulation of glucocorticoid and
mineralocorticoid secretion
Physiologic effect of glucocorticoids and
mineralocorticoids
Effects of adrenal cortex hyper or hypo
function.
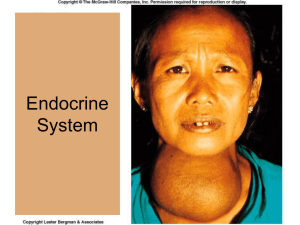
ADRENAL GLAND
INTRODUCTION
2 endocrine organs-adrenal medulla and adrenal
cortex
Adr. medullary hormones...epinephrine,
norepinephrine and dopamine, are not essential for
life, for emergencies.
Adr.cortex hormones are essential for life-secretes
glucocorticoids(cortisol) -- CHO and protein
metabolism.Also mineralocorticoids(aldosterone) -- Na
reabsorption and increase ECF volume,
Sex hormones (androgens and estrogens) -- minimal
effect on reproduction
Adrenocortical secretion is under control of ACTH
but mineralocorticoids secretion also under
independent control by circulating angiotensin II.
ADRENAL MORPHOLOGY
Adrenal
cortex--forms majority of the
ad.gland. Divided into 3 zones:
1) Zona glomerulosa(ZG)-15% of gland
(outer)
2) Zona fasciculata(ZF)-50% of gland
(middle)
3) Zona Reticularis(ZR)-7% of gland. (inner)
The active enzymatic mechanism for
aldosterone synthesis is in the ZG and
that of the sex hormones is present in the
ZR while ZF is for cortisol.
ADRENAL MORPHOLOGY.
Adrenal
medulla—28% of the adrenal
gland.
Interlacing cords of cells that contains
granules.
These cell types secrete—epinephrine and norepinephrine
Dopamine is also secreted by the adrenal
medulla but the cell type is not identifiable.
Adrenal medullary hormones are also known
as catecholamines.
BIOSYNTHESIS OF CATECHOLAMINES
EFFECTS OF EPINEPHRINE
AND NOREPINEPHRINE.
•Their effect is brought about by the action on two
types of receptors and
•They mimic the effect of noradrenergic nervous
discharge.
•Norepinephrine/epinephrine exert metabolic effects
e.g. glycogenolysis in the liver and skeletal muscle.
• plasma lactate, metabolic rate
EFFECTS OF EPINEPHRINE
AND NOREPINEPHRINE (CTD)
•Nor epinephrine causes vasoconstriction of vessels
via 1 receptors
•Nor epinephrine/epinephrine the force of
contraction and rate of contraction by action of the 1
receptors
•Epinephrine dilates the blood vessels in skeletal
muscles and liver via the 2 receptors.
EFFECTS OF DOPAMINE.
The physiologic function of dopamine in
circulation is not known
Has a positive inotropic effect on the heart.
The net effect of moderate doses of dopamine is
an ↑ in systolic pressure and no change in
diastolic pressure.
Catecholamines generally ↑alertness and
myocardial excitability.
ADRENAL CORTEX
Hormones of adrenal cortex are derivatives of
cholesterol
Hormones of Adrenal cortex are known as
steroids.
Include-mineralocorticoids, glucocorticoids and
sex steroids.
BIOSYNTHESIS OF STEROIDS.
Androgen and Estrogen
EFFECTS OF ANDROGENS
Androgens
exert masculinizing effects.
↑ protein metab and growth.
Testosterone from the testes is the most
active androgen.
Secretion of adrenal androgen is
controlled by ACTH.
In adult males,excess adrenal androgens
only accentuate existing characteristics.
In pubertal boys cause precocious puberty.
In females they cause
pseudohermaphroditism.
PHYSIOLOGIC EFFECTS OF
GLUCOCORTICOIDS
Cortisol:
↑ protein catabolism
↑ hepatic gluconeogenesis
↑ G-6-Phosphate activity.
↑ glucose activity
↑ ketone body formation
antagonizes insulin secretion.
permissive action:calorigenic effects of
glucagon
and catecholamines, also for
the
bronchodilatory effects
of catecholamines.
↑ RBC,WBC
helps to cope with stress and also
↑concentration
TRANSPORT AND METABOLISM OF
GLUCOCORTICOIDS
Cortisol
is bound to a protein called transcortin
or corticosteroid-binding globulin.
minor degree of binding to albumin.
Bound steroids are physiologically inactive.
Because of the binding to protein, there is little
free cortisol in the urine.
CBG is synthesized in the liver and its
production is stimulated by estrogen.
TRANSPORT AND METABOLISM OF
GLUCOCORTICOIDS
When
CBG levels↑, more cortisol is bound and
there's reduced free cortisol which stimulates
ACTH and more cortisol is produced until a
new equilibrium is struck.
CBG levels are increased in pregnancy, reduced
in cirrhosis and nephrosis.
Metab of cortisol is in the liver, where most of
the cortisol→ dihydrocortisol →tetrahydro
cortisol which is conjugated to glucoronic acid
by glucoronyl transferase.
PATHOLOGIC EFFECTS OF
GLUCOCORTICOIDS(CORTISOL)
Excess
Cushing's synd
production of cortisol.
2 types-Acth-dependent and Acthindependent.
Acth- independent is caused by glucocorticoid
secreting adrenal tumors
Acth-dependent is caused by Acth-secreting
tumors of anterior pituitary usually called
Cushing's ds and tumors of lungs secreting
Acth.
PRESENTATION OF CUSHINGS SYND
Physiology of the stress response
Catecholamine hormones facilitate immediate physical reactions
associated with a preparation for violent muscular action. These include
the following:
•Acceleration of heart and lung action
•Paling or flushing, or alternating between both
Inhibition of stomach and upper-intestinal action (digestion slows down or
stops)
•General effect on the sphincters of the body
•Constriction of blood vessels in many parts of the body
•Liberation of nutrients (particularly fat and glucose) for muscular action
•Dilation of blood vessels for muscles
•Inhibition of the lacrimal gland (responsible for tear production) and
salivation
•Dilation of pupil (mydriasis)
•Relaxation of bladder
•Evacuation of colon
•Inhibition of erection
•Auditory exclusion (loss of hearing)
•Tunnel vision (loss of peripheral vision)
•Acceleration of instantaneous reflexes
•Shaking
Anti-Inflammatory & Anti-Allergic Effects of
Glucocorticoids•Glucocorticoids inhibit the inflammatory response to tissue injury.
•The glucocorticoids also suppress manifestations of allergic
disease that are due to the release of histamine from tissues.
•Both of these effects require high levels of circulating
glucocorticoids and cannot be produced by administering steroids
without producing the other manifestations of glucocorticoid
excess.(cushings syndrome like effects)
•Large doses of exogenous glucocorticoids inhibit ACTH secretion
to the point that severe adrenal insufficiency can be a dangerous
problem when therapy is stopped.
•However, local administration of glucocorticoids, for example, by
injection into an inflamed joint or near an irritated nerve, produces a
high local concentration of the steroid, often without enough
systemic absorption to cause serious side effects.
The actions of glucocorticoids in patients with
bacterial infections are dramatic but dangerous.
For example, in pneumococcal pneumonia or active
tuberculosis, the febrile reaction, the toxicity, and the
lung symptoms disappear, but unless antibiotics are
given at the same time, the bacteria spread throughout
the body.
It is important to remember that the symptoms are
the warning that disease is present, when these
symptoms are masked by treatment with
glucocorticoids, there may be serious and even fatal
delays in diagnosis and the institution of treatment with
antimicrobial drugs.
Moral of the story-Don’t use steroids just to
relieve symptoms.
EFFECTS OF MINERALOCORTICOIDS
(ALDOSTERONE)
Aldosterone and other steroids with
mineralocorticoid activity ↑ reabsorption of Na
from the kidneys, expanding the ECF vol.
Primarily act on P cells of collecting tubule in
kidney.
Na exchanges for K and H in the renal tubules
producing K diuresis and increased urine acidity.
STIMULI FOR ALDOSTERONE
SECRETION
Glucocorticoid secretion
Surgery
Anxiety
Physical trauma
Hemorrhage
Glucocorticoid secretion
unaffected↑ K
Na intake
Standing
Constriction of the IVC,
Secondary
hyperaldosteronism(ccf,cirrhosis)
REGULATION OF
ALDOSTERONE
SECRETIONRENIN- ANGIOTENSIN
SYSTEM.
ADDISON’S DISEASE
Adrenal
gland not producing enough cortisol
May also involve aldosterone
Also known as adrenal insufficiency or
hypocortisolism
Causes…Disorder of the adrenal glandPrimary adrenal insufficiency /Addisons
disease.
Disorder of ACTH secretion–
Secondary
adrenal insufficiency.
Disorder of CRH from hypothalamus Tertiary adrenal insufficiency.
SYMPTOMS
Chronic
worsening fatigue
Muscle weakness
Loss of appetite
Wt loss
Decreased BP-if persists Addisonian
crisis.
Skin changes…usually areas of
hyperpigmentation over pressure points
Irritability
Depression
PIGMENTATION IN ADDISON'S
DISEASE
DIAGNOSIS
ACTH stimulation test.. Most specific
Addisonian crisis…..
Rx … Hormone replacement.. Steroid tablets..
CONN’S SYNDROME
Is
characterized by overproduction of
mineralocorticoid aldosterone
Caused by Aldosterone-secreting adrenal
adenoma and also Hyperplasia of the
adrenal gland
Aldosterone causes Na and H20 retention
Also causes K excretion in the kidneys
Leading to hypertension
Also known as primary
hyperaldosteronism
SECONDARY ALDOSTERONISM
Secondary aldosteronism due to increase in
Renin levels
E.g.
Decreased bld flow to the kidneys
Decreased blood pressure
Renal artery stenosis
CCF
Cirrhosis
CONN’S SYNDROME CTD
Symptoms include
hypertension
Tetany(Hypocalcemia)
hypokalemic alkalosis
Polyuria
Diagnosis
Adrenal Adenoma – CT scan
QUIZ
a)
b)
c)
d)
Which of the following is expected in a patient
with a gunshot injury to the leg and who has
been bleeding profusely for about an hour
Decreased aldosterone level
Increased aldosterone level
Arteriolar vasodilatation
All of the above
QUIZ
State
the layers of the adrenal glands
What is the effect of cortisol on glucose
Cushing’s syndrome ..Define
State 5 clinical presentation of cushing’s
syndrome.
Conns syndrome.. Define
Pigmentation in addisons disease
Androgens are produced in the adrenal
medulla T/F
17 alpha hydroxylase is contained in the
zona glomerulosa T/F
CONGENITAL ADRENAL HYPERPLASIA
Any
of the severe autosomal recessive
conditions resulting in abnormal steroid
production
Most involve greater or lesser production of sex
steroids
Can alter the dev of primary and secondary
sex characteristics in infants, children
Can be due to 21 hydroxylase deficiency
(commonest cause)
Can also be due to 17 alpha hydroxylase
deficiency
Or 11 hydroxylase deficiency
EFFECTS OF ADRENOCORTICAL
HYPER OR HYPO FUNCTION (CTD)
Primary
hyperaldosteronism e.g. Conn’s synd-Excess mineralocorticoid - K, Na, weakness,
HTN, polyuria.—Adenoma of ZG.
Sec hyperaldosteronism—plasma renin
increased e.g. cirrhosis, heart failure.
Primary Adrenal insufficiency—destroys the
adrenal cortex called Addison's ds-due to
autoimmune ds. Patients lose wt, are tired and
develop severe hypotension.
Secondary adrenal insufficiency—caused by
pituitary disease that Acth secretion
Tertiary adrenal insufficiency is caused by
hypothalamic disorders ( CRH)
EFFECTS OF ADRENAL CORTEX
HYPER OR HYPO FUNCTION..