WIDE QRS COMPLEX TACHYCARDIA
advertisement

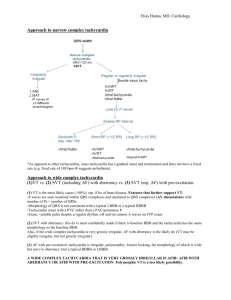
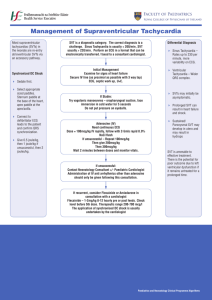
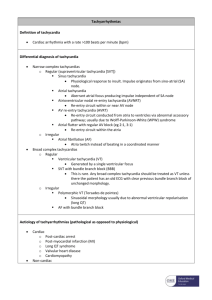
APPROACH TO WIDE QRS COMPLEX TACHYCARDIA Dr HA TUAN KHANH Dr DAVID TRAN Content 1. 2. 3. 4. Definition Causes of WCT Diagnosis criteria Clinical history Physical examination ECG criteria: Brugada criteria, other criteria, findings favoring SVT, VT vs AVRT criteria Management Unstable hemodynamic Stable hemodynamic Definition Wide QRS complex tachycardia is a rhythm with a rate of more than 100 b/m and QRS duration of more than 120 ms SVT (20%) VT (80%) Stewart RB. Ann Intern Med 1986 Causes of wide QRS complex tachycardia • Supraventricular tachycardia - with prexsisting BBB - with BBB due to heart rate (aberrant conduction) - antidromic tachycardia in WPW syndrome • Ventricular tachycardia SVT vs VT Clinical history Age - ≥ 35 ys → VT (positive predictive value of 85%) Underlying heart disease Previous MI → 98% VT Pacemakers or ICD Increased risk of ventricular tachyarrhythmia Medication Drug-induced tachycardia → Torsade de pointes Diuretics Digoxin-induced arrhythmia → [digoxin] ≥2ng/l or normal if hypokalemia SVT vs VT Physical examination Physical findings that indicate presence of AV dissociation (cannon A waves, variable-intensity S1,variation in BP unrelated to respiration) if present are useful Termination of WCT in response to maneuvers like Valsalva, carotid sinus pressure, or adenosine is strongly in-favor of SVT but there are well-documented cases of VT responsive to these SVT vs VT ECG criteria: Brugada algorithm Brugada P. Ciculation 1991 Step 1 Step 2 Step 3 Step 4: LBBB - type wide QRS complex VT SVT R wave >40ms notching of S wave small R wave V1 fast downslope of S wave > 70ms Q wave V6 no Q wave Step 4: RBBB - type wide QRS complex VT SVT rSR’ configuration V1 or R/S > 1 V6 qR (or Rs) complex monophasic R wave R/S ratio < 1 QS complex or Step 4: RBBB morphology Step 4: LBBB morphology Other ECG criteria • North - west QRS axis deviation • Negative or positive concordance • Fusion beats, capture beats • Ventriculoatrial conduction with block • RBBB morphology with LAD > - 300 • LBBB morphology with RAD > + 900 • Previous ECG show MI or previous ECG show that during sinus rhythm, bifascular block is present, which changes in configuration during tachycardia Concordance and Northwest Axis Fusion beat and capture beat Ventriculoatrial conduction with block RBBB morphology with LAD LBBB morphology with RAD Previous MI Previous LBBB Findings favoring SVT • Triphasic pattern in V1 and V6 • Rabbit’s ear • Previous ECG: Preexistent BBB or preexcitation Triphasic pattern Rabbit’s ear Wide complex SVT from preexisting RBBB Wide complex SVT from preexisting LBBB VT vs AVRT ECG criteria Brugada P. Ciculation 1991 Wide complex SVT from bypass tract Summary : diagnosis evaluation ACC/AHA/ESC guidelines for management of pt with SVT. Circulation 2003 Management – Hemodynamic compromise 1. 2. Unstable patient, but still responsible with a discernible BP and/or pulse: - Emergent synchronized cardioversion - If the QRS complex and T wave cannot be distinguished accurately → immediate defibrillation Unstable patient, unresponsive or pulseless → standard ACLS resusciation algorithms ACLS pulseless arrest algorithm AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Ciurculation 2005 Management – Stable hemodynamic 1. VT or WCT of uncertain etiology: Any associated conditions (cardiac ischemia, heart failure, electrolyte abnormalities or drug toxicities) Class I and III antiarrhythmic drugs - Amiodarone: 150mg IV/10mins followed by an infusion of 1mg/min for 6 hours, then 0,5mg/min - Procainamide: 15-18mg/kg infusion over 25-30mins, followed by 1-4mg/min by continuous infusion - Lidocaine: 1-1,5mg/kg IV/2-3mins followed by an infusion of 1-4mg/min Urgent or elective cardioversion Management – Stable hemodynamic 2. SVT Vagal maneuvers: carotid sinus pressure (if no carotid bruits) or Valsava maneuver Adenosine: 6mg over 1-2 seconds. If the initial dose is ineffective, a 12mg dose may be given and repeated once if necessary Calcium channel blocker (Verapamil 2.5 to 5mg IV) or beta blokers (Metoprolol 5 to 10 mg IV) Cardioversion Acute management hemodynamically stable and regular tachycardia ACC/AHA/ESC guidelines for management of pt with SVT. Circulation 2003 Recommendation acute management hemodynamically stable and regular tachycardia ACC/AHA/ESC guidelines for management of pt with SVT. Circulation 2003 Tachycardia algorithm AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Ciurculation 2005 Tachycardia algorithm Thank you for your attention